Pathogens on High-Touch Surfaces in an Arid Megacity: A Longitudinal Molecular Surveillance Study
Mohamad Taisir Ahmad Ghiba, Saleh Ahmed Eifan, Abdulkarim Fahad Alhetheel, Atif Hanif

TL;DR
This study tracks pathogens on high-touch surfaces in Riyadh, Saudi Arabia, finding that heat influences viral presence and hospitals and airports are key hotspots.
Contribution
The study provides the first molecular surveillance baseline of pathogens on surfaces in an arid megacity and links heat to viral persistence.
Findings
19 out of 55 pooled surface samples tested positive for pathogens, including SARS-CoV-2, Adenovirus, and Cryptosporidium.
Hospitals and airports were primary hubs for respiratory viruses, while ATMs frequently had Cryptosporidium.
Higher ambient temperature was significantly associated with detecting viral rather than non-viral pathogens.
Abstract
Contaminated environmental surfaces (fomites) act as pathogen reservoirs, yet surveillance data in arid megacities like Riyadh, Saudi Arabia—characterized by extreme heat and indoor climate control—remain limited. This study established a city-wide molecular baseline for surface contamination and evaluated meteorological influences. We conducted a stratified, longitudinal study (February 2023–May 2024), collecting 270 swabs from seven zones, including hospitals, airports, ATMs, and community hubs. Samples were pooled (N = 55) and screened using QIAstat-Dx multiplex PCR panels. Nineteen pools (34.5%) tested positive. Viral pathogens (SARS-CoV-2, Adenovirus, Rhinovirus) were detected in 10 pools (18.2%) and non-viral pathogens (bacteria/parasites) in 13 pools (23.6%), with 7.3% co-detections. Hospitals and airports emerged as primary hubs for respiratory viruses, while Cryptosporidium was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
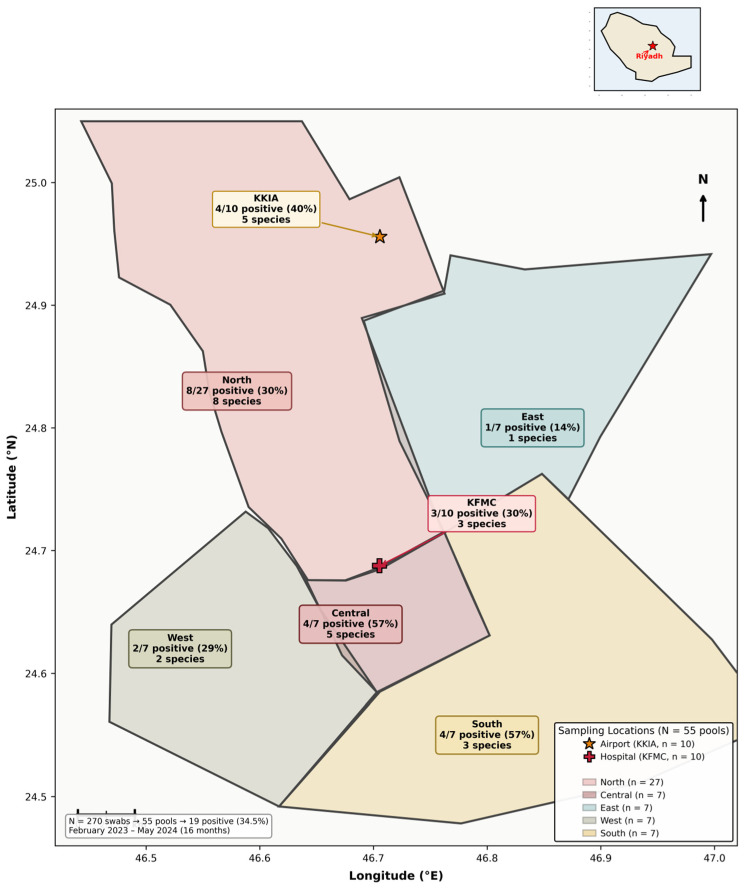 Figure 1
Figure 1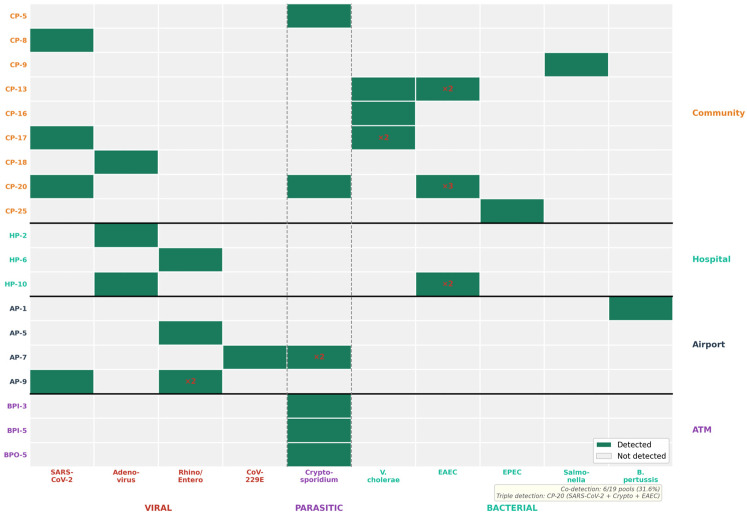 Figure 2
Figure 2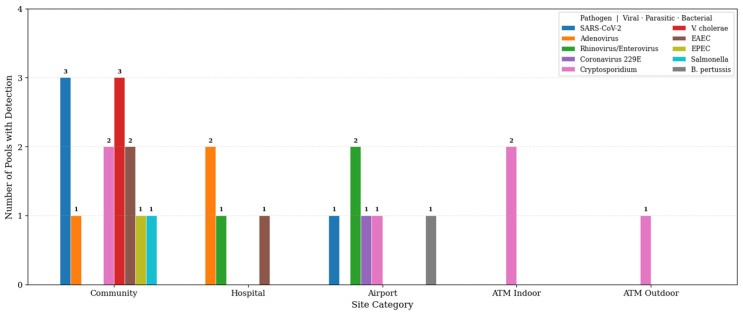 Figure 3
Figure 3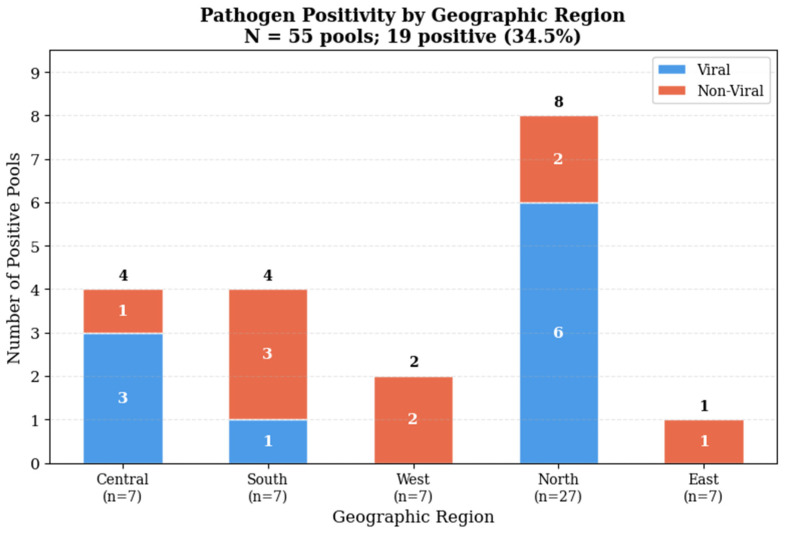 Figure 4
Figure 4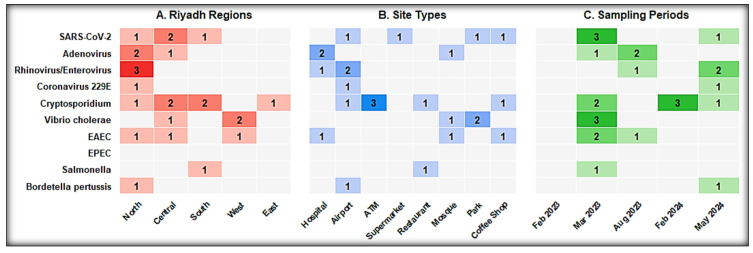 Figure 5
Figure 5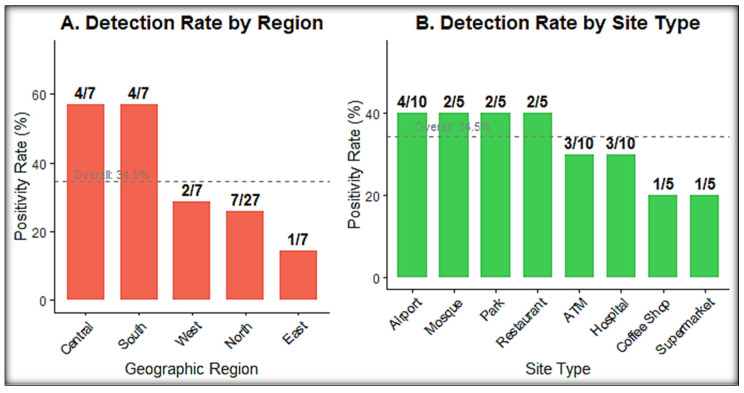 Figure 6
Figure 6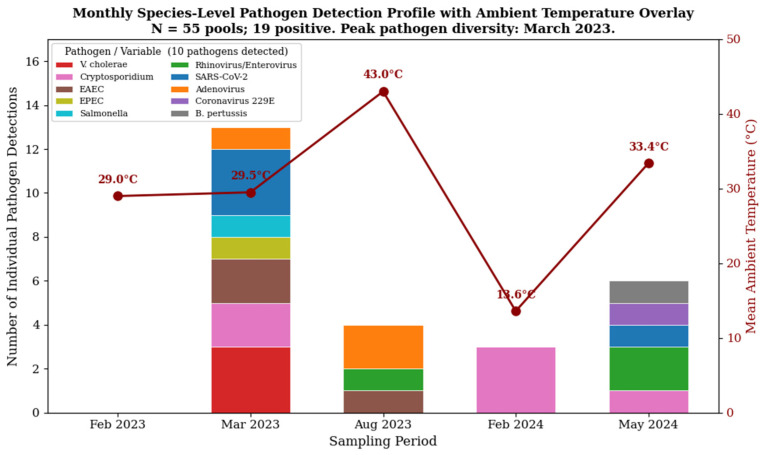 Figure 7
Figure 7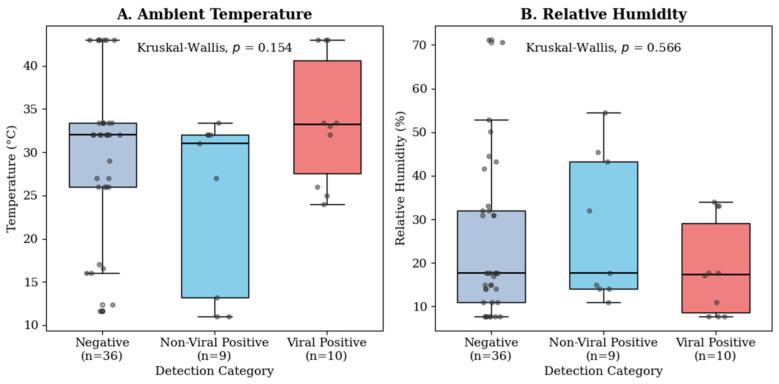 Figure 8
Figure 8- —King Saud University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfection Control and Ventilation · Indoor Air Quality and Microbial Exposure · COVID-19 impact on air quality
1. Introduction
Environmental reservoirs complicate the management of infectious diseases globally. Respiratory and gastrointestinal pathogens, including SARS-CoV-2, influenza, and norovirus, move through contaminated surfaces (fomites) and create opportunities for indirect spread [1,2]. While the field has debated exactly how much fomites contribute compared with airborne transmission—especially during the COVID-19 pandemic—evidence indicates that high-touch surfaces in dense urban settings meaningfully support pathogen dissemination [3,4,5]. Most of our current understanding of environmental