Advanced pancreatic ductal adenocarcinoma with liver metastases treated with multimodal therapy: a case report
Lei Cao, Bin Liu, Jinheng Liu, Hongwei Wu, Mulan Zhong

TL;DR
A 54-year-old man with advanced pancreatic cancer and liver metastases was successfully treated with a combination of therapies, leading to improved survival and quality of life.
Contribution
This case report demonstrates the effectiveness of a multimodal MDT strategy in treating advanced PDAC with liver metastases.
Findings
The patient's liver metastases significantly decreased in size after treatment.
CA19–9 levels dropped from 4141.57 U/mL to 58.64 U/mL.
Overall survival exceeded 15 months with good quality of life.
Abstract
To investigate the therapeutic efficacy and survival benefits of a multidisciplinary team (MDT) strategy, including local interventional therapy, systemic chemotherapy, and immunotherapy, for patients with advanced pancreatic ductal adenocarcinoma (PDAC) presenting with liver metastasis at initial diagnosis. A 54-year-old male patient was diagnosed with PDAC in the tail of the pancreas with multiple intrahepatic metastases (cT3N1M1, stage IV). The patient underwent multimodal comprehensive treatment, including iodine-125 seed implantation at the pancreatic primary site, eight cycles of hepatic arterial infusion chemotherapy, PD-L1 inhibitor (Benmelstobart), and oral S-1 maintenance therapy. After treatment, the patient’s liver metastases significantly decreased in size (partial response according to RECIST 1.1), CA19–9 levels dropped from 4141.57 U/mL to 58.64 U/mL, overall survival…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
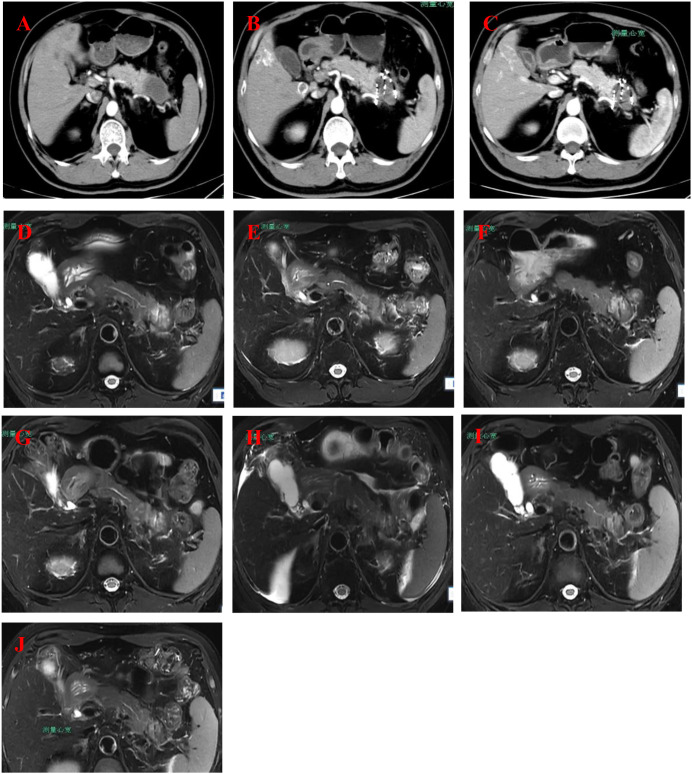 Figure 1
Figure 1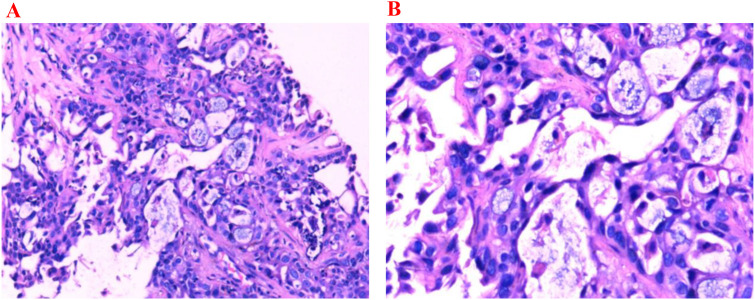 Figure 2
Figure 2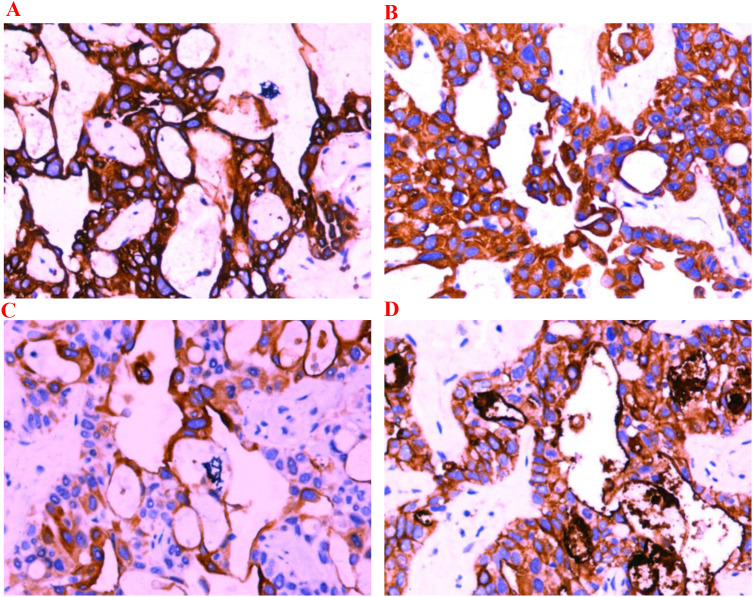 Figure 3
Figure 3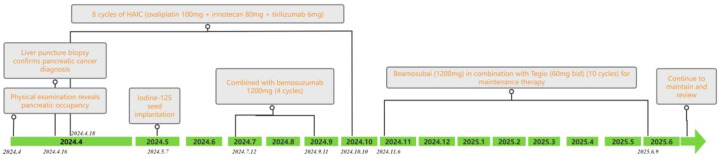 Figure 4
Figure 4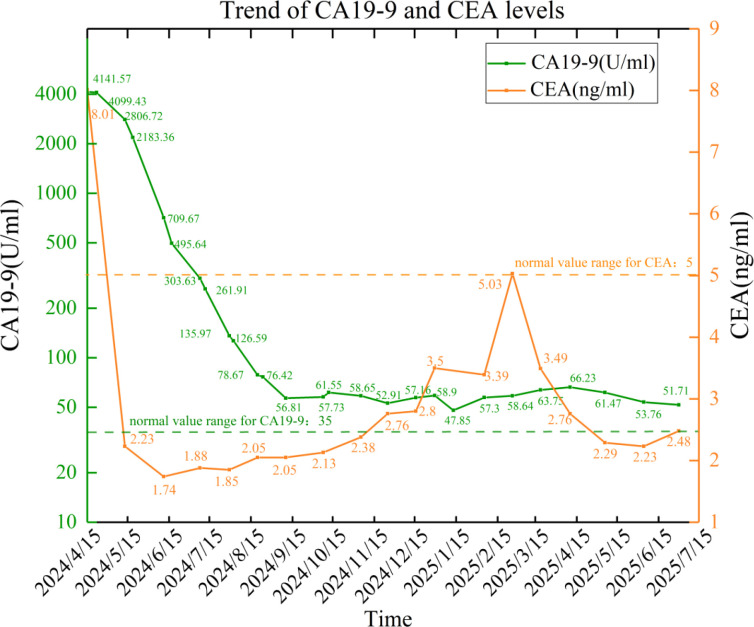 Figure 5
Figure 5| Date | Examination/treatment item | Key findings/procedure details | Clinical significance/treatment response | CA199 (U/mL) |
|---|---|---|---|---|
| 2024-04-04 | Abdominal contrast-enhanced CT, Brain MRI | - Pancreatic tail mass (suspected malignancy); Multiple liver metastases; Enlarged lymph nodes in the pancreatic head region | Initial findings suggestive of pancreatic cancer with liver metastases | – |
