Case Report: Bone fragment in the third ventricle of a 22 year-old woman
Sunil Munakomi, Balaji Srinivas, Iype Cherian, Andrey Belkin, Alexey Pychteev

TL;DR
A 22-year-old woman had a rare bone fragment in her brain's third ventricle after a severe head injury from a traffic accident.
Contribution
This case report adds to the limited literature on foreign objects in the third ventricle and their clinical outcomes.
Findings
A bone fragment was found in the third ventricle following a compound-depressed skull fracture.
The patient required hormone replacement therapy after surgical removal of the fragment.
The patient ultimately died due to severe traumatic hypothalamic injury.
Abstract
Here we present a very rare case of a woman with a bone fragment in the third ventricle of the brain following compound-depressed skull fractures due to a road traffic accident. There are only few case reports of bullets and textiloma being removed from the third ventricle. Following operative removal of the fragment, the patient was started on cortisol, mineralocorticoid and thyroid hormone replacement. However, the patient eventually died of the severe traumatic hypothalamic insult.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
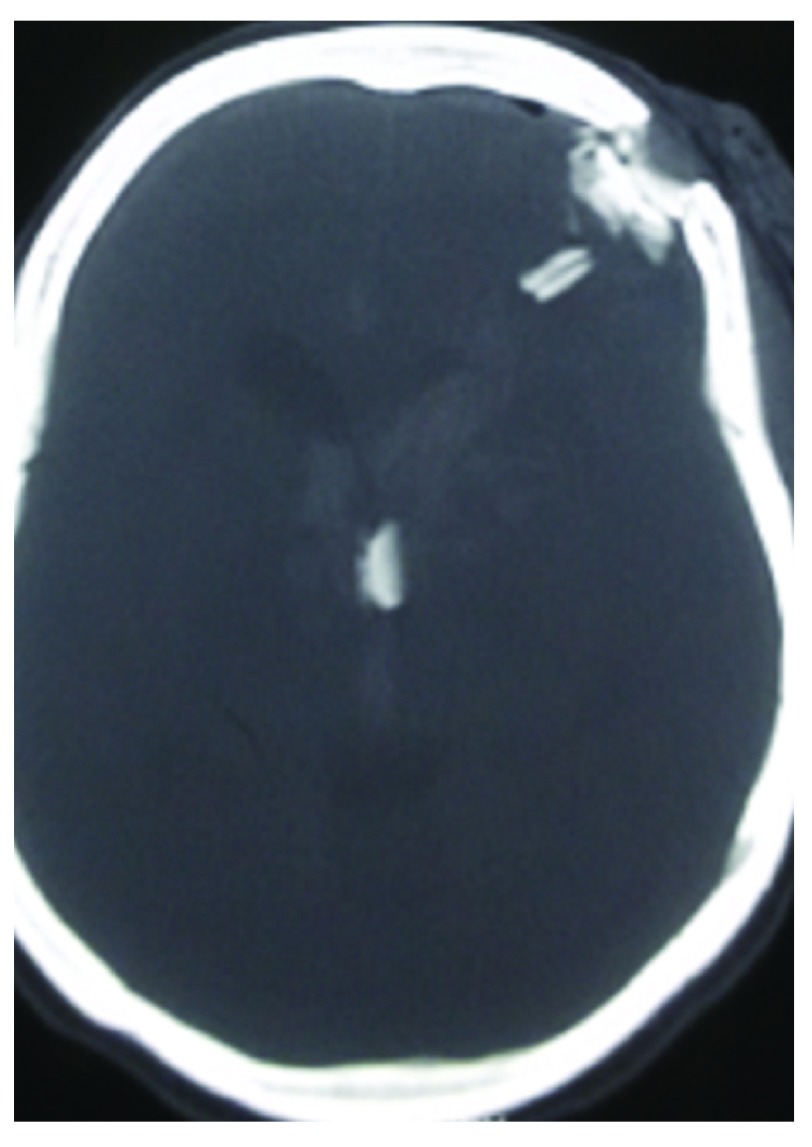 Figure 1
Figure 1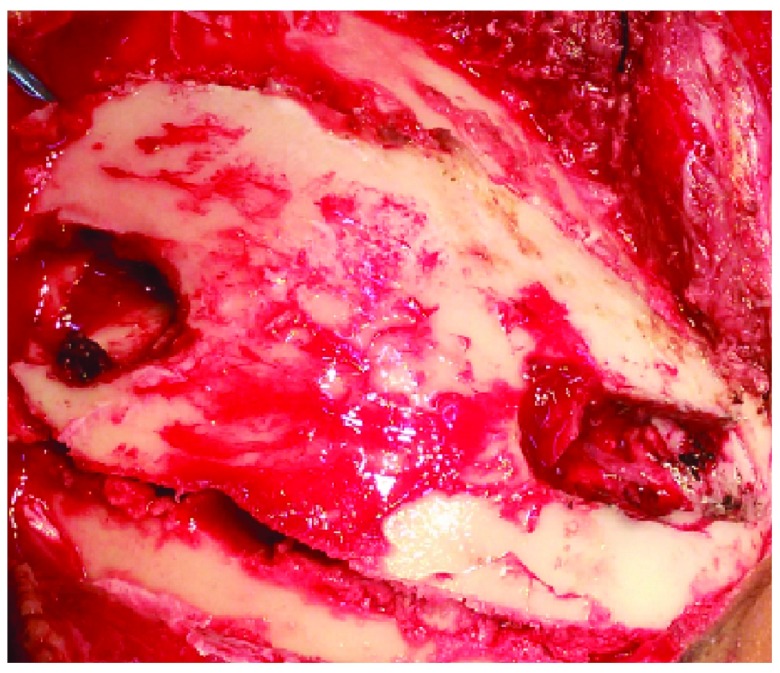 Figure 2
Figure 2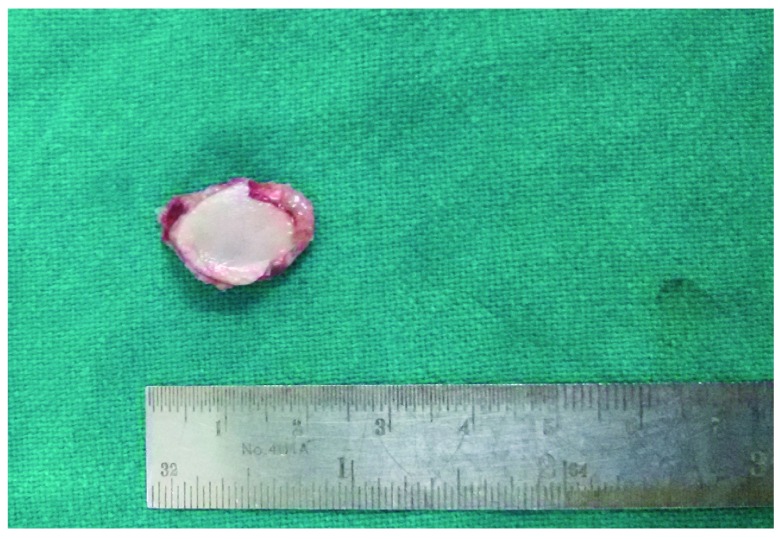 Figure 3