persistence comes from temperate regions in North America, Europe, and East Asia. In those settings, seasonal viral peaks typically align with colder temperatures and lower humidity, conditions known to enhance the stability of enveloped viruses [6,7]. This “temperate bias” left a practical gap in the literature: we knew far less about how pathogens behave across the hot, arid climates typical of the Middle East and the Gulf Cooperation Council (GCC) countries.
Riyadh, Saudi Arabia, offers a clear test case. Summer ambient temperatures frequently exceed 45 °C, while relative humidity often drops below 15% [8,9]. Classical environmental virology suggests that such conditions should speed the inactivation of enveloped viruses and reduce fomite-related risks [10,11]. However, that “outdoor sterilization” hypothesis did not reflect how modern arid cities function day to day. Riyadh operates as an “indoor city,” where routine life occurs almost exclusively in air-conditioned malls, offices, schools, and homes held at 20–24 °C [12,13,14,15]. We hypothesized that these indoor microclimates might shield pathogens from the harsh outdoor environment, potentially supporting year-round persistence [16,17]. Riyadh also serves as a major transit gateway for millions of religious pilgrims traveling for Hajj and Umrah [18]. This scale of movement creates repeated opportunities for pathogen introduction, as illustrated by earlier MERS-CoV and SARS-CoV-2 events [19]. However, comprehensive molecular baselines for surface contamination in Riyadh remained elusive. Prior studies primarily focused on clinical areas or specific single pathogens, leaving the broader environmental burden unclear [20].
We designed this study to address the “arid urban gap” through a longitudinal, multi-site molecular surveillance campaign. We aimed to: (1) measure the prevalence and diversity of respiratory and gastrointestinal pathogens on high-touch surfaces in public spaces; (2) identify specific contamination hotspots; and (3) investigate the relationship between meteorological factors (temperature and humidity) and the differential detection of viral versus non-viral pathogens. Our principal findings reveal that, contrary to the outdoor sterilization hypothesis, higher ambient temperatures were associated with increased viral detection, suggesting that indoor behavioral dynamics drive pathogen persistence in arid megacities.
2. Materials and Methods
2.1. Study Design and Setting
We conducted a stratified, longitudinal environmental surveillance study over 16 months, from February 2023 to May 2024. The work took place across the Riyadh metropolitan area, which we divided into seven geographic zones to ensure representative coverage: five community regions (North, South, East, West, and Central Riyadh) and two high-significance institutional hubs—King Fahad Medical City (KFMC; 24.6885° N, 46.7028° E) and King Khalid International Airport (KKIA; 24.9576° N, 46.6988° E). The five community sampling zones and two institutional facilities are shown in Figure 1.
