From acute diagnosis to longitudinal risk stratification: a paradigm shift in the clinical role of cardiac biomarkers
Hong Zheng, Xue Li, Li-Jiao Guo, Guang-Ling Ji, Hong-Tao Liu, Yue Zheng, Jie Zhou

TL;DR
This paper discusses how cardiac biomarkers are shifting from diagnosing acute issues to managing long-term cardiovascular risks.
Contribution
The paper introduces a new framework for using cardiac biomarkers in longitudinal risk stratification and disease management.
Findings
Biomarkers can inform prevention, early detection, and chronic monitoring of cardiovascular disease.
Multi-biomarker panels and AI-based models are key strategies for implementation.
Challenges include standardization, interpretation, and cost-effectiveness of biomarker use.
Abstract
This perspective examines the evolving role of cardiac biomarkers from acute diagnostic tools to integral components of longitudinal risk stratification and cardiovascular disease management. Evidence from cohort studies, clinical trials, and high-sensitivity assays demonstrates that biomarkers reflecting myocardial injury, hemodynamic stress, inflammation, fibrosis, and metabolic dysfunction can inform prevention, early detection, acute care, and chronic monitoring. Key implementation strategies include multi-biomarker panels, serial measurements, multi-omics integration, and artificial intelligence-based risk modeling. Challenges such as assay standardization, clinical interpretation, and cost-effectiveness are critically evaluated. Overall, this framework highlights the potential for biomarker-guided approaches to promote more preventive, precise, and patient-centered cardiovascular…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
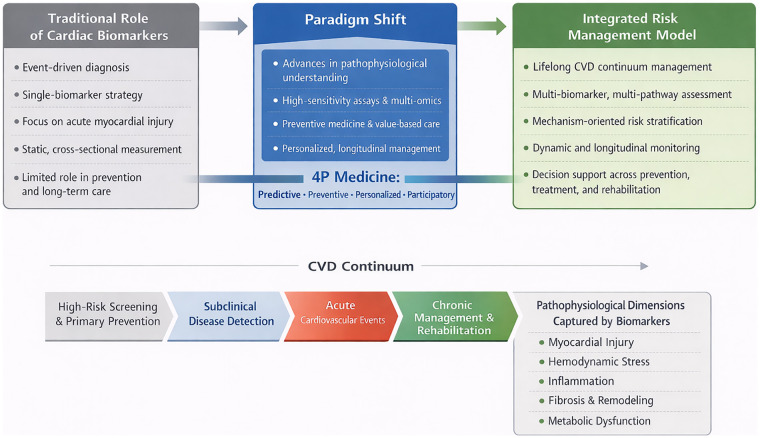 Figure 1
Figure 1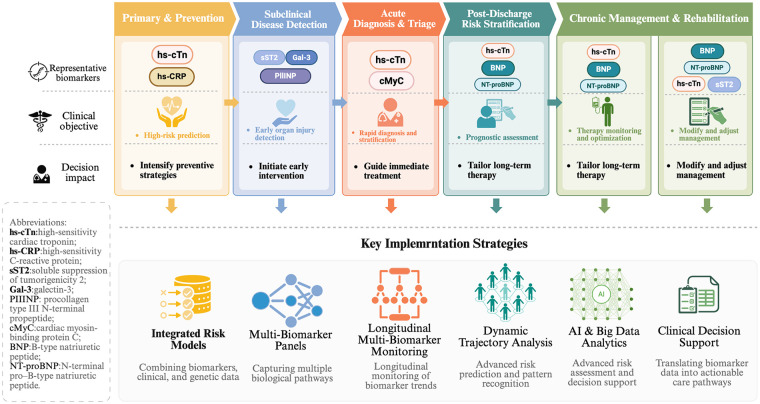 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIL-33, ST2, and ILC Pathways · Cardiac Fibrosis and Remodeling · Biomarkers in Disease Mechanisms
Introduction
1
Cardiovascular disease (CVD) continues to be a primary cause of death and disability worldwide, presenting a persistent and substantial public health challenge (1). This burden underscores the need for management strategies that address CVD across its entire disease spectrum rather than focusing solely on acute events (2). Established cardiac biomarkers, particularly cardiac troponin (cTn) and B-type natriuretic peptide (BNP/NT-proBNP), have long served essential roles in clinical practice (3). Traditionally, their clinical use has predominantly focused on diagnosing acute cardiovascular conditions—such as myocardial infarction or acute heart failure—and on offering limited short-term prognostic evaluation (4). This reactive, event-centered approach provides limited insight into early disease processes and offers insufficient support for long-term risk stratification or primary prevention (5).
