Silent but present: a case of Chagas disease-related megaoesophagus diagnosed in a non-endemic setting
Virginia Donini, Anna Barbiero, Michele Spinicci, Fabio Marra, Francesco Vizzutti, Damiano Bisogni, Gian Maria Rossolini, Francesca Malentacchi, Lorenzo Zammarchi, Alessandro Bartoloni

TL;DR
A case of Chagas disease-related megaoesophagus is reported in a non-endemic country, emphasizing the need for awareness in at-risk migrants.
Contribution
Highlights the first reported case of CD-related megaoesophagus in a non-endemic setting in Europe.
Findings
CD-related megaoesophagus can occur in non-endemic countries due to migration.
The patient had lived in Italy for 14 years before diagnosis, showing the disease's silent progression.
The case underscores the importance of considering CD in at-risk individuals with gastrointestinal symptoms.
Abstract
Due to migration phenomena, Chagas disease (CD) is emerging in Europe, where CD-related gastrointestinal complications are rarely reported. We describe a case of CD-related megaoesophagus in a patient from El Salvador, in Italy since 14 years, highlighting the importance of considering complicated CD in patients at risk with suggestive symptoms.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
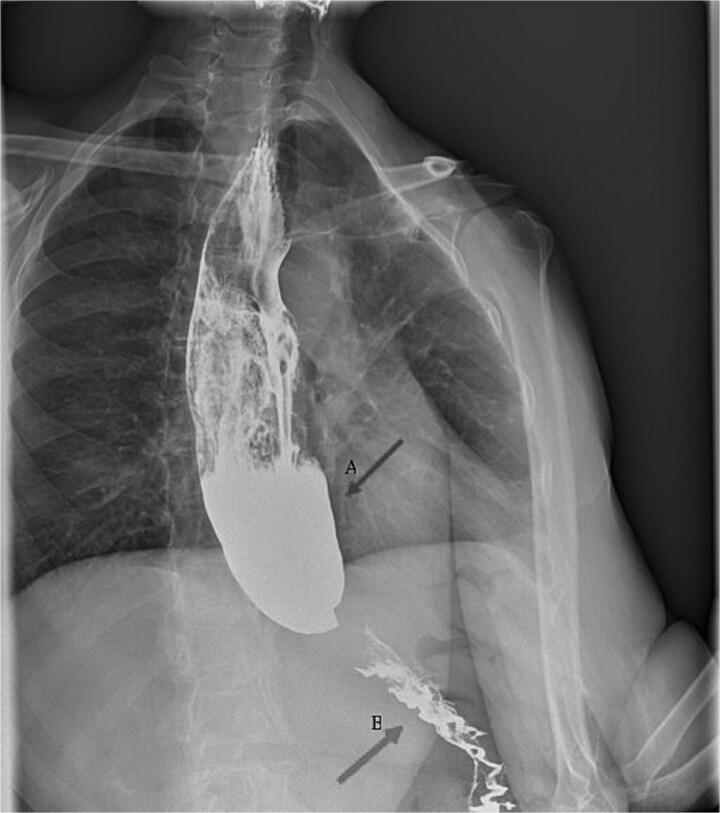 Figure 1
Figure 1- —Università degli Studi di Firenze within the CRUI-CARE Agreement
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrypanosoma species research and implications · Gastroesophageal reflux and treatments · Whipple's Disease and Interleukins
Introduction
Chagas disease (CD), a neglected tropical disease caused by the flagellate protozoa Trypanosoma cruzi, is primarily transmitted by Hemiptera insects, but can also be transmitted vertically, through blood and organ donation and, more rarely, the oral route.1
CD is endemic in continental Latin America and in some areas of the USA. In Europe, where the vector is not present, most cases are recorded in migrants from CD-endemic areas mostly living in Spain, Italy, Portugal, Sweden, Switzerland and the Netherlands.2
Following acute infection, if left untreated, CD progresses to a chronic phase with development of cardiac, digestive or neurological involvement in 30–40% of infected persons within 10–30 years, leading to increased morbidity and mortality.3
Case description
A 63-year-old woman from El Salvador, living in Italy for 14 years and with no known comorbidities, presented with aggravating dysphagia and weight loss (17 kg) since September 2023. The patient’s mother had cardiological problems since an early age and died at 45 of sudden death.
After multiple assessments, including a normal oesophagogastroduodenoscopy, a barium swallow X-ray in January 2024 demonstrated a dyscalasic megaoesophagus (Figure 1). The patient tested positive at the Western-Blot and chemiluminescent immunoassay (CMIA) serology for T. cruzi, confirming the diagnosis of chronic CD with gastrointestinal involvement. T. cruzi PCR on peripheral blood resulted negative.