The five community regions were: North Riyadh (24.736° N, 46.682° E), South Riyadh (24.584° N, 46.774° E), East Riyadh (24.695° N, 46.752° E), West Riyadh (24.633° N, 46.535° E), and Central Riyadh (24.666° N, 46.711° E); multiple sites within each region were sampled (Figure 1). All sampling was anchored within the Riyadh metropolitan area (centered on approximately 24.7136° N, 46.6753° E). Stratified spatial designs are widely used to improve cost-efficiency and geographic representativeness in environmental surveys [21].
2.2. Sampling Strategy and Site Selection
We selected sites after identifying the busiest touchpoints in each setting to maximize the chance of detecting contamination [22,23]. Prior studies indicate that high-touch non-porous surfaces in community settings can harbor respiratory viral RNA and correlate with local COVID-19 trends [24]. We collected a total of 270 environmental swabs (Table 1). Target surface types included the following:
- Healthcare Facilities (KFMC): Waiting area armchairs, reception counters, clinic door handles, and restroom sinks. These surfaces represented routine interfaces among patients, healthcare workers, and visitors [25].
- Transportation Hubs (KKIA): Check-in counters, luggage trolleys, escalator handrails, food court tables, and restroom facilities. Travelers repeatedly handled these surfaces at peak flow times.
- Community Hubs: Public parks (benches, play equipment), mosques (ablution areas, door handles), supermarkets (shopping cart handles, payment terminals), and coffee shops (tables, counters).
- Financial Services: Automated Teller Machines (ATMs), stratified into indoor (bank branch) and outdoor (drive-through or street-side kiosk) placements.
2.3. Sample Collection Protocol
To improve recovery from dry, non-porous surfaces, we used sterile flocked nylon swabs (SAMCO MDM 750, Second Advance Medical Company, Riyadh, Saudi Arabia) pre-moistened with 2 mL of Viral Transport Medium (VTM) [26,27]. Flocked nylon swabs significantly enhance microbial and viral recovery from environmental and clinical surfaces compared with traditional fiber swabs, including under dry-surface conditions [25,28,29,30]. For each sample, we swabbed approximately 100 cm^2^ using a consistent grid approach (vertical, horizontal, and diagonal strokes) while rotating the swab to maximize uptake. For smaller or irregular targets, such as door handles or ATM keypads, we swabbed the entire functional contact area.
We managed strict aseptic protocols to prevent cross-contamination. Personnel wore PPE, including gloves and masks, and changed gloves between every sample [31]. We placed samples into sterile transport tubes immediately, kept them on ice (4 °C) during transport, and ensured transfer to −80 °C storage to maintain viral RNA stability [32].
2.4. Sample Pooling and Extraction
We combined the 270 individual swabs into 55 pooled samples. We pooled based on spatial and temporal logic; each pool contained 4–5 swabs taken from the same location type on the same date. This pooling approach has been widely used in infectious disease surveillance [33,34] and can improve efficiency and reduce costs for SARS-CoV-2 RT-PCR screening when pool sizes remain modest [35,36,37].
We performed nucleic acid extraction using the QIAstat-Dx automated cartridge system, which integrated lysis, purification, and elution. Automated cartridge-based nucleic acid platforms provide robust workflows for diverse clinical and environmental specimens [38]. Each cartridge included an internal control (MS2 bacteriophage) to allow us to detect inhibition from dust or cleaning agents common in environmental matrices.
The composition of the pooled samples is summarized in Table 2 (Results).
2.5. Molecular Detection (Multiplex PCR)
We screened samples using the QIAstat-Dx Respiratory SARS-CoV-2 Panel and the QIAstat-Dx Gastrointestinal Panel 2 (QIAGEN, Hilden, Germany). These syndromic assays used real-time reverse-transcription PCR (RT-PCR) to detect multiple targets in parallel. Independent evaluations of the QIAstat-Dx Respiratory SARS-CoV-2 Panel reported good agreement with reference RT-PCR workflows for several respiratory targets [39,40].
Respiratory Panel Targets: SARS-CoV-2, Influenza A/B, RSV, Adenovirus, Rhinovirus/Enterovirus, Parainfluenza (1–4), Human Metapneumovirus, Bordetella pertussis, Legionella pneumophila, and Mycoplasma pneumoniae.Gastrointestinal Panel 2 Targets: Norovirus (GI/GII), Rotavirus A, Adenovirus F40/41, Salmonella spp., Campylobacter spp., Vibrio cholerae, C. difficile, ETEC, EPEC, EAEC, Cryptosporidium, Giardia lamblia, and Entamoeba histolytica [41].
2.6. Statistical Analysis
All statistical analyses were conducted using R (version 4.5.2; R Core Team, 2025) via RStudio (version 2025.09.2+418). Descriptive summaries captured the overall prevalence and the distribution of detected pathogens. The main outcome variable was detection of any pathogen (binary: positive/negative). For pools that tested positive, a second outcome classified pathogen type (Viral vs. Non-Viral).
Important note on classification: For the binary logistic regression, we grouped the four pools with co-detection (Viral + Non-Viral) into the “Viral” category to focus the model on respiratory viral drivers. As a result, inferential comparisons tested “Viral/Mixed” (n = 10) versus “Non-Viral Only” (n = 9). The descriptive results, however, reported total non-viral detections (n = 13 pools with non-viral detections) to reflect the full set of organisms detected.
We recorded ambient temperature (°C) and humidity at sampling time. Shapiro–Wilk testing indicated non-normal distributions for these meteorological variables, so we used non-parametric comparisons (Mann–Whitney U and Kruskal–Wallis tests) [42]. To test whether meteorological conditions are related to pathogen composition, we constructed a binary logistic regression model using Pathogen Type as the outcome and temperature and humidity as predictors. We assessed model performance using overall model significance, Nagelkerke R^2^ [43], and classification accuracy; the Hosmer–Lemeshow test could not be computed due to the small sample size. Statistical significance was set at p < 0.05.
3. Results
A total of 270 environmental surface swabs were collected and aggregated into 55 pooled samples for molecular analysis. The study covered five distinct setting categories across Riyadh, including community hubs, institutional centers, and financial service points. Overall, pathogen DNA or RNA was detected in 19 of the 55 pools, corresponding to a cumulative prevalence of 34.5%. The distribution of sampling effort and positivity rates across these settings is summarized in Table 2.
The complete pool-level metadata, including constituent swab identifiers, collection dates, surface types, and environmental conditions for all 55 pools, is provided in Supplementary Table S1.
3.1. Overall Prevalence and Pathogen Diversity
The analysis included 55 pooled samples representing 270 individual swabs. Nineteen pools tested positive for at least one target pathogen, producing an overall positivity rate of 34.5%. The remaining 36 pools (65.5%) tested negative. Positive pools contained a broad mix of viral, bacterial, and parasitic targets:
- Viral Pathogens: Detected in 10 pools (18.2% of total). The most frequent viral detections were SARS-CoV-2 (4 pools), Rhinovirus/Enterovirus (3 pools), and Adenovirus (3 pools).
- Non-Viral Pathogens: Detected in 13 pools (23.6% of total). This category included bacteria (Vibrio cholerae, Salmonella, pathogenic E. coli) and parasites (Cryptosporidium).
3.2. Co-Detection Patterns
Four pools (7.3%) showed co-detection of viral and non-viral pathogens:
- Pool CP-17: Co-detection of SARS-CoV-2 and Vibrio cholerae.
- Pool CP-20: Multi-pathogen detection of SARS-CoV-2, Cryptosporidium, and Enteroaggregative E. coli (EAEC).
