A Comprehensive Analysis of Dermatological Manifestations in Lower Limb Para-Athletes
Andre Aabedi, Vera Wang, Devendra K. Agrawal

TL;DR
This paper examines skin issues in athletes with lower limb prostheses, identifying causes and prevention strategies, and highlights new technologies to improve skin health and performance.
Contribution
The paper provides a comprehensive review of skin complications in lower limb para-athletes and evaluates emerging technologies for prevention and management.
Findings
Skin complications affect 34%-77% of lower limb prosthesis users, especially athletes.
Poor prosthetic fit, high activity, and environmental factors are key risk factors for skin issues.
New technologies like smart prosthetics and antimicrobial coatings show promise but need more research.
Abstract
In this article, a critical evaluation of current evidence is presented on the prevalence, mechanisms, prevention, and management of sport-related skin complications in amputee athletes using lower limb prostheses, highlighting emerging technologies aimed at improving skin health and athletic performance. Skin complications were highly prevalent, affecting 34%-77% of lower limb prosthesis users, with even greater frequency among athletes. The most common conditions included maceration, friction blisters, pressure ulcers, contact dermatitis, verrucous and epidermal hyperplasia, and bacterial or fungal infections. Key risk factors encompassed poor prosthetic fit, elevated activity levels, increased perspiration, prolonged wear, inadequate hygiene, and hot or humid environments. Mechanical loading and shear stress at the socket–skin interface, compounded by moisture and heat retention,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
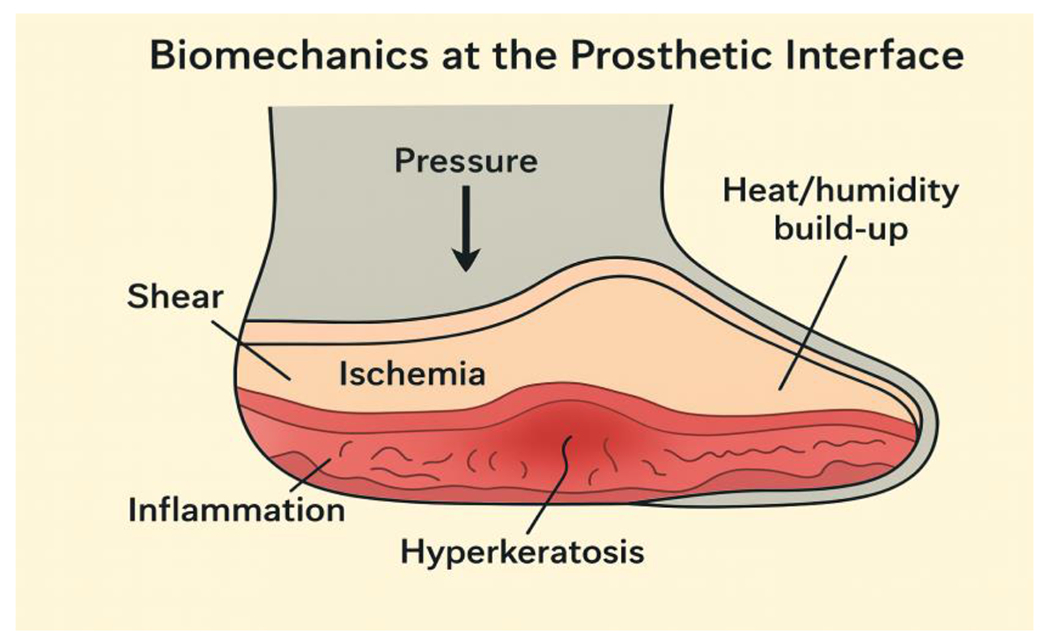 Figure 1
Figure 1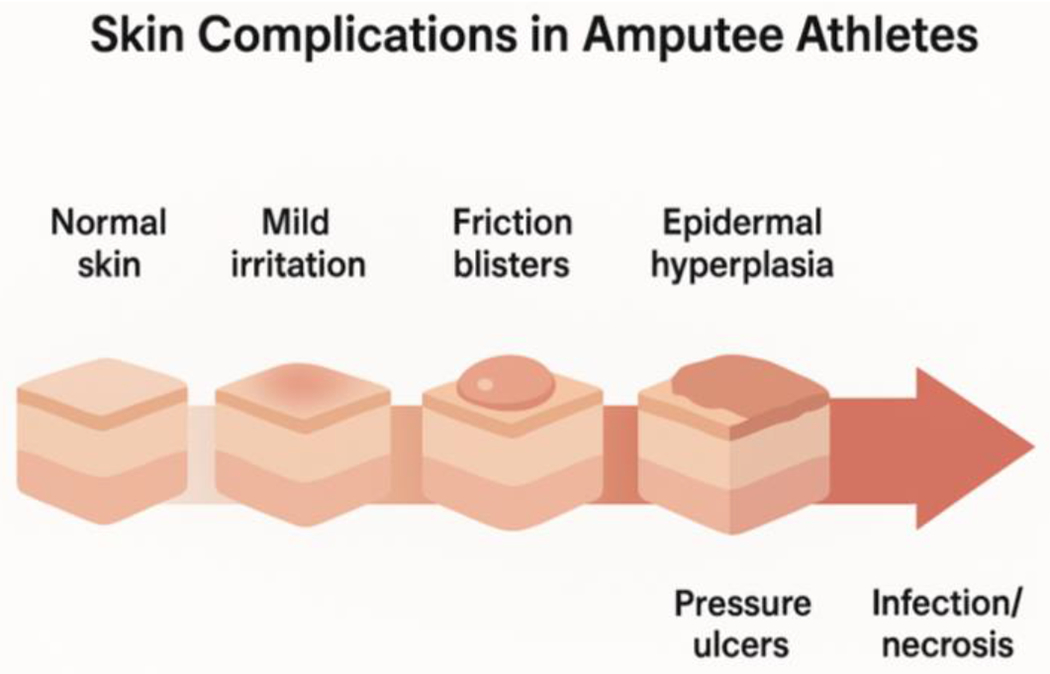 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNail Diseases and Treatments · Skin Diseases and Diabetes · Cutaneous lymphoproliferative disorders research
Introduction