Barium swallow X-ray (January 2024) showing dilatation of the oesophagus (arrow A) and a tapered narrowing at the oesophagogastric junction (‘bird-beak sign’) (arrow B).
In April 2024, the patient underwent a peroral endoscopic myotomy (POEM). After this procedure, she had a progressive improvement in her ability to feed with solid food and she gained 10 kg.
Cardiological evaluation and Holter electrocardiography were normal, as well as endoscopic and radiographic studies of the colon.
Following recovery after POEM, after a thorough discussion with the patient on the risks and benefits related to specific antiparasitic treatment, on 25 November 2024 she was started on benznidazole 150 mg bid, concluded after 60 days with no major adverse events. Approximately 10 days after initiating therapy, she developed a mildly itching cutaneous rash that did not require treatment interruption. At her most recent follow-up in May 2025, she remained in good clinical condition.
Conclusion
This report underlines the importance of always suspecting CD in patients coming from endemic areas with gastrointestinal and/or cardiological symptoms; its prompt recognition would not only favour adequate clinical evaluation and management but would be essential to enable early treatment and limit chronic sequelae.
According to recent reviews, CD is estimated to affect over 100 000 individuals in Europe, with digestive involvement likely present in 9–21% of cases but rarely being reported.4 Estimates for migrant populations and country-specific prevalence data remain highly variable and likely underestimated2; in Spain, where the South American population is highly represented among immigrants, travellers and visiting friends and relatives, CD represented about one third of the diagnoses made on these groups.5 The adoption of spread and systematic screening policies in high-risk populations would be the key to reduce underdiagnosis rates of CD in Europe.
However, despite representing a relevant health issue for the affected population, Chagas disease-related gastrointestinal complications are rarely reported in the European setting, and in general this condition has received considerably less attention in terms of clinical and epidemiological aspects, compared to Chagas related-cardiac involvement.6
Untreated Chagas-related megaoesophagus is associated with a poor prognosis; however, timely POEM can reduce complications and achieve clinical success rates exceeding 90%; some studies have shown that POEM is an effective and safe treatment for Chagasic achalasia.7^,^8
Trypanocidal therapy is not strongly recommended for patients over 50 years of age with organ damage. However, in the described case, it was recommended to prevent cardiac involvement and/or reactivation during eventual future immunosuppression. Due to limited evidence regarding its efficacy in older patients with gastrointestinal involvement, treatment decisions should be individualized in such cases.9^,^10
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chagas Disease. PAHO/WHO | Pan American Health Organization, 2024. https://www.paho.org/en/topics/chagas-disease (18 May 2025, date last accessed).
- 2Strasen J, Williams T, Ertl G, Zoller T, Stich A, Ritter O. Epidemiology of Chagas disease in Europe: many calculations, little knowledge. Clin Res Cardiol 2014;103:1–10. 10.1007/s 00392-013-0613-y. · doi ↗
- 3Pérez-Molina JA, Molina I. Chagas disease. Lancet. 2018;391:82–94. 10.1016/S 0140-6736(17)31612-4.28673423 · doi ↗ · pubmed ↗
- 4Antinori S, Galimberti L, Bianco R, Grande R, Galli M, Corbellino M. Chagas disease in Europe: a review for the internist in the globalized world. Eur J Intern Med 2017;43:6–15. 10.1016/j.ejim.2017.05.001.28502864 · doi ↗ · pubmed ↗
- 5Alkaissy Y, Serre-Delcor N, Arsuaga Vicente M et al. Trends in imported infections among migrants and travellers to Spain: a decade of analysis through the +Redivi network. J Travel Med 2024;31:taae 067. 10.1093/jtm/taae 067.38691427 · doi ↗ · pubmed ↗
- 6Pinazo MJ, Lacima G, Elizalde JI et al. Characterization of digestive involvement in patients with chronic T. Cruzi infection in Barcelona, Spain. P Lo S Negl Trop Dis 2014;8:e 3105. 10.1371/journal.pntd.0003105.25144648 PMC 4140677 · doi ↗ · pubmed ↗
- 7Dantas RO . Management of esophageal dysphagia in Chagas disease. Dysphagia. 2021;36:517–22. 10.1007/s 00455-021-10297-1.33855597 · doi ↗ · pubmed ↗
- 8Farias GFA, de Moura DTH, de Moura ETH et al. Peroral endoscopic myotomy (POEM): a comparative study between Chagasic and idiopathic achalasia. Endosc Int Open 2020;8:E 506–12. 10.1055/a-1035-9288.32258372 PMC 7089801 · doi ↗ · pubmed ↗