Concurrently, medical practice is undergoing a broader transformation from reactive disease treatment toward a proactive model grounded in Predictive, Preventive, Personalized, and Participatory (4P) medicine (6). This shift requires clinical tools capable of identifying risk at earlier stages, monitoring disease trajectories over time, and guiding intervention across different phases of disease progression (4, 6). Within this evolving framework, the clinical function of cardiac biomarkers is a significant conceptual transition.
This transition represents a paradigm shift. Rather than serving solely as diagnostic indicators of acute events, cardiac biomarkers are increasingly deployed as dynamic, multidimensional tools for integrated risk management throughout the full CVD continuum (Figure 1). This continuum encompasses the high-risk phase (screening and primary prevention), the subclinical phase (detection of early organ injury), the acute phase (rapid diagnosis and initial risk stratification), and the chronic or rehabilitative phase (treatment response monitoring, prognosis, and secondary prevention) (7). The growing availability of biomarkers that reflect myocardial stress, fibrosis, inflammation, and metabolic dysfunction has further expanded the scope of cardiovascular risk evaluation (7, 8).
Paradigm shift in the role of cardiac biomarkers across the cardiovascular disease continuum. This figure illustrates the transition from an event-centered use of cardiac biomarkers toward a longitudinal, risk-based management framework. Biomarker applications are mapped across four major stages: high-risk screening and primary prevention, subclinical disease detection, acute diagnosis and risk stratification, and chronic disease management and rehabilitation. At each stage, biomarkers reflect distinct underlying pathophysiological processes, including myocardial injury, hemodynamic stress, inflammation, fibrosis, and metabolic dysfunction, thereby supporting stage-specific clinical decision-making.
Ultimately, contemporary cardiac biomarkers are increasingly positioned as core components of modern CVD management (4). By capturing distinct pathophysiological processes at different disease stages, these biomarkers help bridge underlying biological mechanisms with objective risk assessment and individualized clinical decision-making (4, 9). This integration supports a transition toward a more anticipatory, precise, and systematically organized model of cardiovascular care.
This perspective defines the proposed “paradigm shift” as a coordinated transition in three interrelated dimensions. It is crucial to clarify that this article adopts a narrative perspective rather than constituting a systematic review. The referenced literature was selected to exemplify pivotal conceptual advances, landmark clinical trials, and pertinent population-based studies within biomarker-guided risk management and does not constitute a comprehensive summary of the entire evidence base. The first dimension involves a fundamental change in the application of biomarkers, from tools for discrete event detection to instruments for longitudinal, dynamic risk surveillance. The second dimension concerns a shift in analytical strategy, from assessing individual biomarkers in isolation toward integrating multi-marker profiles that reflect complementary pathophysiological mechanisms. The third dimension represents an evolution in clinical intent, from a reactive model focused on diagnosis toward a proactive model prioritizing risk prediction, preventive intervention, and personalized treatment optimization. Collectively, these dimensions form a unified conceptual framework that distinguishes modern, biomarker-guided cardiovascular care from traditional diagnostic approaches.
To ensure the precision of this framework, it is essential to acknowledge a critical epistemological caveat that underpins the entire discussion. The proactive model proposed here is fundamentally built upon the capacity of biomarkers to stratify risk. Therefore, before elaborating on the applications of this paradigm, a clear operational distinction should be made. Clinical validity refers to a biomarker's ability to provide independent or incremental prognostic information beyond established risk factors. In contrast, clinical utility requires evidence that acting on that information leads to improved patient-centered outcomes. In many domains discussed in this perspective, the current evidence base more robustly supports clinical validity than definitive outcome improvement through biomarker-guided intervention. Consequently, any subsequent references to prevention or treatment optimization should be interpreted primarily within the context of risk stratification potential-identifying individuals or populations at higher likelihood of future events-rather than implying proven strategies for modifying those outcomes. This distinction safeguards against overinterpretation and aligns the discourse with the current standards of evidence-based medicine (10).