| 2024-04-15 | Laboratory tests | Significant elevation of CA199 | Tumor activity marker | 4141.57 |
| 2024-04-18 | Hepatic arteriography + drug perfusion (Cycle 1) | First interventional therapy | Good postoperative recovery, preliminary control of liver metastases | – |
| 2024-05-07 | Iodine-125 seed implantation (external hospital) | Local radiotherapy intervention | Local control of the primary lesion | – |
| 2024-05-13 | Upper abdominal contrast-enhanced CT/MRI, Lab tests | - CT: Post-particle implantation changes; Shrinking liver metastases; Abnormal enhancement in left kidney (metastasis to be ruled out) | Partial remission post interventional therapy + particle implantation | 2806.72 |
| 2024-05-16 | Hepatic artery perfusion (Cycle 2) | Second interventional therapy | Continued control of liver metastases | – |
| 2024-06-11 | Upper abdominal contrast-enhanced CT/MRI, Lab tests | - CT: Progressive shrinkage of liver metastases; Irregular left kidney contour | Marked therapeutic response | 709.67 |
| 2024-06-14 | Hepatic artery perfusion (Cycle 3) | Third interventional therapy | Maintenance of therapeutic efficacy | – |
| 2024-07-11 | Hepatic artery perfusion (Cycle 4) | Fourth interventional therapy | – | – |
| 2024-07-12 | Bemotuzumab immunotherapy (Cycle 1) | Initiation of maintenance immunotherapy | Enhanced systemic control through combination therapy | – |
| 2024-07-30 | Laboratory tests | CA199 approaching normal range | Stable disease status | 78.67 |
| 2024-08-01 | Hepatic artery perfusion (Cycle 5) | Fifth interventional therapy | – | – |
| 2024-08-21 | Upper abdominal contrast-enhanced MRI | - Stable pancreatic lesion size | First indication of splenic vein complications | – |
| 2024-08-22 | Hepatic artery perfusion (Cycle 6) | Sixth interventional therapy | – | – |
| 2024-09-12 | Hepatic artery perfusion (Cycle 7) | Seventh interventional therapy | – | – |
| 2024-10-09 | Upper abdominal contrast-enhanced MRI, Lab tests | - Splenic vein collateral circulation formation | Long-term stability | 56.81 |
| 2024-10-10 | Hepatic artery perfusion (Cycle 8) | Eighth interventional therapy | Completion of interventional therapy cycles | – |
| 2024-11-06 | Bemotuzumab immunotherapy (Cycle 2) | Continuation of immunotherapy | – | – |