- Pool HP-10: Co-detection of Adenovirus and EAEC.
- Pool AP-7: Co-detection of Coronavirus 229E and Cryptosporidium.
Additionally, two pools showed within-category multi-pathogen co-detection: Pool CP-13 contained Vibrio cholerae and EAEC (dual enteric contamination), and Pool AP-9 contained Rhinovirus/Enterovirus and SARS-CoV-2 (dual respiratory viral contamination). The complete co-detection matrix is visualized in Figure 2. In total, 6 of 19 positive pools (31.6%) harbored ≥2 distinct pathogens.
To assess whether multi-pathogen co-detection reflected non-random contamination clustering, we compared observed co-detection rates to those expected under an independence model based on marginal species prevalences. Among 19 positive pools, 6 (31.6%) harbored ≥2 pathogens, compared to an expected rate of 19.8% under independence (expected: 3.76 pools; observed: 6 pools; ratio: 1.6×). While this excess did not reach statistical significance (binomial test, p = 0.156), the systematic co-occurrence of respiratory viruses with enteric pathogens on restroom surfaces suggests shared contamination pathways rather than independent deposition events.
3.3. Detailed Pathogen Counts
From the raw detection outputs, the observed frequencies were:
- Cryptosporidium spp.: Detected most often, appearing in 6 pools.
- SARS-CoV-2: Detected in 4 pools.
- Vibrio cholerae: Detected in 3 pools.
- Pathogenic E. coli: EAEC (n = 3) and EPEC (n = 1).
- Adenovirus: Detected in 3 pools.
- Rhinovirus/Enterovirus: Detected in 3 pools.
- Other detections: Salmonella (n = 1), Bordetella pertussis (n = 1), Coronavirus 229E (n = 1).
The complete pathogen-specific detection profile, including Ct values, site associations, plausible circulation pathways, and recommended control measures, is presented in Table 3.
3.4. Site-Specific Contamination Profiles
Pathogen distribution varied across zones and showed clear site-linked patterns (Figure 3 and Figure 4).
Community Hubs (Parks, Cafes, Markets): This zone carried the highest absolute burden, with 9 positive pools (36% positivity). The profile was diverse, including SARS-CoV-2, Salmonella, Vibrio cholerae, and Cryptosporidium. The mix likely reflected high turnover, variable hygiene practices, and broad public access.Airports (KKIA): Four pools tested positive (40% positivity). Detections included SARS-CoV-2, Rhinovirus, and Coronavirus 229E, consistent with respiratory introduction through travel. One airport pool also contained Bordetella pertussis, and another contained Cryptosporidium.Hospitals (KFMC): Three pools tested positive (30% positivity). The profile leaned toward respiratory viruses (Adenovirus, Rhinovirus) and enteric bacteria (EAEC). Adenovirus appeared on a hospital toilet door handle and waiting area seating, highlighting routine infection-control pressure points in high-traffic areas.Banking Services (ATMs): Three pools tested positive. A clear pattern emerged: positive ATM pools in this zone yielded only Cryptosporidium, with no viruses or bacteria co-detected. This suggested that ATM keypads functioned as a selective niche where hardy Cryptosporidium oocysts persisted, while more fragile viral envelopes and bacterial cells likely degraded under desiccation and heat.
3.5. Surface Contamination Risk Ranking
To translate molecular detection data into actionable risk stratification, surface types were ranked by positivity rate, pathogen diversity, and co-detection frequency (Table 4). Extended cross-tabulations of pathogen detection by site type, surface category, and sampling period are presented in Figure 5.
Restroom surfaces ranked highest across all metrics: highest positivity (44.4%), highest diversity (all 10 species detected), and highest co-detection rate (42%), identifying restrooms as the primary convergence zone for multi-route pathogen transmission. ATM touchscreens (indoor) ranked second in terms of positivity (40.0%) but showed Cryptosporidium exclusively with zero co-detection, indicating a single-pathway contamination mechanism requiring oocysticidal disinfection. Hospital surfaces showed moderate positivity (30.0%) with intermediate diversity and 33% co-detection, reflecting healthcare-associated respiratory and enteric pathogen overlap. Outdoor ATM surfaces ranked lowest (20.0%), suggesting that UV exposure and environmental weathering reduce but do not eliminate parasitic contamination.
The surface risk ranking informed the recommended disinfection strategy by surface type (Table 5).
The detection of infectious agents exhibited a distinct temporal trend during the study period. As illustrated in Figure 6 (species-level monthly profiles are shown in Figure 7), viral pathogens were predominantly detected during the warmer summer months (August), whereas bacterial and parasitic agents were more frequently identified during the cooler winter/spring season (February–March). This seasonal divergence was not statistically significant (χ^2^ = 1.35, p = 0.246), suggesting that environmental conditions in Riyadh—specifically the extreme summer heat driving populations indoors—may differentially select for viral persistence on high-touch surfaces.
3.6. Environmental Drivers: The Temperature Effect
To examine the “Indoor City” hypothesis, we analyzed the relationship between meteorological variables and pathogen detection in three stages.
3.6.1. Comparison Across All Groups
First, a Kruskal–Wallis H test was conducted to compare median temperatures across the three outcome groups: Negative, Non-Viral Positive, and Viral Positive. While the Viral Positive group had the highest median temperature (33.2 °C), the overall difference across groups was not statistically significant (H(2) = 3.74, p = 0.154) (Figure 8). Air quality index distributions across pathogen detection categories are presented in Figure S2.
To isolate the specific effect of environmental conditions on pathogen survival, we constructed a binary logistic regression model comparing Viral Positive pools against Non-Viral and Negative pools. The analysis identified ambient temperature as a significant positive predictor of viral detection. Specifically, for every 1 °C increase in temperature, the odds of detecting a viral pathogen increased significantly, reinforcing the observation that viral targets were more frequently recovered during the warmer sampling periods. The magnitude of this environmental effect is detailed in Table 6.
3.6.2. Viral Positive vs. Negative Pools
Second, we compared pools positive for viruses (n = 10) against negative pools (n = 45). Although viral-positive pools were associated with a slightly higher median temperature (33.2 °C) than negative pools (32.0 °C), this difference was not statistically significant (p = 0.225). Binary logistic regression confirmed that neither temperature nor humidity significantly predicted the presence of a virus compared to a negative result (Overall model: χ^2^(2) = 2.578, p = 0.267).
3.6.3. Viral vs. Non-Viral Positive Pools
Finally, to test whether meteorological conditions could differentiate between types of contamination, we performed a binary logistic regression comparing only the positive pools (N = 19) (Table 7). In this model, higher ambient temperature was a significant predictor of viral detection (χ^2^(2) = 9.345, p = 0.009; Nagelkerke R^2^ = 0.518).
Temperature: Higher ambient temperature significantly predicted viral detection (OR = 1.728, 95% CI [1.050, 2.845], p = 0.032). For each 1 °C increase, the odds that a positive sample contained a virus (rather than a non-viral pathogen) rose by 72.8%.Humidity: Relative humidity did not reach significance in this model (p = 0.200).
3.6.4. UV Index as Environmental Correlate
UV index data (categorical: Low, Moderate, High, Very High) were available for all 55 pools. Among the 19 positive pools, a distinct pattern emerged: at Low UV index, all five detections (100%) were non-viral pathogens (Cryptosporidium and enteric bacteria), whereas 10 of 11 viral-positive pools were detected at High or Very High UV levels. Fisher’s exact test confirmed that viral detection was significantly associated with higher UV categories (Low + Moderate: 1/22 pools viral; High + Very High: 10/33 pools viral; OR = 0.12, p = 0.036). This pattern parallels the temperature finding: high UV co-occurs with extreme heat, and both drive populations indoors, indirectly increasing respiratory virus deposition on climate-controlled indoor surfaces (Figure S6).