Skin complications represent a significant challenge for amputee athletes using lower limb prostheses, arising from the distinctive mechanical and environmental stresses imposed during athletic activity. The prosthetic socket-skin interface experiences repetitive friction, shear forces, and elevated humidity levels that collectively predispose athletes to various dermatologic conditions [1]. These complications can interrupt prosthesis use, compromise athletic performance, and substantially diminish quality of life [2].
Common cutaneous manifestations include maceration, friction blisters, pressure ulcers, allergic contact dermatitis, epidermal hyperplasia, hyperhidrosis, and bacterial or fungal infections [3]. The prevalence of skin problems among lower limb amputees is notably high—studies report rates approaching 70% in general amputee populations—and may be elevated further in athletes due to heightened activity levels and perspiration [3]. Ill-fitting prostheses, suboptimal socket design, and prolonged wear during sports substantially amplify these risks [4]. Allergic reactions to prosthetic materials and liners have also been documented, with patch testing identifying causative allergens in a considerable proportion of affected individuals.
Sport-specific prostheses, though engineered to enhance performance, may paradoxically introduce additional cutaneous risks when improperly fitted or inadequately maintained. Effective prevention hinges on meticulous skin care protocols, routine residual limb inspection, optimal prosthetic fitting, and timely management of incipient skin changes [5]. Multidisciplinary care integrating dermatology, rehabilitation medicine, and prosthetists is critical for early detection and intervention, thereby minimizing complications and sustaining athletic participation. Despite the high prevalence and clinical impact of these complications, additional research is warranted to characterize sport-specific risk factors and establish evidence-based prevention strategies for this population [6]. This critical review is a comprehensive analysis of the types, causes, prevention, and management of sport-related skin complications in lower-limb prosthesis users.