Theoretical basis and driving forces of the paradigm shift
2
The evolution in the role of cardiac biomarkers in CVD management reflects a broader transformation in modern medicine. This paradigm shift arises from multiple, interrelated developments and marks a transition from reactive, event-driven care toward proactive, mechanism-based, and integrated disease management.
Advances in pathophysiological insight
2.1
Traditionally, cardiac biomarkers such as cardiac troponin were primarily used to detect acute myocardial injury, particularly myocardial necrosis. Contemporary research, however, recognizes CVD as a continuous process characterized by interacting pathophysiological mechanisms, including myocardial stress, fibrosis, chronic low-grade inflammation, and metabolic dysregulation (11). This expanded understanding has driven the development and clinical adoption of a broader biomarker spectrum. Natriuretic peptides reflect myocardial wall stress and volume overload. Soluble suppression of tumorigenicity 2 (sST2) and procollagen type III N-terminal peptide provide insight into myocardial fibrosis and remodeling (12–14). High-sensitivity C-reactive protein (hs-CRP) extends beyond a general marker of systemic inflammation; it specifically reflects chronic low-grade vascular inflammation, which directly contributes to endothelial dysfunction and atherogenesis (15–17). Elevated hs-CRP levels are consistently associated with a higher risk of major adverse cardiovascular events, including myocardial infarction, stroke, and cardiovascular mortality, independent of traditional risk factors (18). Crucially, hs-CRN provides incremental prognostic value beyond markers of myocardial injury and hemodynamic stress, thereby capturing the distinct contribution of inflammatory pathways to cardiovascular risk—a dimension not assessed by cardiac-specific biomarkers alone.
Overall, these markers enable clinicians to monitor disease progression across its stages, moving beyond acute diagnosis toward continuous risk assessment. These advances collectively support a transition from an event-centered interpretation of biomarkers toward the continuous monitoring of underlying disease mechanisms.
Technological progress in biomarker measurement
2.2
Technological advances in biomarker measurement have been central to this paradigm shift. High-sensitivity assays can now detect biomarkers at very low concentrations, uncovering subclinical myocardial injury that was previously undetectable (19). In parallel, multi-omics technologies—particularly proteomics and metabolomics— enable systematic discovery of novel biomarker signatures and provide deeper insight into disease-specific molecular networks (20). These approaches enhance mechanistic understanding and support more refined risk stratification. Point-of-care testing platforms further expand clinical applicability by enabling rapid biomarker assessment in diverse settings, including primary care, emergency departments, and resource-limited environments (21). Collectively, these technological developments allow biomarkers to be applied earlier, measured more frequently, and used across a wider range of clinical contexts than was previously feasible.
Evolving demands in clinical practice
2.3
Clinical practice increasingly requires tools that support long-term cardiovascular risk management rather than solely acute diagnosis. Several needs drive this shift (22–25). First, precise risk stratification is required to identify high-risk individuals before clinical symptoms develop. Second, early detection of potentially reversible pathological changes enables timely intervention. Third, biomarker profiles can inform individualized treatment selection. Finally, longitudinal monitoring supports assessment of therapeutic response and adjustment of management strategies over time. These demands reflect a broader movement toward personalized and evidence-based care. Biomarkers are increasingly expected to guide decision-making across the entire disease trajectory, rather than serving a single diagnostic purpose.
Influence of preventive medicine and value-based care
2.4
Broader healthcare trends further reinforce this transformation. Preventive medicine emphasizes early risk detection and primary prevention, encouraging biomarker use before overt disease develops (4). At the same time, value-based care prioritizes improved long-term outcomes while optimizing healthcare resources (26). Biomarkers contribute to these goals by improving risk prediction accuracy, supporting targeted interventions, and reducing unnecessary testing or treatment. In this context, biomarker-guided strategies align clinical decision-making with both patient-centered outcomes and healthcare system sustainability (4, 10). Together, these advances in pathophysiology, technology, clinical practice, and healthcare priorities explain why cardiac biomarkers are increasingly used for ongoing cardiovascular risk management, rather than only for event-based diagnosis.