ROC Analysis: ROC analysis confirmed temperature as a statistically significant classifier of viral versus non-viral positive pools (AUC = 0.756, 95% CI [0.532, 0.979], p = 0.025), with an optimal cutoff of >32.50 °C yielding 60.0% sensitivity and 88.9% specificity.
Additional supplementary visualizations are provided: functional surface zone analysis (Figure S1), AQI and detection (Figure S2), multivariate environmental analysis (Figure S3), AQI versus pathogen load (Figure S4), pathogen diversity with co-detection patterns (Figure S5), UV index analysis (Figure S6), and environmental trend analysis (Figure S7). Complete pool-level metadata is provided in Supplementary Table S1.
4. Discussion
This study provided a broad molecular snapshot of high-touch surface contamination across Riyadh and established a baseline for environmental pathogen burden in an arid megacity, consistent with work showing that high-touch “hubs” can act as key nodes for microbial dissemination in public spaces [3,44]. The overall positivity rate of 34.5% matched, and in some cases exceeded, rates reported from temperate hospitals where ~63% of high-touch sites surpassed accepted cleanliness thresholds and a substantial fraction showed moderate–heavy contamination [45,46]. This reinforces evidence that frequently touched surfaces in community and healthcare environments often harbor diverse microorganisms at moderate-to-high loads [47,48]. That result pushed back against the assumption that the regional climate alone ensured environmental sterility.
4.1. The “Indoor City” Paradox: Heat and Viral Persistence
The most striking signal was the positive association between ambient temperature and viral detection (OR = 1.728). Experimental work has consistently shown that heat speeds inactivation of enveloped viruses such as SARS-CoV-2 [10] and other coronaviruses, with faster decay at higher temperatures on surfaces [49,50]. In a purely outdoor model, viral recovery should have dropped as temperatures climbed toward 45 °C.
The observed pattern pointed in a different direction. In Riyadh, higher outdoor heat likely shifted daily behavior. People moved indoors and stayed there longer, relying on climate-controlled spaces maintained around 20–24 °C with low humidity. Those indoor conditions could favor viral stability and increase airborne and fomite exposure. While this study did not measure ventilation directly, the literature links poor indoor air exchange to prolonged survival of respiratory viruses [51,52,53]. In that sense, “high temperature” in the dataset behaved like a proxy for “high indoor density.” More people indoors meant more shedding and more surface contact in malls, terminals, and hospitals, aligning with models suggesting that dense networks of high-touch surfaces can accelerate the redistribution of contamination [44]. That indoor load plausibly outweighed any outdoor “sterilization” effect from the sun and heat.
The temperature–detection association observed in this study is consistent with established evidence on the environmental determinants of pathogen RNA persistence. SARS-CoV-2 nucleic acid demonstrates greater stability in cold, dry environments, with surface detectability measured in days at 4 °C but declining to hours at temperatures exceeding 37 °C [54]. At temperatures above 38 °C—common outdoors in Riyadh for approximately five months of the year—thermal degradation acts as a natural reduction mechanism for enveloped viral RNA on exposed surfaces [55]. However, this outdoor effect is structurally bypassed in Riyadh’s built environment, where indoor temperatures are maintained at 20–24 °C by ubiquitous air conditioning—within the commonly reported range for respiratory virus transmission (15–25 °C) [6,15].
Humidity adds a second layer of complexity to the Indoor City framework. The relationship between relative humidity and viral RNA persistence follows a U-shaped curve: many respiratory viruses remain detectable longer in very dry (<40% RH) or very humid (>75% RH) environments, with more rapid nucleic acid degradation occurring at intermediate relative humidity (50–70% RH) [56]. Riyadh’s outdoor humidity frequently falls below 15% RH, while indoor air-conditioned spaces typically maintain 30–50% RH—both within the low-humidity persistence zone. This means that neither the outdoor nor the indoor humidity regime in Riyadh’s arid environment reaches the intermediate zone that would accelerate viral RNA decay, potentially contributing to the detection of enveloped viral nucleic acid on both indoor and outdoor surfaces in our dataset.
UV radiation represents the third environmental variable with relevance to surface pathogen dynamics. High-intensity UV radiation from sunlight accelerates degradation of SARS-CoV-2 and other enveloped viral RNA on surfaces, significantly reducing their outdoor detectability compared to shaded indoor environments [57,58]. Our exploratory analysis of UV index as a correlate of detection type (Section 3.6.4) revealed a significant association: viral detections were concentrated at High and Very High UV index categories (Fisher’s exact p = 0.036), while all detections at Low UV were exclusively non-viral. Importantly, this does not imply that UV increases viral persistence; rather, high UV co-occurs with extreme heat, and both together drive populations indoors, increasing respiratory virus deposition on climate-controlled indoor surfaces. UV index thus acts as an indirect proxy for indoor congregation behavior rather than a direct predictor of viral persistence.
Together, these three environmental variables—temperature, humidity, and UV radiation—operate in concert to shape the distinct contamination patterns observed across Riyadh’s indoor and outdoor surfaces. While mechanistic studies describe viability changes under controlled conditions, our dataset assesses nucleic acid detection rather than infectious viability; the environmental associations reported here should therefore be interpreted as correlates of RNA detectability patterns rather than direct measures of infection risk.
4.2. Pathogen-Specific Ecological Signals and Plausible Circulation Pathways
While the viral/non-viral binary classification served the specific statistical purpose of testing whether climatic conditions differentially predict pathogen type, the QIAstat-Dx panels identified pathogens at the species or genus level, revealing distinct ecological signatures across site types. The following sections interpret each major detection in the context of established transmission mechanisms and the arid indoor-city environment. All interpretations represent plausible pathways inferred from the consistency of site–pathogen associations with published mechanistic evidence; source attribution cannot be established from observational pooled surface detections.
SARS-CoV-2 (4 pools: CP-8, CP-17, CP-20, AP-9)
SARS-CoV-2 was the most frequently detected viral pathogen, recovered from community surfaces (supermarket carts, park benches, coffee shop tables) and an airport food court table. The relatively low Ct values (33.9–34.8), while above thresholds typically associated with recoverable infectious virus in clinical samples, suggest more recent contamination than the high-Ct (>35) detections of other pathogens in this dataset, though Ct values alone cannot establish viability. Detection is consistent with respiratory droplet deposition and direct hand contact from symptomatic or pre-symptomatic individuals. In air-conditioned indoor environments maintained at 20–24 °C, HVAC systems may contribute to redistribution of aerosolized virus to surfaces distant from the source individual, expanding the spatial footprint of fomite contamination [59]. The co-detection with V. cholerae in CP-17 and with Cryptosporidium and EAEC in CP-20 is consistent with convergent multi-source contamination at high-traffic community surfaces, where respiratory, fecal–oral, and hand-to-surface transmission routes overlap.
The outdoor half-life of SARS-CoV-2 at temperatures exceeding 27 °C is less than 2 h, and UV irradiance at Riyadh’s summer levels (>900 W/m^2^) further accelerates inactivation on unshaded surfaces [55]. The detection of SARS-CoV-2 during the warm sampling period (August 2023) therefore reflects the Indoor City dynamic: virus deposited on indoor surfaces at air-conditioned temperatures persists in conditions where outdoor surfaces experience rapid inactivation of enveloped viruses. This finding is consistent with the framework’s prediction that indoor high-touch surfaces in arid megacities serve as recurring sites of enveloped respiratory virus contamination even during extreme summer heat.