| 2024-11-25 | Upper abdominal contrast-enhanced MRI | - Slight shrinkage of liver metastases | Local progression (ascites suggests potential peritoneal metastasis) | 58.65 |
| 2024-12-16 | Upper abdominal contrast-enhanced MRI | - Stable pancreatic lesion | Requires monitoring of fluid changes | 57.16 |
| 2025-01-13 | Upper abdominal contrast-enhanced MRI | - Slight enlargement of pancreatic tumor | Disease progression (primary lesion enlargement + systemic fluid accumulation) | 58.90 |
| 2025-02-05 | Upper abdominal contrast-enhanced MRI | - Reduced pleural effusion after absorption | Improvement following supportive care (diuretics + anti-infection) | 57.30 |
| 2025-02-26 | Upper abdominal contrast-enhanced MRI, Lab tests | - Reduced marginal enhancement of pancreatic tumor | Possible reduction in tumor activity | 58.64 |
| Date | Event/management |
|---|---|
| 2024-12-18 | Received anti-tumor treatment |
| 2024-12-30 | Experienced grade III myelosuppression; administered 150 μg of human granulocyte colony-stimulating factor and 3 mg of interleukin-11 |
| 2024-12-31–2025-1-8 | Received 300 μg of granulocyte colony-stimulating factor and 3 mg of interleukin-11 |
| 2025-1-9–2025-1-14 | Received 300 μg of granulocyte colony-stimulating factor |
| 2025-2-26 | Received anti-tumor treatment |
| 2025-3-19 | Experienced grade III myelosuppression |
| 2025-3-19–2025-3-21 | Received 300 μg of granulocyte colony-stimulating factor |
| 2025-3-22 | Received 6 mg of pegylated recombinant human granulocyte colony-stimulating factor |
| 2025-3-25–2025-3-26 | Received 3 mg of interleukin-11 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Cholangiocarcinoma and Gallbladder Cancer Studies · Hepatocellular Carcinoma Treatment and Prognosis
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is one of the most aggressive solid tumors. Approximately 80% of PDAC patients are diagnosed with locally advanced or distant metastasis, with a median survival of less than 12 months and a 5-year survival rate of less than 10% (1). For metastatic PDAC patients, the prognosis is even worse, with a median survival of less than 6 months and a 5-year survival rate of less than 1% (2). Although traditional chemotherapy regimens (such as FOLFIRINOX and gemcitabine plus nab-paclitaxel) can improve the prognosis of some patients to a certain extent, the overall efficacy is still limited, and drug resistance often occurs (3).
