Case Report: A case of giant left ventricular aneurysm resulting in LAD compression and stenosis
Qun Wang, Longyu Li, Wenhua Lin

TL;DR
A 67-year-old man with heart failure had a large left ventricular aneurysm that compressed a heart artery, showing how such aneurysms can actively cause new heart problems.
Contribution
This case highlights the rare complication of a giant left ventricular aneurysm causing dynamic coronary artery compression and emphasizes the role of advanced imaging in diagnosis.
Findings
A giant left ventricular aneurysm caused dynamic mid-LAD stenosis through extrinsic compression.
Multimodal imaging confirmed extensive scar tissue covering 69% of the left ventricle.
The case illustrates a feedback loop of ischemia and ventricular remodeling due to the aneurysm.
Abstract
We present the case of a 67-year-old male smoker who developed progressive heart failure despite successful primary PCI for an acute extensive anterior ST-elevation myocardial infarction. Initial echocardiography revealed an apical left ventricular aneurysm (LVA). Readmission 40 days later showed dramatic ventricular dilation, severely reduced LVEF (19%), and a large inferoapical aneurysm. Multimodality imaging was pivotal: repeat angiography demonstrated a new dynamic mid-LAD stenosis; IVUS confirmed extrinsic luminal compression without plaque; CMR and nuclear scintigraphy quantified extensive scar (69% of LV). This comprehensive workup excluded conventional causes and established a diagnosis of external mechanical compression of the mid-LAD by the expanding giant LVA, creating a vicious cycle of ischemia and remodeling. This case underscores that an LVA is not merely a passive scar…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
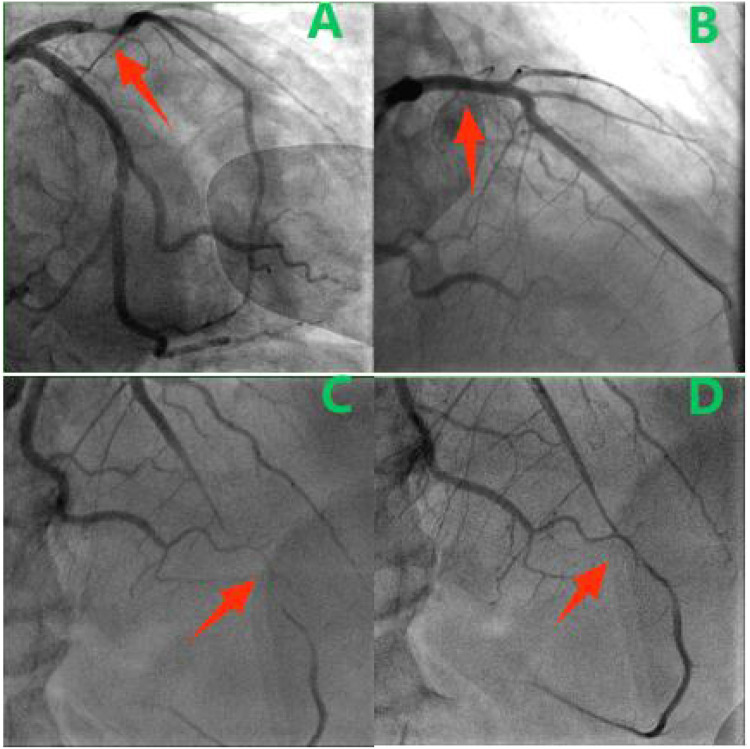 Figure 1
Figure 1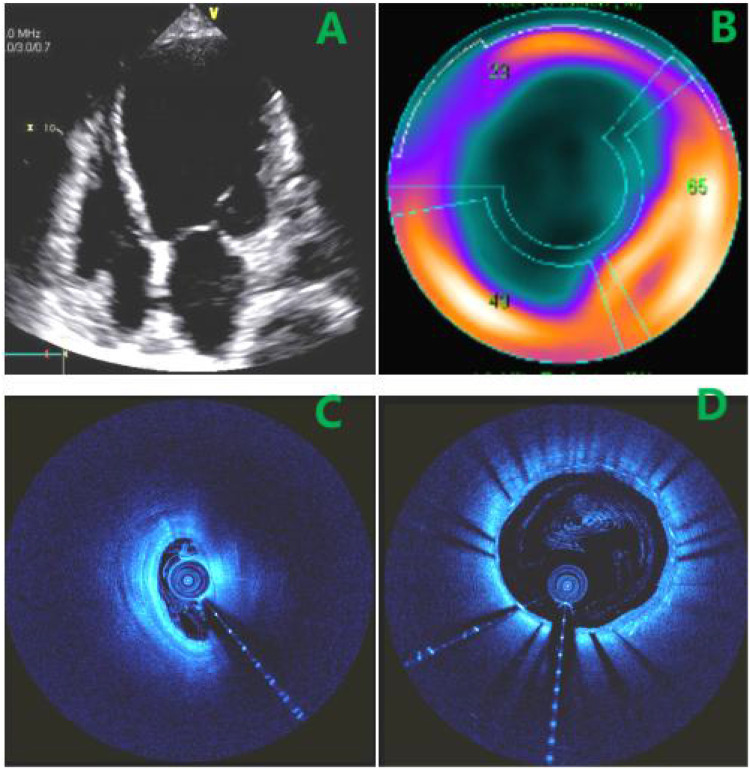 Figure 2
Figure 2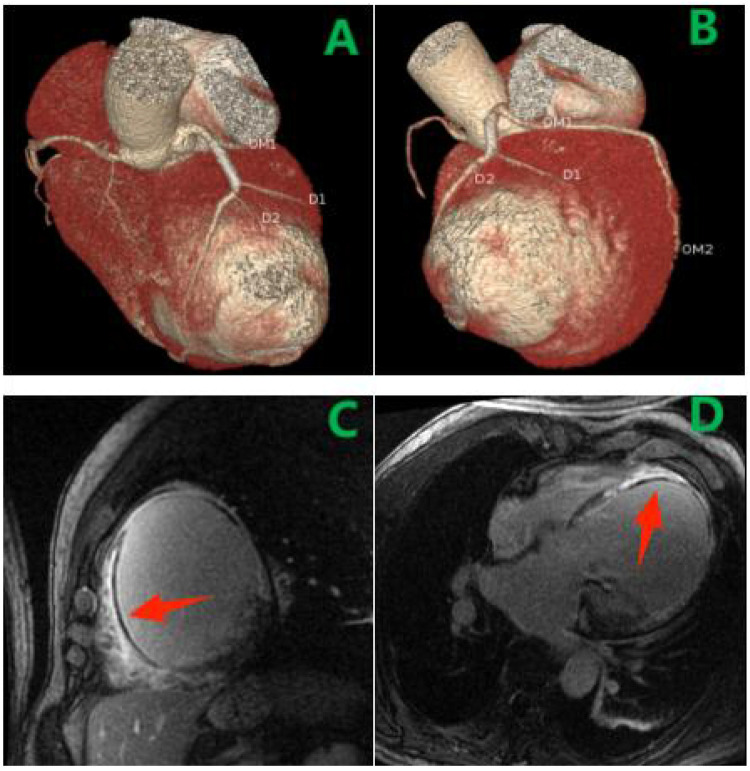 Figure 3
Figure 3| Timepoint | Event | Key findings/interventions |
|---|---|---|
| Day 1 | Presentation | Chest pain, ECG anterior STEMI, elevated biomarkers. |
| Day 1–5 | Initial Management | Antiplatelet, anticoagulation, heart failure therapy. |