Adenovirus (3 pools: CP-18, HP-2, HP-10)
Adenovirus was detected on a mosque door handle (CP-18), a hospital waiting area seat (HP-2), and a hospital toilet door handle (HP-10). As a non-enveloped, double-stranded DNA virus, adenovirus exhibits exceptional environmental stability, retaining infectivity for weeks on stainless steel and polypropylene at 21–23 °C and resisting both desiccation and many alcohol-based formulations [60,61]. This stability makes adenovirus one of the pathogens most likely to accumulate on surfaces between cleaning events.
The HP-10 detection (toilet door handle, co-detected with EAEC) is consistent with the “toilet plume” mechanism, whereby virus-laden particles are aerosolized during flushing and deposited on adjacent surfaces, including door handles, taps, and flush buttons [62]. The dual respiratory and fecal–oral transmission capability of adenovirus means that both direct hand contact and toilet plume aerosolization may contribute to surface contamination in hospital restrooms. The mosque surface detection (CP-18) is noteworthy given that mosques in Riyadh are high-frequency, high-density shared-facility environments where multiple individuals make rapid sequential hand-to-surface contact, creating conditions favorable for fomite accumulation. The non-enveloped adenovirus capsid also confers resistance to many alcohol-based hand sanitizers, meaning that hand hygiene compliance alone may be insufficient to interrupt transmission in high-density worship settings without concurrent surface disinfection with non-alcohol agents.
Rhinovirus/Enterovirus (3 pools: HP-6, AP-5, AP-9)
Rhinovirus/Enterovirus was detected in a hospital children’s play area (HP-6), an airport toilet doorknob (AP-5), and an airport food court table (AP-9, co-detected with SARS-CoV-2). As a non-enveloped virus, rhinovirus persists on hard surfaces for hours to days, with greater stability than enveloped viruses under the low-humidity conditions characteristic of air-conditioned indoor environments [63]. The hospital play area detection is consistent with high shedding from pediatric populations, who are the primary reservoir for rhinovirus and frequently contaminate shared toys and surfaces through nasal secretions and hand contact.
The airport detections (AP-5, AP-9) are consistent with traveler-mediated introduction of respiratory pathogens. The co-detection of rhinovirus and SARS-CoV-2 in a single airport pool (AP-9) demonstrates the convergence of multiple respiratory viruses on high-touch surfaces in transit environments, consistent with airports functioning as mixing hubs where geographically distinct respiratory virus lineages are introduced simultaneously by arriving passengers.
Coronavirus 229E (1 pool: AP-7)
Human coronavirus 229E was detected on an airport ATM (AP-7, co-detected with Cryptosporidium). The detection of a seasonal coronavirus in an airport environment is consistent with the virus being introduced via international travel. Surface persistence studies show that 229E can survive up to 9 days on aluminum and glass surfaces at 21 °C under laboratory conditions, with markedly faster inactivation above 30 °C [64]. The climate-controlled airport terminal, maintained at approximately 22–24 °C, represents conditions near the laboratory optimum for 229E surface persistence, contextualizing the detection within the Indoor City framework. The co-detection with Cryptosporidium indicates convergent contamination from independent sources—respiratory virus introduction via a traveler and fecal–hand transfer of oocysts—on a shared high-touch interface.
Cryptosporidium spp. (6 pools: CP-5, CP-20, BPI-3, BPI-5, BPO-5, AP-7)
Cryptosporidium was the most frequently detected non-viral pathogen and the only pathogen detected in all three ATM-positive pools (BPI-3, BPI-5, BPO-5), though it was also found in community (CP-5, CP-20) and airport (AP-7) settings. Detection is consistent with fecal–hand–surface transfer via inadequate post-toilet hand hygiene. Oocysts are deposited on keypads by contaminated fingers, and the thick-walled oocyst structure (4–6 µm) confers extreme resistance to desiccation, heat, chlorine, and alcohol-based sanitizers [65]. This structural resilience explains the selective persistence of Cryptosporidium on ATM surfaces, where enveloped viruses would degrade within hours under Riyadh’s ambient outdoor temperatures.
The most distinctive site–pathogen pattern in this dataset was the exclusive Cryptosporidium-only profile of ATM-positive pools: all three ATM pools (BPI-3, BPI-5, BPO-5) contained Cryptosporidium and no other pathogen. Where alcohol-based wipes are used for surface maintenance, they are ineffective against protozoan oocysts, potentially creating a selective survival advantage: routine cleaning may reduce competing pathogens while leaving Cryptosporidium intact. This finding has direct infection prevention implications, as discussed in Section 4.3 below. The detection of Cryptosporidium in community (CP-5, CP-20) and airport (AP-7) pools is consistent with the ubiquitous fecal–oral route operating wherever hand hygiene is suboptimal after restroom use.
Vibrio cholerae (3 pools: CP-13, CP-16, CP-17)
V. cholerae was detected exclusively in community settings (Central and West Riyadh parks and cafes), with all three detections occurring in March 2023. This temporal clustering may reflect a shared environmental contamination source or a concurrent contamination event rather than independent sporadic detections. The fecal–oral route is the established transmission pathway; surface detection in food-handling areas is consistent with contamination from hands soiled after restroom use or from handling contaminated food items. V. cholerae survives on surfaces for hours to days, depending on moisture and organic matter, with less resistance to desiccation than oocysts. The co-detections with EAEC (CP-13) and SARS-CoV-2 (CP-17) indicate convergent contamination from both fecal–oral and respiratory routes on these community surfaces.
EAEC, EPEC, and Salmonella (community and hospital pools)
Enteroaggregative E. coli (EAEC; 3 pools: CP-13, CP-20, HP-10), enteropathogenic E. coli (EPEC; 1 pool: CP-25), and Salmonella spp. (1 pool: CP-9) were detected primarily in community settings, with one hospital detection (EAEC on HP-10, a toilet door handle). These organisms serve as fecal indicator markers, confirming inadequate hand hygiene after restroom use as a prevalent contamination pathway. The hospital toilet door detection (HP-10, co-detected with adenovirus) is particularly consistent with the toilet plume aerosolization mechanism depositing both respiratory and enteric pathogens on restroom surfaces. Community detections implicate food-handling and sanitation gaps in shared public spaces. Appropriately selected and correctly applied surface disinfectants are generally effective against these bacteria, indicating that improved cleaning frequency and hand hygiene infrastructure (soap, water, dispensers) at community sites are the primary control levers.
Bordetella pertussis (1 pool: AP-1)
B. pertussis was detected in a single airport pool. Environmental surface detection of B. pertussis is rarely documented, as the organism has limited environmental persistence and is sensitive to desiccation. The detection likely reflects recent respiratory shedding by a traveler, consistent with the airport’s role as a hub for the introduction of respiratory pathogens from diverse geographic origins. While surface transmission of B. pertussis is considered a minor route relative to droplet transmission, the detection underscores that airports serve as convergence points for a broad range of respiratory pathogens beyond the commonly surveilled influenza and coronaviruses.
4.3. Site-Specific Infection Prevention and Control Implications
These evidence-based recommendations translate the molecular findings into actionable protocols for specific end-users, including hospital Infection Prevention and Control (IPC) teams, airport facility management, municipal cleaning contractors, and ATM maintenance providers. The stratification of pathogen detections by site type provides a basis for targeted, evidence-informed infection prevention recommendations adapted to the arid indoor-city context of Riyadh (Figure S5).