Method
A comprehensive literature search was conducted across PubMed, Scopus, Embase, and SPORTDiscus databases using combinations of the terms “lower limb amputation,” “prosthesis,” “athlete,” “sports,” and “skin complications.” Peer-reviewed studies published in English within the past two decades were included if they examined cutaneous outcomes in lower limb prosthesis users engaged in athletic or high-activity contexts. Data were extracted on epidemiology, risk factors, complication types, preventive strategies, and technological innovations.
Overview of Skin Biomechanics in Prosthesis Use
The residual limb skin of amputee athletes using prostheses experiences distinctive mechanical loading patterns—including pressure, shear, and friction—that can fundamentally alter normal skin physiology and trigger cutaneous complications. Mechanical loading induces deformation of skin and underlying soft tissues, initiating cellular and microvascular changes with clinically significant consequences. Sustained or repetitive pressure and shear forces at the prosthetic socket interface compromise local perfusion, precipitating ischemia and elevating the risk of ulceration and tissue necrosis [7]. Shear stresses are particularly implicated in both deep tissue injury and superficial lesions, as they distort dermal and subcutaneous architecture, disrupting microcirculation and promoting inflammatory cascades [8].
At the cellular level, mechanical forces activate mechanotransduction pathways in keratinocytes, fibroblasts, and other resident skin cells, triggering dysregulated cytokine release, sustained inflammation, and compromised regenerative capacity. Chronic mechanical stress can induce compensatory hyperkeratosis and epidermal hyperplasia, with severe cases progressing to cellular necrosis or aberrant differentiation [9]. The skin’s biomechanical response demonstrates considerable heterogeneity, modulated by individual factors including baseline vascular integrity, pre-existing skin condition, and the local microenvironment—particularly humidity and temperature gradients within the prosthetic socket (Figure 1) [9].
For amputee athletes, elevated activity levels and repetitive cyclical loading during sport impose amplified physiological stress, substantially increasing vulnerability to dermatologic sequelae including contact irritation, pressure ulcers, and verrucous hyperplasia [10]. Systematic monitoring and mitigation of these mechanical forces are therefore essential to preserving skin integrity and optimizing prosthetic function in this population [11].
Skin complications in amputee athletes are heavily influenced by how prosthetic liners, socket materials, sweat, and heat interact during activity. Materials with poor ventilation and heat retention trap moisture against the skin, increasing sweat production and causing maceration—which heightens the risk of irritation, rashes, and ulcers [12]. Silicone liners, though cushioning, tend to promote sweating and require daily cleaning to prevent hygiene-related problems [13]. Exercise significantly raises temperature and humidity inside the socket, intensifying sweat production and discomfort. Research using sensors and thermal imaging confirms that skin temperature and moisture levels spike after physical activity, creating hot spots and sweat accumulation that can damage skin integrity-especially during intense or prolonged exercise.
Newer technologies show promise in addressing these issues. Vented liner-socket systems effectively reduce humidity and perceived sweating while maintaining secure fit [12]. Similarly, phase-change material (PCM) liners and sockets with cooling channels help regulate skin temperature and improve comfort, potentially preventing skin breakdown [14]. However, more research is needed to confirm whether these innovations provide lasting benefits for athletic populations [14].
Epidemiology and Risk Factors
Skin problems are common and clinically important in lower limb amputees who use prostheses, particularly among athletes. Studies report that 34% to 77% of prosthesis users experience cutaneous complications, with variation depending on the population studied and assessment methods used [15]. General amputee populations show skin problem rates of 41% to 74%, with higher frequencies among more active individuals and those wearing prostheses for extended daily periods [16]. A large Dutch survey found that 63% of users reported skin issues within the past month, with younger, more active amputees at greatest risk [17]. Another recent study reported a 77% one-month prevalence, though severe problems were not linked to higher BMI [18].