| Day 5 | PCI | Proximal LAD 95% stenosis stented. |
| Day 7 Discharge | LVEF 43%, on guideline-directed medications. | |
| ∼40 days post-discharge | Readmission | Worsening heart failure, LVEF 19%,CAG: new mid-LAD dynamic stenosis. |
| Readmission period | Advanced Imaging | IVUS, CTA, CMR performed confirming aneurysm compression. |
| Treatment Decision | Surgery recommended but declined. Medical therapy continued. | |
| 1-year | Follow-up | Aneurysm stable, NYHA II-III, reduced quality of life. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Pericarditis and Cardiac Tamponade · Cardiovascular Effects of Exercise
Introduction
Case report
A 67-year-old man presented with a five-day history of intermittent chest pain. He had a significant smoking history (40 pack-years) and denied hypertension or diabetes. Physical examination revealed bilateral basal lung crackles. Cardiac auscultation indicated a regular rhythm without murmurs, and there was no peripheral edema. Admission electrocardiography showed sinus rhythm with pathological Q waves and ST-segment elevation in leads V1–V6. Laboratory findings included elevated BNP (1,840 pg/mL), CK-MB (10.6 ng/mL), myoglobin (150 ng/mL), troponin I (17.5 ng/mL), and D-dimer (1,070 ng/mL). Echocardiography revealed left ventricular dilation (LVEDd 53 mm), reduced systolic function (LVEF 42%), hypokinesis of the interventricular septum and left ventricular free wall, an apical left ventricular aneurysm (LVA), and diastolic dysfunction. A diagnosis of acute extensive anterior myocardial infarction was established.
The patient received antiplatelet therapy and guideline-directed medical therapy for heart failure. On hospital day 5, coronary angiography demonstrated a critical 95% segmental stenosis in the proximal left anterior descending artery (LAD) (Figure 1A), a 70% focal stenosis in the mid left circumflex artery, and patent left main and right coronary arteries. A 4.0 × 23 mm drug-eluting stent was successfully deployed in the proximal LAD (Figure 1B). Post-procedurally, the patient was angina-free. Follow-up echocardiography before discharge showed LVEDd 57 mm and LVEF 43%. Discharge medications included aspirin 100 mg daily, ticagrelor 90 mg twice daily, atorvastatin 20 mg daily, ramipril 1.25 mg daily, spironolactone 20 mg daily, and metoprolol tartrate 12.5 mg twice daily.