In summary, this paradigm shift results from converging advances in disease biology, measurement technology, clinical expectations, and healthcare priorities. Cardiac biomarkers are no longer limited to diagnostic confirmation of acute events. Instead, they have become essential tools for predicting risk, guiding prevention, and managing CVD across its entire course.
Core application scenarios and biomarker profiles in the new paradigm
3
This integrated approach is necessitated by the pathophysiological complexity and temporal evolution of cardiovascular disease. Consequently, biomarkers should be evaluated based on their distinct biological mechanisms and stage-specific clinical validities. This rationale leads to their classification into dedicated categories, such as those indicative of myocardial injury [e.g., high-sensitivity cardiac troponin (hs-cTn)], hemodynamic stress (e.g., BNP/NT-proBNP), inflammation (e.g., hs-CRP), fibrosis and remodeling (e.g., sST2, galectin-3), and cellular stress (e.g., growth differentiation factor 15). Accordingly, specific biomarker profiles align with particular disease stages and underlying pathophysiological mechanisms (Supplementary Table S1). Moving beyond isolated or supplementary use, biomarkers are increasingly combined and measured longitudinally. This approach enables continuous risk evaluation and supports dynamic clinical decision-making. This systematic application of biomarkers, as demonstrated across the following scenarios, provides a structured and clinically applicable framework that aligns biomarker use with disease stage, encompassing the full spectrum from prevention and diagnosis to treatment and long-term follow-up.
Primary prevention and high-risk population screening
3.1
In primary prevention, biomarkers help identify individuals with subclinical myocardial injury or persistent cardiac stress before symptoms manifest. Elevated hs-cTn reflects minor cardiomyocyte injury or turnover, while BNP/NT-proBNP indicates myocardial wall stress and volume overload (3, 27). Hs-CRP provides information on low-grade systemic inflammation (28). Even modest and sustained elevations in these biomarkers are independently associated with increased cardiovascular risk in asymptomatic individuals. In preventive cardiology, biomarker-based risk stratification is particularly valuable for identifying high-risk individuals who may not be recognized by conventional risk assessment models. The integration of hs-cTn, natriuretic peptides, and inflammatory markers facilitates the earlier detection of not only myocardial injury and subclinical cardiac stress but also underlying vascular inflammation (29–31). This comprehensive biomarker profile enables a more precise estimation of cardiovascular risk than traditional factors alone (3). Consequently, this approach supports early lifestyle modification and preventive pharmacological interventions in populations that may otherwise be considered low risk based on traditional factors.
However, despite these promising associations, the implementation of biomarker-based screening in primary prevention is not without potential harms. High-sensitivity assays may detect low-level biomarker elevations unrelated to modifiable cardiovascular pathology, particularly in populations such as older adults or those with chronic kidney disease, where baseline troponin and natriuretic peptide levels are often chronically elevated (32, 33). Such findings may lead to false-positive classifications, overestimation of risk, and downstream consequences including unnecessary diagnostic testing, increased healthcare utilization, potential overtreatment, and patient anxiety (34). Moreover, indiscriminate screening risks exacerbating health disparities, especially when access to confirmatory testing and follow-up care is unevenly distributed. Therefore, for biomarker-informed screening to be both clinically effective and equitable, implementation should occur within structured risk assessment frameworks and supported by rigorous cost-effectiveness, calibration and equity analyses (4, 34).
Early disease detection and subclinical management
3.2
This stage focuses on identifying structural and functional cardiac abnormalities before overt clinical disease develops. Biomarkers such as sST2 and galectin-3 reflect fibrotic and inflammatory processes involved in myocardial remodeling. Growth differentiation factor-15, a stress-responsive cytokine, is associated with early atherosclerosis and heart failure risk (35, 36). By revealing early pathological changes, these biomarkers facilitate timely intervention. They support proactive management of patients with occult coronary disease or early myocardial dysfunction, potentially slowing disease progression.