Athletes face elevated risk due to increased mechanical stress, repetitive friction, and prolonged prosthesis use during training and competition [19]. Athletic activity and employment status are independent risk factors for skin complications, with active amputees showing higher rates of dermatologic problems. Common sport-related issues include friction blisters, pressure ulcers, contact dermatitis (both irritant and allergic), epidermal hyperplasia, and bacterial or fungal infections [16]. These complications significantly affect daily life, often reducing prosthesis use, limiting athletic participation, and diminishing quality of life [2]. Fungal and bacterial infections, intertriginous dermatitis, and eczema occur frequently, especially with increased humidity and prolonged wear. Additional risk factors include summer season and daily prosthesis use exceeding eight hours [20].
Key risk factors for sport-related skin complications in lower limb amputee athletes include prosthetic fit, amputation level, activity intensity, hygiene practices, and environmental conditions. Prosthetic fit is the primary determinant of skin health. Poor fit generates friction, pressure, and shear forces that cause irritant and allergic contact dermatitis, ulcers, and epidermal hyperplasia. Frequent adjustments and individualized fitting are essential, particularly for highly active athletes [21]. While sport-specific prostheses reduce risk, they do not eliminate it [4].
Amputation level significantly influences complication rates. Proximal amputations create greater mechanical stress and biomechanical demands than distal amputations, increasing vulnerability to skin problems [22]. Higher-level amputations may also impair thermoregulation, further elevating risk during intense activity [19]. Activity intensity directly correlates with skin complications. Athletes in high-impact or endurance sports face elevated risk from repetitive loading, prolonged prosthesis use, and sustained exposure to friction and moisture [15]. Hygiene practices play a critical role. Both excessive washing with antibacterial soaps and inadequate stump or liner hygiene increase susceptibility to infections and dermatitis. Smoking compounds this risk [17]. Optimal prevention involves regular but moderate cleaning, prompt treatment of skin breaks, and avoidance of irritants, as emphasized by American College of Sports Medicine guidelines [23]. Environmental factors including heat, humidity, and facility cleanliness further modulate risk. Elevated temperature and humidity increase perspiration and moisture accumulation, promoting maceration and infection. Contaminated equipment and poor facility hygiene present additional hazards [2].
Types of Cutaneous Complications
Lower limb amputee athletes face elevated risk for skin complications during sports due to increased mechanical stress, friction, and occlusion at the skin-prosthesis interface. These complications primarily fall into two categories: mechanical injuries and dermatitis. Mechanical injuries include friction blisters, abrasions, pressure ulcers, calluses, and verrucous hyperplasia, arising from repetitive shear forces, pressure points, and ill-fitting sockets during high-intensity or prolonged activity. Ulcers and irritations are most frequently documented, along with calluses and inclusion cysts [10]. Athletes experience particularly high rates of blisters and abrasions due to increased loading and movement, which can lead to secondary infection [19].
Dermatitis manifests as either irritant or allergic contact dermatitis. Irritant dermatitis results from physical and chemical irritation—sweat, heat, and friction—while allergic contact dermatitis stems from sensitization to prosthetic materials or liners. Allergic reactions account for a substantial proportion of residual limb dermatitis cases, warranting patch testing for persistent or atypical presentations [16]. Both types present with erythema, pruritus, and scaling, making clinical differentiation challenging [21]. Bacterial and fungal infections represent the primary infectious complications in amputee athletes. Bacterial infections are more prevalent, typically manifesting as cellulitis or localized abscesses at the residual limb-prosthesis interface. Contributing factors include elevated humidity, friction, and microtrauma from prosthetic use [3]. Fungal infections, though less frequent, are predominantly caused by dermatophytes thriving in the moist prosthetic socket environment [16]. Prolonged athletic activity, excessive perspiration, and inadequate hygiene practices amplify risk for both infection types [19].