In recent years, with the continuous development of interventional therapy, immunotherapy, and molecular targeted drugs, the multidisciplinary comprehensive treatment (MDT) strategy for PDAC has gradually gained attention. For example, radioactive seed implantation can enhance local control of the primary tumor (4); hepatic arterial infusion chemotherapy (HAIC) can significantly increase the drug concentration in liver metastases (5); and immune checkpoint inhibitors (such as PD-1/PD-L1 inhibitors) can enhance antitumor immune responses by modulating the tumor microenvironment (6). However, how to integrate these treatment modalities into an efficient and safe individualized treatment plan and ultimately extend the survival of patients with advanced PDAC remains a major challenge in current clinical practice.
This article reports a case of advanced PDAC with liver metastasis at initial diagnosis, who achieved long-term survival through a multimodal comprehensive treatment strategy, including iodine-125 seed implantation, HAIC, PD-L1 inhibitors, and oral S-1. This case aims to explore the potential value of MDT in advanced PDAC and provide useful references for the clinical management of such patients.
Case presentation
The patient is a 54-year-old male who was admitted to the hospital on April 4, 2024, due to a “pancreatic mass detected during a physical examination.” He had a history of hypertension for more than 10 years, well controlled with irbesartan and amlodipine besylate, with no other significant past medical history, and no known family history of malignancy. Enhanced CT scan of the whole abdomen revealed a mass in the tail of the pancreas (approximately 4.9 cm × 3.0 cm × 2.7 cm) with multiple liver metastases and enlarged peripancreatic lymph nodes (Figure 1A), with no signs of other distant metastases. Laboratory tests on April 15, 2024, showed a significant elevation in serum CA19–9 levels, reaching 4141.57 U/mL. Pathological results from ultrasound-guided liver mass biopsy confirmed pancreatic ductal adenocarcinoma (Figure 2). Immunohistochemical tests on April 16, 2024, showed positive results for CK7, CK19, CK20, and CA125 (Figure 3). The patient was clinically staged as cT3N1M1 (stage IV).