Rapid diagnosis and differential diagnosis of acute cardiovascular events
3.3
In acute care settings, biomarkers play a critical role in rapid diagnosis and triage. Serial measurements of hs-cTn using accelerated diagnostic algorithms are central to the early diagnosis of acute myocardial infarction (37–39). Emerging biomarkers, such as cardiac myosin-binding protein C, demonstrate faster release kinetics than traditional troponins. These characteristics may improve very early diagnosis and enhance decision-making in emergency departments, reducing delays to definitive treatment (40).
In-Hospital and post-discharge risk stratification and prognosis
3.4
Beyond diagnosis, biomarkers provide important prognostic information during hospitalization and after discharge. Elevated levels of hs-cTn, natriuretic peptides, and inflammatory markers are associated with increased risk of mortality and rehospitalization (41). Multi-marker strategies combine complementary biological information. For example, integrating markers of myocardial injury, hemodynamic stress, and inflammation improves risk stratification and helps identify patients who may benefit from intensified treatment or closer follow-up (42).
From a prognostic perspective, hs-CRP improves risk stratification in multi-marker panels by capturing systemic inflammation, a process closely associated with adverse cardiac remodeling and recurrent cardiovascular events (43). While hs-cTn indicates myocardial injury and natriuretic peptides reflect hemodynamic stress, hs-CRP provides complementary information on this distinct inflammatory pathway (44). Patients with persistently elevated hs-CRP levels after an acute cardiovascular event demonstrate significantly higher rates of rehospitalization and mortality, underscoring its specific utility for post-discharge risk assessment (45).
Chronic disease management: treatment guidance and monitoring
3.5
In chronic cardiovascular conditions, particularly heart failure, biomarkers are valuable for guiding therapy and monitoring response. Changes in natriuretic peptide levels reflect hemodynamic status and treatment effectiveness. A sustained reduction after initiation of guideline-directed medical therapy is associated with improved clinical outcomes (46, 47). Serial biomarker measurements support individualized treatment titration and enable a treat-to-target approach. Integrating biomarker data with clinical evaluation enables more nuanced therapeutic decision-making. Although reductions in natriuretic peptides correlate with favorable prognosis and some trials suggest benefit from biomarker-guided strategies, evidence for consistent improvement in hard clinical endpoints across heterogeneous populations remains inconclusive (48). Accordingly, serial biomarker monitoring is best regarded as a tool for enhanced risk stratification rather than a validated treat-to-target mandate (48).
Emerging applications: cardiotoxicity monitoring and cardiac rehabilitation
3.6
Biomarkers also play an expanding role in specialized clinical settings. In cardio-oncology, hs-cTn and natriuretic peptides are increasingly used to detect early chemotherapy-related cardiotoxicity, allowing timely implementation of cardioprotective strategies (49, 50). In cardiac rehabilitation, longitudinal biomarker trends may objectively reflect physiological improvement, such as reduced myocardial stress or favorable remodeling. These measurements can help tailor rehabilitation intensity and monitor treatment effectiveness (51, 52).
In summary, biomarkers in the new paradigm are applied in a structured and stage-specific manner across the cardiovascular disease spectrum (Figure 2). By aligning biomarker categories with disease stage and clinical purpose, this framework provides clinicians with a practical reference for biomarker selection and interpretation. Integrated use of biomarkers across prevention, diagnosis, treatment, and follow-up supports a more proactive, individualized, and systematic approach to cardiovascular care.
Stage-Specific applications and implementation strategies of cardiac biomarkers. This figure presents an integrated clinical pathway illustrating how multi-biomarker panels, serial measurements, and data-driven analytics can be incorporated into routine cardiovascular care. Biomarkers are used to support risk stratification, guide treatment selection and titration, monitor therapeutic response, and inform prognosis. The framework emphasizes longitudinal assessment and dynamic risk re-evaluation, providing a practical reference for implementing biomarker-based strategies in prevention, acute care, and chronic disease management.