(A) Initial CAG showing stenosis (arrow) in the proximal LAD. (B) After stent placement. (C,D) Diastolic (C) and systolic (D) views showing dynamic mid-LAD compression (arrow).
Approximately 40 days after discharge, the patient was readmitted with progressive heart failure symptoms (dyspnea on ordinary exertion). Physical examination revealed basal lung crackles and an enlarged cardiac dullness border, without peripheral edema. Electrocardiography was unchanged. BNP had increased to 2,524 pg/mL. Echocardiography showed marked left ventricular dilation (LVEDd 62 mm), severely reduced LVEF (19%), a large mid-to-inferior left ventricular wall aneurysm, and moderate mitral regurgitation (Figure 2A). Repeat coronary angiography revealed a patent proximal LAD stent but a new diffuse 95% stenosis in the mid-LAD segment (Figures 1C,D). The stenosis exhibited dynamic phasic variation, unresponsive to intracoronary nitroglycerin. Myocardial bridging was excluded by review of angiograms. Intravascular ultrasound (IVUS) confirmed stent patency and showed a cyclically compressed, slit-like lumen in the mid-LAD segment without significant plaque (Figures 2C,D).
(A) large LV aneurysm on echo. (B) Perfusion scan:extensive scar (blue), minimal viable myocardium (red). (C) IVUS showing compressed mid-LAD lumen. (D) IVUS demonstrated patency of the stent in the proximal LAD.
Coronary computed tomography angiography (CTA) confirmed a giant left ventricular aneurysm and delineated its spatial relationship to the LAD (Figures 3A,B). Cardiac magnetic resonance imaging, including cine imaging (FIESTA sequence) for function and late gadolinium enhancement (PSIR sequence) for tissue characterization, revealed extensive fibrosis and microvascular obstruction in the anterior, lateral, septal, and apical segments of the left ventricle (Figures 3C,D). Myocardial perfusion scintigraphy revealed a scar involving approximately 69% of the left ventricular area (Figure 2B).