Medical imaging progress of pancreatic and liver conditions. (A) (2024-4-4): CT scan of the abdomen showing pancreatic tail mass, suspected as a malignant tumor, with liver metastasis and enlarged lymph nodes. (B) (2024-5-13): MRI scan of the abdomen depicting a pancreatic tail tumor, with signs of liver metastasis, gallbladder inflammation, and possible kidney involvement. (C) (2024-6-11): CT and MRI showing unchanged pancreatic mass with metastatic liver lesions, mild gallbladder inflammation, and lymphadenopathy. (D) (2024-8-21): MRI scan highlighting the pancreatic mass, possible splenic vein thrombosis, and multiple liver lesions showing no significant change. (E) (2024-10-9): MRI of the abdomen showing a stable pancreatic mass with continued liver metastasis and a possible inflammatory process in the kidneys. (F) (2024-11-25): MRI scan showing pancreatic tumor with minimal changes, continued liver metastases, and moderate kidney abnormalities. (G) (2024-12-16): MRI showing unchanged pancreatic tumor, suspected splenic vein involvement, and stable liver lesions with mild gallbladder inflammation. (H) (2025-1-13): MRI showing slight growth in pancreatic tumor, stable liver metastases, and increased abdominal fluid accumulation. (I) (2025-2-5): MRI depicting stable pancreatic mass, unchanged liver metastases, and decreased pleural fluid. (J) (2025-2-26): MRI showing slight reduction in the edge enhancement of the pancreatic tumor, with stable liver metastases and mild pleural effusion.
Histopathological images stained with hematoxylin and eosin (H&E). (A) (H&E ×100) shows deeply stained nuclei (high chromatin) with variable size and shape (pleomorphism). (B) (H&E ×200) reveals cells arranged in glandular patterns, with some areas showing dense cell clusters forming solid cords or irregular glandular lumens; nuclei are significantly enlarged with an increased nuclear-to-cytoplasmic ratio; cytoplasm is moderate to scanty and eosinophilic; cell arrangement is disordered with partial loss of polarity.
Immunohistochemistry (×200). (A) CK7 positive; (B) CK19 positive;(C) CK20 positive; (D) CA125 positive.
From April 2024 to February 2025, the patient underwent multidisciplinary comprehensive treatment, with the specific treatment plan and timeline shown in Table 1, Figure 1, and Figure 4.
Timeline of treatments and investigations.
Local interventional therapy
In May 2024, the patient underwent iodine-125 seed implantation at the pancreatic primary site. Follow-up imaging showed stable size of the primary lesion with dense deposition of multiple seeds within.
Systemic treatment
The patient completed eight cycles of hepatic arterial infusion chemotherapy (HAIC) (oxaliplatin 100 mg + irinotecan 80 mg + tirilizumab 6 mg), combined with Benmelstobart (1200 mg per dose, intravenous infusion, infusion time 60 min per dose, every 3 weeks for a total of four cycles). Subsequently, the patient entered the maintenance treatment phase, with a regimen of Benmelstobart combined with oral S-1 (60 mg per dose, twice daily, continuous administration for 21 days followed by a 14-day break, for a total of 10 cycles).
Supportive care
On December 18, 2024, the patient received anti-tumor therapy. On December 30, 2024, he experienced grade III myelosuppression due to chemotherapy, with decreased white blood cells and platelets, and was managed with subcutaneous granulocyte colony-stimulating factor (G-CSF) and interleukin-11. The patient received further anti-tumor therapy on February 26, 2025. Subsequently, the patient experienced a second episode of grade III myelosuppression on March 19, 2025, which was managed with supportive care including G-CSF, pegylated recombinant human G-CSF, and interleukin-11 subcutaneously (Table 2).
During follow-up, the patient’s tumor markers significantly improved. CA19–9 levels decreased from the baseline of 4141.57 U/mL to 58.64 U/mL in June 2025, while CEA remained within the normal range. The dynamic changes are shown in Figure 5. Imaging assessment revealed a 45% reduction in the sum of the longest diameters of liver metastases (partial response according to RECIST 1.1 criteria), with the pancreatic primary lesion remaining stable (Figure 1B). As of July 2025, the patient’s overall survival had reached 15 months, with an ECOG performance status of 1 and no signs of disease progression.
Trend of CA19–9 levels (U/ml) and CEA (ng/ml) levels.