Key strategies and tools for achieving the paradigm shift
4
To achieve this shift in cardiac biomarker use—from simple diagnostic aids to core parts of risk management—a systematic set of strategies and innovative tools is essential. This will make biomarkers more useful in practice and support cardiovascular care that is precise, adaptable, and well-coordinated.
Integrated risk assessment models
4.1
The clinical value of a single biomarker is inherently limited. Its utility increases substantially when combined with complementary sources of information. Integrating biomarkers with traditional risk factors (e.g., blood pressure, lipid profiles), as well as imaging findings and genetic data, enables the construction of multidimensional risk assessment models (53). These integrated models improve risk stratification by identifying individuals who may be underestimated by conventional scores alone. They also support the definition of individualized treatment thresholds, which is essential for precision prevention (54). For example, combining high-sensitivity cardiac troponin with polygenic risk scores has been shown to enhance the prediction of future cardiovascular events in asymptomatic populations (53, 55). Such integrated models are particularly valuable in preventive care. They support personalized risk assessment and enable earlier, targeted interventions based on individual mechanisms, moving beyond uniform, population-wide prevention approaches. Overall, integrated risk models provide a more comprehensive and clinically actionable representation of cardiovascular risk.
Dynamic monitoring and trajectory analysis
4.2
Single biomarker measurements offer only a snapshot of disease status. In contrast, changes in biomarker levels over time often provide more clinically meaningful information. Longitudinal monitoring allows clinicians to assess disease progression and treatment response more accurately (56). In heart failure, rising natriuretic peptide levels may signal impending clinical deterioration, whereas sustained reductions are often associated with therapeutic benefit and improved prognosis (57). By focusing on trajectories rather than isolated values, clinicians can detect risk earlier and adjust therapy in a timely manner (58). Thus, dynamic monitoring shifts biomarker use from static interpretation toward longitudinal risk assessment. While trajectory-based evaluation may enhance prognostic accuracy, further prospective studies are needed to confirm that routine, trajectory-guided adjustments consistently lead to improved clinical outcomes.
Multi-biomarker panel strategies
4.3
Cardiovascular disease is driven by multiple overlapping pathophysiological processes. No single biomarker can adequately capture this complexity. Multi-biomarker panels address this limitation by combining markers that reflect distinct biological pathways, including myocardial injury, hemodynamic stress, inflammation, and fibrosis (59). This approach improves diagnostic accuracy and supports disease phenotyping, such as distinguishing inflammatory-dominant from fibrotic-dominant disease patterns. It also facilitates more targeted therapeutic decisions, thereby advancing precision cardiovascular medicine (60, 61). Multi-biomarker strategies therefore offer a more complete and clinically informative assessment than single-marker approaches.
Artificial intelligence and big data analytics
4.4
The increasing volume of clinical, laboratory, and multi-omics data exceeds the capacity of traditional analytical methods. Artificial intelligence and machine learning provide tools to manage this complexity and extract clinically relevant patterns (62). Artificial intelligence can process and analyze large and complex datasets beyond the reach of traditional statistical tools (63). In cardiovascular research, these datasets often encompass electronic health records, repeated biomarker measurements, medical images, and multi-omics data from extensive population studies (64). It is important to note, however, that not all studies employing these advanced analytical methods utilize true longitudinal trajectory modeling (65, 66). While some analyses are based on cross-sectional biomarker features or single baseline measurements, others explicitly integrate repeated measures over time (65, 67). This distinction is critical, as trajectory-based models, which leverage machine learning algorithms to model non-linear associations and track changes in biomarkers longitudinally (68), are better positioned to capture dynamic risk. Yet, they also require more complex data infrastructure and rigorous validation to ensure clinical utility.
This capability supports dynamic, individualized risk prediction that updates with new data, moving beyond static, one-time assessments (69). Consequently, these methods can identify novel biomarker signatures, optimize risk prediction models, and refine clinical decision pathways using large-scale real-world data (70). Importantly, studies have shown that machine learning models integrating biomarker data—particularly when leveraging repeated or longitudinal measurements—may improve discrimination metrics compared with conventional risk scores in selected datasets; however, such improvements are context dependent and have not been consistently replicated across diverse populations or clinical settings (62, 70, 71).