(A,B) CTA: giant aneurysm adjacent to LAD. (C,D) CMR LGE confirmed microvascular obstruction (MVO) within the apical septal subendocardial infarct (arrow).
The cause of the new mid-LAD stenosis was systematically evaluated. Significant atherosclerosis progression was considered unlikely given the minimal plaque burden on IVUS. In-stent restenosis was excluded by IVUS confirmation of proximal stent patency. Coronary artery spasm was deemed improbable due to the lack of response to intracoronary nitroglycerin, and myocardial bridging was ruled out by careful angiographic review. Ultimately, the convergence of findings—dynamic phasic narrowing on angiography, extrinsic compression on IVUS, and the anatomic adjacency of the aneurysm to the LAD on CTA—collectively supported the diagnosis of external vascular compression by the expanding ventricular aneurysm.
Stenting the compressed segment was deemed high-risk. Therefore, surgical aneurysm resection with CABG was recommended but declined by the patient. He was managed with optimized guideline-directed medical therapy. At one-year follow-up, the patient reported persistent heart failure symptoms (NYHA class II-III). Repeat echocardiography showed the aneurysm was stable in size, but global LV function remained severely impaired (LVEF ∼20%). He had no further hospitalizations for acute heart failure but reported a reduced quality of life. The timeline of the clinical course and management is presented in Table 1.
Discussion
LVA is a common cardiac complication following myocardial infarction. Among patients with acute transmural MI who did not receive reperfusion therapy, approximately 30%–35% develop significant LVA (1). About 85% of these cases occur in the anterior wall or apex, frequently associated with occlusion of the left anterior descending artery—a region where the thinner myocardial structure and relatively poor blood supply increase susceptibility to aneurysmal formation (1). With the widespread use of primary percutaneous coronary intervention, the incidence of LVA has declined markedly in recent years, with current estimates below 5% (2).
LVA represents the end-stage morphological manifestation of post-infarction ventricular remodeling. Pathologically, it results from the replacement of transmural infarcted myocardium by fibrous scar tissue, leading to a persistent, paradoxical bulging of the ventricular wall (1). The remodeling process unfolds in two phases: the early phase, beginning 24–72 h after infarction, involves inflammatory infiltration, cardiomyocyte slippage, and acute expansion of the infarct zone; the late phase, spanning weeks to months, is characterized by fibroblast activation, collagen deposition, and scar maturation. This progression varies considerably among individuals (3). Several factors influence remodeling severity, with anterior wall MI conferring a 1.9-fold higher risk than other infarct locations (4), and multi-vessel disease increasing risk by 1.2-fold compared to single-vessel involvement (5). Systemic inflammation and associated growth factors are central drivers of this process (3); notably, soluble suppression of tumorigenicity 2 (sST2) has been implicated in infarct zone inflammation and is closely linked to myocardial fibrosis and remodeling progression (6).
Giant LVA is now infrequently encountered in clinical imaging, and documented cases of coronary artery compression by an LVA—impairing myocardial perfusion—are rarer still. These uncommon presentations underscore the need to reappraise the clinical implications of LVA. Beyond the conventional risks of thromboembolism, wall motion abnormalities, and heart failure, LVA can initiate a self-perpetuating cycle: myocardial ischemia → ventricular remodeling/LVA formation → coronary compression → recurrent ischemia. This vicious circle significantly elevates the risk of reinfarction, malignant arrhythmias, and sudden cardiac death.