Discussion
This case describes an advanced PDAC patient who achieved an overall survival of 15 months following a combination treatment strategy involving iodine-125 seed implantation, HAIC, PD-L1 inhibitors, and S-1. Currently, standard systemic therapy for metastatic PDAC primarily comprises FOLFIRINOX or gemcitabine-based regimens, with reported median overall survival ranging from 6.7 to 11.1 months. By comparison, at the time of data cutoff, the patient in this case had achieved an overall survival exceeding 15 months. At the most recent follow-up, the overall survival was approximately 21 months, accompanied by a favorable quality of life. These findings suggest that a multimodal treatment strategy may offer additional clinical benefit in selected patients. The individualized therapeutic approach was applied in real-world clinical practice and may provide an important reference for the multidisciplinary comprehensive treatment of advanced PDAC. The analysis is now unfolded from three dimensions: synergistic mechanisms of treatment, technological innovation and safety control, and dynamic monitoring and precision treatment.
In this patient, a sequential therapeutic strategy was implemented, beginning with HAIC to control liver metastases, followed by iodine-125 seed implantation for sustained local tumor control, and subsequently combined with immunotherapy and maintenance therapy. Iodine-125 seed implantation, as a form of precision radiotherapy, may exert anti-tumor effects through dual mechanisms. On one hand, its continuous low-dose radiation can potentially induce double-strand breaks in tumor cell DNA within the effective range. In this case, the primary lesion remained stable for 11 months after the procedure, which is broadly consistent with the reported local control rate of 85.71% in the literature (7). On the other hand, seed implantation may also have a radiosensitizing effect. Studies suggest that irradiation at 6 Gy combined with 30 nM gemcitabine can significantly upregulate the Bax/Caspase-3 pathway, increasing the apoptosis rate of PANC-1 cells to 41.2% (8). HAIC may additionally enhance drug delivery to liver metastases through a “first-pass effect,” with floxuridine exposure in the liver reaching 6–8 times that of systemic chemotherapy (9). In this case, a 45% reduction in liver metastases was observed, which roughly aligns with the 66.1% objective response rate (ORR) in the combination treatment group. The sequential treatment model of HAIC → seed implantation → PD-L1 inhibitor could potentially stimulate anti-tumor immune responses through a series of chain reactions, including promoting antigen release, enhancing antigen presentation, and T-cell recognition.
In terms of technological application and safety, the 3D-printed coplanar template technique significantly enhances the precision of seed implantation. It achieves a target V100 of 91.17% while keeping the duodenal irradiation dose below 45 Gy (10), effectively avoiding severe complications. In this case, there were no occurrences of pancreatic fistula or perforation, which is consistent with reports that the template technique reduces the incidence of severe complications to less than 5% (11). HAIC also demonstrates advantages in terms of safety. Studies have shown that the mFOLFOX regimen can reduce total bilirubin levels by 46.56% in patients with hyperbilirubinemia (12), with hematological toxicity primarily consisting of grade 1–2 events (12). HAIC also demonstrated acceptable safety in this patient, enabling continuation of subsequent systemic therapy over a relatively long course.
From the perspective of dynamic monitoring and treatment guidance, the 98.6% reduction in CA19–9 levels in this case is consistent with the characteristics of a treatment-sensitive population (patients with a reduction of >50% within 3 months have an OS of 14.2 months) (13). A comprehensive multidimensional monitoring system should also include parameters from multiple categories such as inflammation-nutrition indicators, molecular features, and radiomics. For example, patients with serum albumin ≥3.5 g/dL and CRP <0.3 mg/dL have a 62% lower risk of disease progression (14); patients with a KRAS mutation abundance reduction of over 30% have a 3.5-fold increase in response rate to S-1 therapy (15). The dynamic changes in the CT values of the primary lesion in this case also reflect the biological effects of the continuous radiation from the seeds, which is associated with dosimetric features of V100>90%. These observations indicate that integrated dynamic monitoring may help inform treatment adjustment and response evaluation in patients undergoing multimodal therapy.