Recent population-based studies demonstrate that artificial intelligence-assisted biomarker models can be implemented at the health-system level to monitor cardiovascular risk in real time across large patient populations (72, 73). These models employ continuous learning frameworks, through which incoming clinical and laboratory data iteratively refine risk predictions (74). This process facilitates timely preventive interventions and supports personalized disease management.
The scalability of this approach is being confirmed. Recent large population-based studies from 2025 and early 2026 have not only demonstrated methodological feasibility and scalability within retrospective or observational datasets, but they also further illustrated the practicality of deploying artificial intelligence-assisted biomarker integration at the health system level for population-scale monitoring (75–78). Despite these advances, widespread real-world deployment with demonstrated clinical impact remains an ongoing area of investigation rather than an established standard of care. Collectively, these findings underscore the increasing practicality of incorporating machine learning-based biomarker models into routine clinical practice for real-time cardiovascular risk monitoring.
Before clinical implementation, machine learning-based biomarker models should meet several essential standards to ensure scientific robustness and ethical integrity. First, they should undergo rigorous external validation in independent and demographically diverse populations to confirm generalizability (79, 80). Second, models should demonstrate adequate calibration and transparently report discrimination metrics, including confidence intervals and decision-curve analyses where appropriate (79, 80). Third, algorithmic fairness should be systematically assessed to detect potential bias across sex, age, ethnicity, socioeconomic status, and comorbidity subgroups (80, 81). Fourth, continuous post-deployment surveillance is required to identify model drift and performance degradation over time (82). Fifth, and most critically, prospective evaluation of their impact on clinical decision-making and patient outcomes is necessary to establish true clinical utility (83). Without adherence to these safeguards, predictive performance alone cannot justify routine clinical integration.
In summary, artificial intelligence-driven biomarker analytics represent a powerful but methodologically demanding extension of precision cardiovascular medicine. Their promise lies in enhancing risk stratification and supporting dynamic decision-making; however, their clinical legitimacy ultimately depends on rigorous validation, transparent reporting, equitable performance, and demonstrable outcome benefit. Thoughtful integration of these safeguards is essential to translate computational innovation into meaningful improvements in cardiovascular care.
Challenges and future directions
5
Despite substantial progress, several barriers continue to limit the routine clinical implementation of biomarker-guided cardiovascular care. While biomarkers have advanced cardiovascular care, their routine use in clinical practice remains limited by structural, analytical, and implementation challenges. Addressing these challenges is essential for translating conceptual advances into sustained clinical benefit.
Key challenges
5.1
Four major challenges currently limit broader implementation. One major challenge is pre-analytical and analytical variability. Differences in sample collection, processing, and assay performance can significantly affect biomarker measurements. Without standardized protocols and validated reference ranges, results may not be comparable across clinical settings (84, 85). A second challenge lies in clinical interpretation. Biomarker levels can be influenced by comorbid conditions such as chronic kidney disease, obesity, or atrial fibrillation. These factors may reduce specificity for cardiac pathology and complicate clinical decision-making (86). Third, robust health economic evidence is often lacking. Cost-effectiveness analyses are needed to justify the broader use of biomarker-based screening and longitudinal monitoring compared with conventional strategies (87). Finally, barriers to clinical translation persist. These include delayed updates to clinical guidelines, variable clinician familiarity with newer biomarkers, and limited integration of biomarker data into electronic health records and clinical workflows (88).
Future directions
5.2
Future progress will require coordinated efforts in several key areas. First, multi-omics technologies such as proteomics and metabolomics are expected to yield more specific biomarkers aligned with distinct disease mechanisms and stages (89). Second, individualized biomarker thresholds should be developed. Adjusting cut-off values for factors such as age, sex, renal function, and comorbidities may improve both diagnostic and prognostic accuracy (90). Third, digital integration should be strengthened. Embedding serial biomarker data into electronic health records and clinical decision support systems would enable dynamic risk assessment and personalized treatment guidance (91, 92). Finally, prospective biomarker-guided interventional trials are needed. Such studies are essential to determine whether biomarker-driven strategies can improve hard clinical outcomes, including mortality and hospitalization rates (93).