Hospitals
Hospital detections were dominated by respiratory pathogens (adenovirus, rhinovirus/enterovirus), with one enteric indicator detection (EAEC) on a toilet door handle. Cleaning protocols should employ disinfectants with documented efficacy against both enveloped and non-enveloped viruses, as standard alcohol-based products are suboptimal for non-enveloped adenovirus [66,67]. Cleaning frequency should be increased for waiting area seating and toilet door handles, with particular attention to pediatric areas where rhinovirus shedding is highest. The co-detection of adenovirus and EAEC on a toilet door handle (HP-10) supports the recommendation that hospital restroom surfaces be treated as dual-risk sites requiring disinfection active against both respiratory and enteric organisms.
Airports
Airports exhibited the broadest pathogen diversity per site type, including respiratory viruses (SARS-CoV-2, rhinovirus, CoV-229E), Cryptosporidium, and B. pertussis. Intensified disinfection protocols may be warranted for toilet doorknobs, food court tables, and ATM keypads during and after peak passenger traffic periods associated with Hajj, Umrah, and Riyadh Season [68]. Environmental surveillance could be integrated into public health screening at international arrival points, and the baseline contamination rates established in this study may inform future exploratory threshold development for triggering enhanced cleaning responses. Touchless alternatives for high-frequency interfaces (payment terminals, check-in kiosks) merit consideration.
ATMs and Banking Surfaces
The finding that all ATM-positive pools contained Cryptosporidium only represents the most actionable infection prevention signal in this dataset. If alcohol-based wipes are used for routine ATM maintenance, they are ineffective against protozoan oocysts [69]. Facilities could transition to oocysticidal agents with demonstrated efficacy: hydrogen peroxide-based disinfectants [69], high-concentration sodium hypochlorite [70], or UV-C irradiation [69] for routine ATM cleaning. Installation of hand sanitizer stations adjacent to ATM kiosks may serve as a complementary measure. The acceleration of contactless and NFC payment technology in Saudi Arabia’s Vision 2030 digital transformation agenda offers a structural solution that reduces the reliance on shared keypads entirely.
Community Sites
Community settings exhibited the greatest pathogen diversity (7 of 10 detected pathogens), including enteric pathogens (V. cholerae, Salmonella, EAEC, EPEC, Cryptosporidium) alongside SARS-CoV-2 and adenovirus. Improved sanitation targeting enteric pathogens in public parks and cafes, public education on hand hygiene after using shared surfaces, and municipal coordination on restroom maintenance are the primary interventions. The temporal clustering of V. cholerae in March 2023 merits further investigation of water quality at the implicated community sites.
Seasonal Adaptation
A critical operational implication of the Indoor City framework is that cleaning intensification for respiratory viruses should not be limited to winter months. In Riyadh, the finding that 100% of warm-season detections were viral—a pattern consistent with increased indoor crowding during extreme outdoor heat—indicates that summer likely represents a period of elevated respiratory virus contamination risk on indoor surfaces. Infection prevention protocols should therefore align with indoor occupancy cycles (school terms, Ramadan evening economy, summer commercial activity) rather than outdoor meteorological seasons.
4.4. Study Limitations
Molecular Detection and Viability
All detections in this study were based on nucleic acid amplification and therefore indicate the presence of pathogen genetic material rather than infectious organisms. PCR detects both intact and degraded particles; viability assays such as cell culture or propidium monoazide (PMA)–PCR provide closer estimates of infectious risk but are more laborious, less sensitive, and inapplicable to non-culturable organisms, including norovirus and Cryptosporidium [71]. For enveloped viruses such as SARS-CoV-2, RNA persistence on surfaces substantially exceeds infectivity: viral RNA remains detectable for days after culturable virus is no longer recoverable [72]. The high Ct values observed for most detections (>35 for 7 of 10 detected pathogen categories) suggest that the majority represent non-viable nucleic acid remnants rather than actively infectious material. However, SARS-CoV-2 detections at Ct 33.9–34.8 may indicate more recent contamination events with higher residual pathogen loads. Importantly, Ct interpretation is assay-, matrix-, and target-dependent, and no universal Ct threshold can reliably infer infectivity from environmental surface samples.
Despite this limitation, environmental molecular surveillance—whether applied to surfaces, air, or wastewater—is an internationally recognized tool for public health monitoring and outbreak early warning that relies on nucleic acid detection by design [73]. Detection of pathogen nucleic acid on a surface provides actionable information even in the absence of viability data: it confirms that contamination pathways exist, identifies hygiene failures at specific locations, and provides early signals of pathogen circulation in a community before clinical cases accumulate. For structurally robust organisms—Cryptosporidium oocysts, adenovirus capsids—nucleic acid detection correlates more strongly with viability than for fragile enveloped viruses, because the structural integrity that protects nucleic acid also preserves infectivity. Viability assessment using cell culture and PMA-PCR for selected pathogens is identified as a priority for future confirmatory studies. Specifically, PMA-PCR can distinguish intact from membrane-compromised organisms without culture, while cell culture remains the reference standard for culturable viruses; combining both approaches would better quantify infectious risk from environmental surface samples.
Pooling Strategy
The 5-sample pooling strategy improved feasibility and coverage but prevents attribution of positive results to specific individual swabs within a pool. At the expected low background positivity (<5%), the theoretical sensitivity loss from pooling is marginal (approximately 2.3 Ct shift); however, empirical validation of pooling sensitivity was not performed with this specific sample matrix. The pooled design is therefore appropriate for baseline surveillance and hypothesis generation but not for individual-surface risk quantification.
Sample Size and Statistical Power
Of 55 pooled samples, 19 were positive, yielding 10 viral-positive and 9 non-viral-positive pools for the binary logistic regression. The study was not formally powered to detect the observed effect size, and the sample of positive pools (n = 19) constrains statistical power for multivariable models and subgroup analyses. The statistically significant result (p = 0.032) should therefore be interpreted as hypothesis-generating rather than confirmatory. Statistically non-significant results (e.g., humidity as a predictor) should be interpreted as “insufficient evidence” rather than “evidence of no effect.” Future studies with larger sample sizes across multiple seasons are needed to confirm these preliminary associations.
Meteorological Measurement
Temperature and humidity were measured as outdoor ambient conditions at or near sampling time. The Indoor City framework highlights the structural mismatch between outdoor meteorological variables and the indoor microenvironments where pathogen persistence actually occurs. Future surveillance should incorporate indoor temperature and humidity monitoring as primary predictors rather than relying exclusively on outdoor data.
Environmental Variables and Analytical Scope
While we collected data on broader meteorological variables—including UV index, AQI, wind speed, and pollen—the sample size of 19 positive pools precluded the application of complex multivariable or machine learning models, which would risk severe overfitting and yield unstable estimates. Exploratory analyses of these variables are presented in Figure S3. Future large-scale surveillance efforts should integrate these additional variables with advanced predictive modeling to build on the baseline established here.
Generalizability
The study was conducted in a single city during a defined post-pandemic period (February 2023–May 2024). Context-specific factors—building design, HVAC configurations, cleaning regimes, population density—may limit transferability of findings to other arid megacities, though the theoretical framework may be broadly applicable to Gulf Cooperation Council (GCC) cities with similar climate and infrastructure profiles.