As a single case report, these findings do not replace evidence from prospective clinical trials but indicate the potential feasibility of a multidisciplinary, multimodal treatment strategy in selected patients with advanced PDAC. The observed outcomes suggest that a tripartite treatment framework integrating “local control, systemic clearance, and immune activation” should be further developed. It is recommended that future research focus on the following areas: First, the development of a dynamic prognostic model incorporating ctDNA clearance rate to achieve more precise efficacy assessment; second, in-depth exploration of the mechanism by which S-1 enhances the immune therapeutic effect by downregulating COL1A1; and third, optimization of the spatiotemporal combination strategy of seed implantation and HAIC to enhance treatment synergy. This case underscores the potential value of a multidisciplinary, multimodal approach in advanced PDAC and may serve as a practical reference for developing individualized treatment plans in the future.
Conclusion
This case, through a multidisciplinary comprehensive treatment strategy, including the combination of iodine-125 seed implantation, HAIC, PD-L1 inhibitors, and S-1, enabled a patient with advanced PDAC and liver metastasis to achieve an overall survival of more than 15 months, demonstrating good clinical benefits.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rompianesi G Loiaco G Rescigno L Benassai G Giglio MC Campanile S . A systematic review of indications and clinical outcomes of electrochemotherapy in pancreatic ductal adenocarcinoma. Cancers. (2025) 17. 408 doi: 10.3390/cancers 17030408, PMID: 39941777 PMC 11816056 · doi ↗ · pubmed ↗
- 2Chakrabarti S Kamgar M Mahipal A . Systemic therapy of metastatic pancreatic adenocarcinoma: current status, challenges, and opportunities. Cancers. (2022) 14. 2588 doi: 10.3390/cancers 14112588, PMID: 35681565 PMC 9179239 · doi ↗ · pubmed ↗
- 3Mastrantoni L Chiaravalli M Spring A Beccia V Di Bello A BagalàC . Comparison of first-line chemotherapy regimens in unresectable locally advanced or metastatic pancreatic cancer: a systematic review and Bayesian network meta-analysis. Lancet Oncol. (2024) 25:1655–65. doi: 10.1016/s 1470-2045(24)00511-4, PMID: 39542008 · doi ↗ · pubmed ↗
- 4Dai F Wang J An H Lei T Tang K Ma X . Therapy of (125)I particles implantation inhibited the local growth of advanced non-small cell lung cancer: a retrospective clinical study. Am J Transl Res. (2019) 11:3737–49. PMC 661464031312384 · pubmed ↗
- 5Laface C Laforgia M Molinari P Ugenti I Gadaleta CD Porta C . Hepatic arterial infusion of chemotherapy for advanced hepatobiliary cancers: state of the art. Cancers. (2021) 13. 3091 doi: 10.3390/cancers 13123091, PMID: 34205656 PMC 8234226 · doi ↗ · pubmed ↗
- 6Retecki K Seweryn M Graczyk-Jarzynka A Bajor M . The immune landscape of breast cancer: strategies for overcoming immunotherapy resistance. Cancers. (2021) 13. 6012 doi: 10.3390/cancers 13236012, PMID: 34885122 PMC 8657247 · doi ↗ · pubmed ↗
- 7Ji L Zhang W Hao S Wang Z Ding T Zhang G . Percutaneous transhepatic cholangial drainage combined with intra-tumoral iodine-125 seeds implantation and chemotherapy for locally progressive pancreatic head cancer with obstructive jaundice. J Contemp Brachytherapy. (2022) 14:462–9. doi: 10.5114/jcb.2022.121563, PMID: 36478703 PMC 9720689 · doi ↗ · pubmed ↗
- 8Li Q Li Y Liu J Huang X Li Z . Synergistic effects of (125)I seed implantation brachytherapy and gemcitabine in pancreatic tumors. Discov Med. (2024) 36:1464–76. doi: 10.24976/Discov.Med.202436186.136, PMID: 39054717 · doi ↗ · pubmed ↗