Rather than proposing novel biomarkers, this perspective's key contribution lies in rethinking how both established and emerging biomarkers can be deployed along longitudinal, stage-specific care pathways. This integrated framework moves beyond describing biomarker-disease associations toward actionable, system-level strategies. These strategies align biomarker application with preventive cardiology, treatment individualization, and sustainable health system design. The novelty of this paradigm lies in its integrated approach, not in discovering single biomarkers. It systematically embeds biomarkers into longitudinal care pathways, connecting prevention, treatment optimization, and value-based healthcare delivery.
Addressing these challenges and pursuing these strategies will help turn biomarkers from research tools into practical parts of cardiovascular care. This will support more precise, evidence-based, and personalized patient management.
Summary
6
The clinical role of cardiac biomarkers has evolved substantially. Once used mainly for the diagnosis of acute events, they are now integral to comprehensive and personalized cardiovascular risk assessment across all stages of disease. This evolution reflects a broader shift from reactive diagnosis to proactive risk prediction, from isolated measurements to longitudinal monitoring, and from uniform treatment strategies to individualized management.
Realizing the full potential of this paradigm will require close collaboration among laboratory medicine, cardiology, epidemiology, and data science. Key priorities include assay standardization, effective integration of biomarker data into clinical workflows, and the generation of high-quality evidence to guide practice. Through these efforts, biomarker-guided strategies can support a more preventive, precise, and patient-centered model of cardiovascular care, with the ultimate goal of improving long-term outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yang H Ma Q Han L Liu H. A global prediction of cardiovascular disease from 2020 to 2030. Front Cardiovasc Med. (2025) 12:1462705. 10.3389/fcvm.2025.146270540860359 PMC 12375611 · doi ↗ · pubmed ↗
- 2Victor G Shishani K Vellone E Froelicher ES. The global burden of cardiovascular disease in adults: a mapping review. J Cardiovasc Nurs. (2025). 10.1097/JCN.000000000000120040179360 · doi ↗ · pubmed ↗
- 3Everett BM Zeller T Glynn RJ Ridker PM Blankenberg S. High-sensitivity cardiac troponin I and B-type natriuretic peptide as predictors of vascular events in primary prevention: impact of statin therapy. Circulation. (2015) 131(21):1851–60. 10.1161/CIRCULATIONAHA.114.01452225825410 PMC 4444427 · doi ↗ · pubmed ↗
- 4Neumann JT de Lemos JA Apple FS Leong DP. Cardiovascular biomarkers for risk stratification in primary prevention. Eur Heart J. (2025) 46(39):3823–43. 10.1093/eurheartj/ehaf 51740795138 · doi ↗ · pubmed ↗
- 5Neumann JT Twerenbold R Weimann J Ballantyne CM Benjamin EJ Costanzo S Prognostic value of cardiovascular biomarkers in the population. JAMA. (2024) 331(22):1898–909. 10.1001/jama.2024.559638739396 PMC 11091824 · doi ↗ · pubmed ↗
- 6Sagner M Mc Neil A Puska P Auffray C Price ND Hood L The P 4 health Spectrum - A predictive, preventive, personalized and participatory Continuum for promoting healthspan. Prog Cardiovasc Dis. (2017) 59(5):506–21. 10.1016/j.pcad.2016.08.00227546358 · doi ↗ · pubmed ↗
- 7Thupakula S Nimmala SSR Ravula H Chekuri S Padiya R. Emerging biomarkers for the detection of cardiovascular diseases. Egypt Heart J. (2022) 74(1):77. 10.1186/s 43044-022-00317-236264449 PMC 9584006 · doi ↗ · pubmed ↗
- 8Kurt B Rex K Reugels M Fordyce CB Fudim M Sharma A Inflammatory biomarkers in heart failure: clinical perspectives on hs CRP, IL-6 and emerging candidates. Curr Heart Fail Rep. (2025) 22(1):35. 10.1007/s 11897-025-00710-341196450 PMC 12592283 · doi ↗ · pubmed ↗