4.5. Future Directions: Toward Predictive Environmental Surveillance
The significant associations between temperature and viral detection (OR = 1.728, p = 0.032), UV index category and viral detection (Fisher’s exact p = 0.036), and the elevated co-detection frequency (31.6% observed vs. 19.8% expected), suggest that surface contamination is governed by multi-factor interactions rather than single-variable drivers. This motivates a shift from univariate approaches toward integrative predictive frameworks. Environmental trend analyses across all sampling periods are presented in Figure S7.
Machine learning algorithms have been increasingly applied to model non-linear relationships between environmental factors and pathogen dynamics. Ensemble methods (gradient boosting, random forest) and Gaussian process regression have demonstrated moderate explanatory power for predicting respiratory disease occurrence from climate and air pollution data [74]. Explainable AI approaches, particularly SHAP (SHapley Additive exPlanations) analysis, can identify which environmental variables contribute most to model predictions, providing interpretable outputs suitable for public health decision-making [75]. Hybrid approaches combining ML with compartmental epidemiological models (e.g., SIR frameworks) show promise for handling time-dependent environmental influences [76].
We propose a stage-by-stage framework, building on the baseline established here. Stage 1 (feature expansion): future studies should incorporate lagged environmental effects (7–21-day windows for temperature, humidity, UV, AQI), composite indices, spatial connectivity metrics, and temporal features (Hajj/Umrah calendars, school terms). Stage 2 (model development): this stage comprises the use of a substantially larger dataset (e.g., hundreds of pools) and penalized regression (LASSO, elastic net) for variable selection, followed by the application of ensemble methods for non-linear interaction capture; the current dataset (N = 55, 19 positive) provides baseline prevalence and effect sizes for power calculation but is insufficient for stable model training. Stage 3 (deployment): this stage involves model outputs translated into operational risk scores compatible with existing municipal cleaning schedules, enabling proactive risk management aligned with Saudi Vision 2030 public health objectives.
Several challenges must be acknowledged. Data quality remains a primary constraint: the current study’s reliance on outdoor ambient conditions rather than indoor microenvironmental measurements introduces measurement error. While correlations between environmental variables and pathogen detection exist, establishing direct causal links remains complex due to multiple mediating behavioral pathways. Interpretability must be prioritized: complex models can function as opaque predictors that limit their utility for operational public health decisions. Future studies should incorporate indoor temperature and humidity monitoring, direct PM_2_.5/PM_10_ measurements, and foot traffic data as primary predictors.
5. Conclusions
This study provides the first city-wide molecular baseline of surface pathogen contamination across diverse public and clinical environments in an arid megacity. The overall positivity rate of 34.5% across 55 pooled samples demonstrates frequent molecular evidence of pathogen contamination on Riyadh’s urban surfaces despite the common assumption that extreme arid heat sharply reduces environmental pathogen persistence. The detection of 10 distinct pathogens—4 respiratory viruses, 1 parasite, and 5 bacterial pathogens—at the species or genus level reveals contamination signatures that are both site-specific and seasonally structured.
The statistically significant association between higher ambient temperature and viral detection among positive pools (OR = 1.728, p = 0.032; AUC = 0.756) provides preliminary empirical support consistent with the Indoor City hypothesis: in arid megacities where extreme outdoor heat drives populations into climate-controlled indoor spaces, indoor surfaces serve as recurring sites of respiratory virus contamination even during peak summer. This framework challenges conventional seasonality models and has direct implications for the timing and targeting of infection prevention efforts in Gulf cities.
The following evidence-informed recommendations emerge from the pathogen–site associations identified in this study. Hospitals could employ broad-spectrum disinfectants effective against both enveloped and non-enveloped viruses, with increased cleaning frequency in waiting areas and pediatric zones. Airports may warrant enhanced disinfection during peak passenger periods (Hajj, Umrah, Riyadh Season) with consideration of environmental surveillance as a complementary input to public health screening and adoption of touchless interfaces. ATM disinfection protocols could transition from alcohol-based wipes to oocysticidal agents (hydrogen peroxide, sodium hypochlorite, or UV-C irradiation), complemented by hand sanitizer stations and accelerated adoption of contactless payment technology. Community sites would benefit from improved sanitation targeting enteric pathogens, public hand hygiene education, and coordinated municipal restroom maintenance.
A critical operational implication of the Indoor City framework is that cleaning intensification for respiratory viruses could be aligned with indoor occupancy cycles—school terms, Ramadan evening economy, summer commercial activity—rather than outdoor meteorological seasons. In arid megacities, peak summer indoor crowding likely represents a period of elevated respiratory virus contamination risk on indoor surfaces that conventional winter-focused protocols do not address.
Establishing baseline surface contamination profiles, as demonstrated here, provides the foundation for sentinel environmental surveillance systems capable of detecting deviations from baseline that may signal emerging outbreaks. Integration of environmental monitoring data with clinical surveillance through digital health platforms represents a future priority for enhancing public health preparedness in Saudi Arabia and comparable arid urban environments worldwide.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leung N. Transmissibility and Transmission of Respiratory Viruses Nat. Rev. Microbiol.20211952854510.1038/s 41579-021-00535-633753932 PMC 7982882 · doi ↗ · pubmed ↗
- 2Castaño N. Cordts S. Jalil M.K. Zhang K. Koppaka S. Bick A. Paul R. Tang S. Fomite Transmission, Physicochemical Origin of Virus–Surface Interactions, and Disinfection Strategies for Enveloped Viruses with Applications to SARS-Co V-2ACS Omega 202166509652710.1021/acsomega.0c 0633533748563 PMC 7944398 · doi ↗ · pubmed ↗
- 3Ackerley L. Cooper S. Upson S. Paskey A. Gent L. Buckley C. Spitzer M. Sexton J. Picton J. Reynolds K. Who Touched That? Interconnection of High-Touch Surfaces Drives Pathogen Spread in Public Spaces Eur. J. Public Health 202333 ckad 160.99510.1093/eurpub/ckad 160.995 · doi ↗
- 4Wang P. Zhang N. Miao T. Chan J.P.T. Huang H. Lee P.K.H. Li Y. Surface Touch Network Structure Determines Bacterial Contamination Spread on Surfaces and Occupant Exposure J. Hazard. Mater.202141612613710.1016/j.jhazmat.2021.12613734492926 · doi ↗ · pubmed ↗
- 5Arienzo A. Gallo V. Tomassetti F. Pitaro N. Pitaro M. Antonini G. A Narrative Review of Alternative Transmission Routes of COVID 19: What We Know so Far Pathog. Glob. Health 202311768169510.1080/20477724.2023.222804837350182 PMC 10614718 · doi ↗ · pubmed ↗
- 6Moriyama M. Hugentobler W.J. Iwasaki A. Seasonality of Respiratory Viral Infections Annu. Rev. Virol.202078310110.1146/annurev-virology-012420-02244532196426 · doi ↗ · pubmed ↗
- 7Sooryanarain H. Elankumaran S. Environmental Role in Influenza Virus Outbreaks Annu. Rev. Anim. Biosci.2015334737310.1146/annurev-animal-022114-11101725422855 · doi ↗ · pubmed ↗
- 8Dasari H.P. Desamsetti S. Langodan S. Viswanadhapalli Y. Hoteit I. Analysis of Outdoor Thermal Discomfort Over the Kingdom of Saudi Arabia Geohealth 20215 e 2020 GH 00037010.1029/2020 GH 000370 PMC 818228034141978 · doi ↗ · pubmed ↗