Figure 3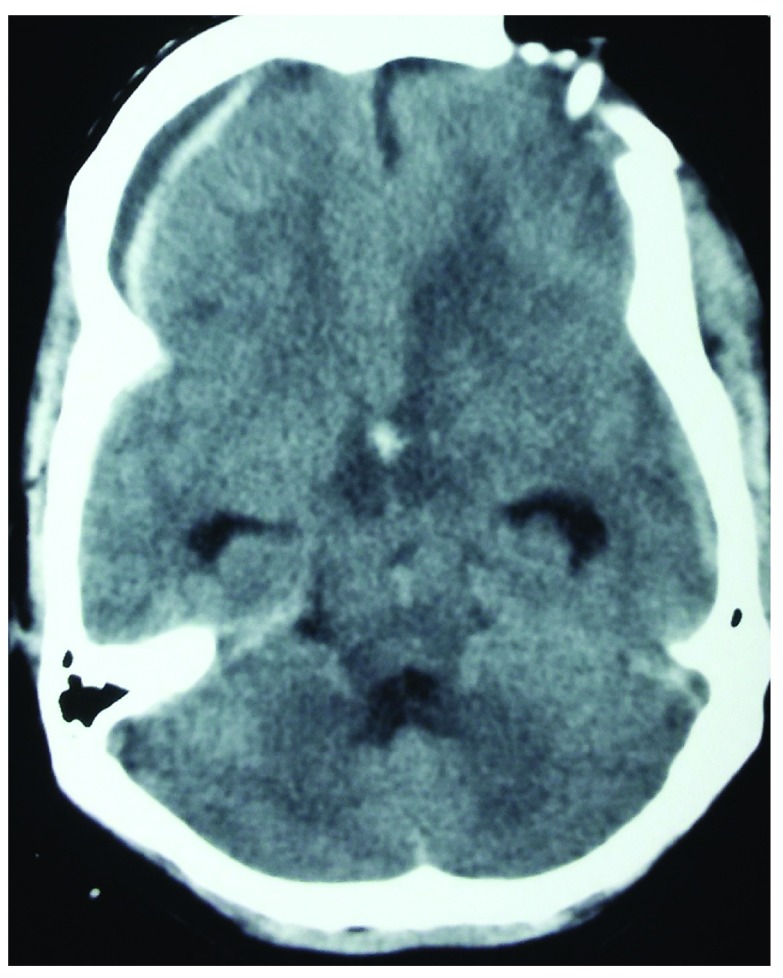 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury and Neurovascular Disturbances · Neurosurgical Procedures and Complications · Cerebrospinal fluid and hydrocephalus
Case report
A 22 year-old female, with no significant past medical and surgical illnesses, was brought to the casualty room with a Glasgow coma scale of 6/15 following a collision between two bikes three hours earlier. Local examination revealed two compound depressed skull fractures in the frontal and the parietal region with egress of brain matter. Following primary resuscitation, computed tomography (CT) of the head confirmed the local findings along with the presence of one bone fragment in the third ventricle ( Figure 1). The patient was taken for debridement of the wound and craniotomy with retrieval of the bone fragment ( Figure 2, Figure 3) following hematoma tracking. Intraventricular drain was placed and neurosurgical intensive care was provided. Repeated CT scans showed hypodensities around the third ventricle ( Figure 4). On the second post-operative day, the patient was started on ionotropic support because of the refractory hypotension, and was also replaced with hydrocortisone, fludrocortisone and thyroid hormones. Wound dressing and the ventricular drain care was continued. Cerebrospinal fluid (CSF) culture from the drain resulted sterile. The patient died on the 8 ^th^ post-operative day because of the traumatic severe hypothalamic insult.