Chronic skin alterations result from repetitive mechanical stress, sustained moisture exposure, and allergic reactions. Common manifestations include irritant and allergic contact dermatitis, verrucous hyperplasia, epidermal hyperplasia, calluses, inclusion cysts, and chronic ulcerations [2]. Allergic contact dermatitis frequently relates to prosthetic materials or liners, with patch testing confirming sensitization in a substantial proportion of affected athletes. Persistent friction and pressure produce hyperkeratotic lesions, cyst formation, and ulceration that can significantly impair prosthesis tolerance and athletic performance [10]. Athletes also commonly report excessive perspiration and cold skin, reflecting altered thermoregulation and increased physiological demands (Figure 2) [17]. Early recognition and coordinated multidisciplinary management are critical to preserving prosthetic function and maintaining athlete quality of life.
Prevention and Management
Skin complications affect 36% to 70% of lower limb amputee athletes using prostheses, representing a significant clinical challenge [2]. Common disorders include ulcers, irritations, calluses, verrucous hyperplasia, and contact dermatitis, arising from mechanical shear, friction, elevated humidity, and immune vulnerability at the residual limb [24]. These complications frequently reduce prosthesis tolerance, compromise athletic performance, and diminish quality of life [3].
Optimal prosthetic fit and rigorous hygiene form the foundation of prevention. Technological advances, including microprocessor-controlled variable-stiffness ankle-foot devices, demonstrate improved biomechanics and may reduce abnormal loading patterns that contribute to skin breakdown [25]. Sport-specific prostheses are engineered to accommodate athletic demands while minimizing injury risk [4]. Regular evaluation of prosthetic fit, socket interface, and liner materials is essential, as improper fit and inappropriate materials are primary contributors to cutaneous problems [19].
Skin care protocols should emphasize daily washing and thorough drying of the residual limb while avoiding antibacterial soaps that may provoke irritation.[26] The American College of Sports Medicine recommends routine surveillance for skin infections, strict hygiene adherence, and prompt exclusion from sport until lesions resolve [27]. Multidisciplinary collaboration—integrating dermatology, rehabilitation medicine, and prosthetics expertise-enables early detection and intervention critical for sustaining athletic participation [27,28].
Athletes should be trained in self-examination techniques using mirrors and encouraged to engage family members or support persons in routine skin monitoring, particularly when visual limitations exist. Education must address modifiable risk factors including smoking cessation and elimination of unnecessary antibacterial products [17]. Athletes require individualized guidance addressing the unique demands of their sport—including intensified mechanical loading, increased perspiration, and environmental exposures—along with targeted risk mitigation strategies [29].
Future Directions
Emerging strategies to mitigate sport-related cutaneous complications in lower limb amputee athletes focus on three pivotal technological innovations: smart prosthetics, antimicrobial materials, and telemonitoring systems [30]. Next-generation prosthetics integrate real-time sensor technologies to continuously monitor pressure distribution, temperature fluctuations, and tissue health at the residual limb-socket interface [31]. Wireless, battery-free sensors transmit data to external devices, enabling early detection of impending skin breakdown and dynamic socket optimization—critical capabilities for preventing friction injuries and pressure ulcers in athletes [32]. Emerging neuroprosthetic feedback systems aim to restore sensory perception and reduce cognitive load during prosthesis use, potentially lowering complication risk through improved gait mechanics and enhanced prosthetic embodiment [33,34].
Advanced antimicrobial coatings for prosthetic sockets and liners address the elevated infection risk associated with prolonged skin contact and perspiration during athletic activity [35]. Surface technologies incorporating metal and metal oxide nanoparticles and phytochemical compounds demonstrate broad-spectrum antimicrobial efficacy, biofilm disruption, and superior biocompatibility, with potential to substantially reduce infection rates and improve tissue integration [36,37]. These innovations are particularly salient given rising antimicrobial resistance in athletic populations [38].