In this particular case of giant LVA, aside from established risk factors such as delayed reperfusion, extensive smoking history, and significant left anterior descending artery disease, the adequacy of pharmacotherapy must be considered. Renin–angiotensin–aldosterone system inhibitors and beta-blockers require careful uptitration to evidence-based target doses, and appropriate diuretic use may mitigate remodeling by reducing ventricular volume load. Additionally, cardiac magnetic resonance revealed extensive microvascular obstruction—a known companion of epicardial reperfusion that may perpetuate ischemic injury and adverse remodeling; thus, strategies to improve microvascular perfusion warrant attention (7). Although this patient declined surgery, LVA resection combined with left ventricular reconstruction remains a well-established curative option for suitable candidates (8).
Emerging molecular targets offer future therapeutic potential. Preclinical studies suggest that inhibiting lysozyme 2 (Lyz2) helps preserve the cardiac extracellular matrix, attenuates scar formation, and improves function (9). Similarly, modulation of the MIAT–DHX9 axis may ameliorate the remodeling microenvironment by regulating abnormal vascular smooth muscle cell activity (10). These approaches target fundamental pathways in fibrosis and inflammation and, though not yet translated to clinical practice, represent promising research directions.
In summary, contemporary understanding frames post-infarction LVA not as a mere passive scar, but as a dynamic, mechanically disruptive entity that actively promotes disease progression. Early recognition and multidisciplinary strategies to disrupt its vicious cycle are essential to improving outcomes, and they reinforce the pathophysiological rationale for surgical intervention in advanced cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sattar Y Alraies MC. Ventricular Aneurysm. (2025).32310415 · pubmed ↗
- 2O'Gara PT Kushner FG Ascheim DD Casey DE Jr Chung MK de Lemos JA 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology foundation/American Heart Association task force on practice guidelines. Circulation. (2013) 127(4):e 362–425. 10.1161/CIR.0b 013e 3182742 c 8423247304 · doi ↗ · pubmed ↗
- 3Yalta K Yilmaz MB Yalta T Palabiyik O Taylan G Zorkun C. Late versus early myocardial remodeling after acute myocardial infarction: a comparative review on mechanistic insights and clinical implications. J Cardiovasc Pharmacol Ther. (2020) 25(1):15–26. 10.1177/107424841986961831416353 · doi ↗ · pubmed ↗
- 4Zaliaduonyte-Peksiene D Simonyte S Lesauskaite V Vaskelyte J Gustiene O Mizariene V Left ventricular remodelling after acute myocardial infarction: impact of clinical, echocardiographic parameters and polymorphism of angiotensinogen gene. J Renin Angiotensin Aldosterone Syst. (2014) 15(3):286–93. 10.1177/147032031247122823283822 · doi ↗ · pubmed ↗
- 5Tarantini G Napodano M Gasparetto N Favaretto E Marra MP Cacciavillani L Impact of multivessel coronary artery disease on early ischemic injury, late clinical outcome, and remodeling in patients with acute myocardial infarction treated by primary coronary angioplasty. Coron Artery Dis. (2010) 21(2):78–86. 10.1097/MCA.0b 013e 328335 a 07420071979 · doi ↗ · pubmed ↗
- 6Marino R Magrini L Orsini F Russo V Cardelli P Salerno G Comparison between soluble ST 2 and high-sensitivity troponin I in predicting short-term mortality for patients presenting to the emergency department with chest pain. Ann Lab Med. (2017) 37(2):137–46. 10.3343/alm.2017.37.2.13728029000 PMC 5203991 · doi ↗ · pubmed ↗
- 7Aldujeli A Tsai TY Haq A Tatarunas V Knokneris A Briedis K Impact of coronary microvascular dysfunction on functional left ventricular remodeling and diastolic dysfunction. J Am Heart Assoc. (2024) 13(9):e 033596. 10.1161/JAHA.123.03359638686863 PMC 11179865 · doi ↗ · pubmed ↗
- 8Lawton JS Tamis-Holland JE Bangalore S Bates ER Beckie TM Bischoff JM. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. (2022) 145(3):e 18–e 114. 10.1161/CIR.000000000000103934882435 · doi ↗ · pubmed ↗