CT image showing the bone fragment lodged in the third ventricle.
Intra-operative picture showing two sites of compound depressed fracture and the craniotomy performed circling both of them.
Image showing the bone fragment retrieved from the third ventricle.
Post-operative image showing evidence of hypodensities surrounding hypothalamic region.
Discussion
As brain abscesses may result from driven bone fragments and other retained foreign bodies in the brain, the removal of readily accessible foreign bodies has received much attention ^3– 6^. Migration of foreign bodies can occur because of gravitational force. Other routes of migration can be subdural, parenchymal, transventricular or along streamlining along the white matter track ^7^. The removal of foreign bodies is mostly done via craniotomy ^8, 9^, but other methods such as burr hole, stereotaxy ^10^ and sometimes by ventriculoscopy ^11^ have also been described.
The goals of modern treatments include removal of the foreign body under a controlled environment in the neurosurgical operation setting. Surgical principles include removal of bone fragments, intracerebral hematoma, control of hemorrhages and prevention of further loss of neural tissue. Patients should receive a broad spectrum intravenous antibiotic therapy along with tetanus prophylaxis. Monitoring and control of elevated intracranial pressure with maintenance of cerebral perfusion pressure plays a significant role in the patient’s survival and outcome. The follow-up of such patients is essential, considering known complications like cerebrospinal fluid fistula in the early post-operative period and brain abscesses and seizures which may occur years after injury. Outcome after a penetrating head injury is directly related to the Glasgow coma scale at the time of presentation, which is the reflection of the extent of brain tissue damage caused directly by the primary impact. Intensive post-operative monitoring of intracranial pressure, cardio-respiratory function and metabolic status are required for optimizing the outcome of victims of penetrating craniocerebral injuries ^12^. Penetrating head injuries have a higher mortality and morbidity than blunt trauma even in a civilian set up ^13^. Even after timely removal of the penetrating objects and intensive medical management, the outcome may remain poor.
Consent
Informed written consent for publication of images and clinical details was obtained from the patient’s husband.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Greenwood J Jr: Removal of foreign body (bullet) from the third ventricle. J Neurosurg.1950;7(2):169–72. 10.3171/jns.1950.7.2.0169 15405323 · doi ↗ · pubmed ↗
- 2Lavrnic S Stosic-Opincal T Gavrilovic S: Intraventricular textiloma with granuloma formation following third ventricle colloid cyst resection - a case report. Cent Eur Neurosurg.2009;70(2):86–8. 10.1055/s-2008-1081506 19711261 · doi ↗ · pubmed ↗
- 3Carey ME Young H Mathis JL: A bacteriological study of craniocerebral missile wounds from Vietnam. J Neurosurg.1971;34(2 Pt 1):145–154. 10.3171/jns.1971.34.2part 1.0145 14768680 · doi ↗ · pubmed ↗
- 4Hagan RE: Early complications following penetrating wounds of the brain. J Neurosurg.1971;34(2 Pt 1):132–141. 10.3171/jns.1971.34.2part 1.0132 14768678 · doi ↗ · pubmed ↗
- 5Hammon WM: Analysis of 2187 consecutive penetrating wounds of the brain from Vietnam. J Neurosurg.1971;34(2 Pt 1):127–131. 10.3171/jns.1971.34.2part 1.0127 14768677 · doi ↗ · pubmed ↗
- 6Hammon WM: Retained intracranial bone fragments: analysis of 42 patients. J Neurosurg.1971;34(2 Pt 1):142–144. 10.3171/jns.1971.34.2part 1.0142 14768679 · doi ↗ · pubmed ↗
- 7Rengarchy SS Carey M Templer J: The Sinking Bullet. J Neurosurg.1992;30(2):291–294. 10.1097/00006123-199202000-00029 1545906 · doi ↗ · pubmed ↗
- 8Campbell WP Howard WO Weary WB: Gunshot wounds of the brain. Report of two unusual complications: bifrontal pneumocephalus and a loose bullet in the lateral ventricle. Arch Surg.1942;44(5):789–798. 10.1001/archsurg.1942.01210230013002 · doi ↗