Remote monitoring platforms utilizing wearable sensors and mobile health technologies enable continuous tracking of skin integrity, prosthetic fit, and activity patterns. End-users and clinicians emphasize the importance of lightweight, unobtrusive systems that generate actionable insights, facilitating timely intervention and individualized prosthetic management [39]. These platforms may additionally support clinical reimbursement and decision-making through objective documentation of complications and prosthetic performance [30,40].
These converging innovations hold promise for reducing the incidence and severity of cutaneous complications, enhancing athlete safety, and improving long-term outcomes in this population. Future research should focus on sport-specific studies and standardized reporting.
Conclusion
Skin complications remain a prevalent and consequential challenge for amputee athletes using lower limb prostheses, arising from the complex interplay of mechanical loading, moisture accumulation, and material interactions at the socket–skin interface. These dermatologic issues not only compromise comfort and prosthesis tolerance but also limit athletic participation and performance. Preventive strategies centered on optimal prosthetic fit, routine skin surveillance, strict hygiene, and early multidisciplinary management are critical to sustaining sport participation and minimizing morbidity. Ongoing advances in prosthetic design—such as temperature-regulating liners, antimicrobial coatings, and sensor-based feedback systems—offer promising avenues for real-time monitoring and risk reduction. However, the current literature remains limited by small sample sizes, heterogeneous methodologies, and a lack of sport-specific data. Future research should prioritize prospective studies that define the biomechanical and environmental determinants of skin health in athletic contexts, evaluate the clinical utility of emerging technologies, and establish standardized, evidence-based guidelines for prevention and management. By integrating innovation with individualized care, clinicians and researchers can substantially improve outcomes and quality of life for amputee athletes striving for high-level performance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2021 US Obesity Forecasting Collaborators. National-level and State-level Prevalence of Overweight and Obesity Among Children, Adolescents, and Adults in the USA, 1990-2021, and Forecasts up to 2050. The Lancet 404 (2024): 2278–2298.
- 2Phil Mc Ewan, Faurby M, Lübker C, The Evolving Burden of Obesity in the U.S.: A Novel Population-Level System Dynamics Approach. Journal of Medical Economics 28 (2025): 1512–1525.40880254 10.1080/13696998.2025.2554518 · doi ↗ · pubmed ↗
- 3Qiyuan KL Mechanisms of Action and Therapeutic Applications of GLP-1 and Dual GIP/GLP-1 Receptor Agonists. Front Endocrinol 15 (2024): 1431292.
- 4Pillarisetti L, Agrawal DK. Semaglutide: Double-edged Sword with Risks and Benefits. Arch Intern Med Res 8 (2025): 1–13.39902055 10.26502/aimr.0189 PMC 11790292 · doi ↗ · pubmed ↗
- 5Nauck Michael A, Müller Timo D. Incretin Hormones and Type 2 Diabetes. Diabetologia 66 (2023): 1780–1795.37430117 10.1007/s 00125-023-05956-x PMC 10474001 · doi ↗ · pubmed ↗
- 6Zafer M, Tavaglione F, Manuel RG, GLP-1 Receptor Agonists and Glucagon/GIP in Obesity Management: Review Article. Aliment Pharmacol Ther 61 (2025): 1872–1888.40364529 10.1111/apt.70196 PMC 12323726 · doi ↗ · pubmed ↗
- 7Nauck MA, Daniel RQ, Jakob W, The Evolving Story of Incretins (GIP and GLP-1) in Metabolic and Cardiovascular Disease: A Pathophysiological Update. Diabetes Obes Metab 23 (2021): 5–29.34310013 10.1111/dom.14496 · doi ↗ · pubmed ↗
- 8Holst JJ. The Physiology of Glucagon-Like Peptide 1. Physiol Rev 87 (2007): 1409–1439.17928588 10.1152/physrev.00034.2006 · doi ↗ · pubmed ↗