Amebic liver abscess with bronchopleural fistula
Michaela Schumacher, Andrea Erba, Seraina Bally, Seraina Frei, Maja Weisser Rohacek, Andreas Neumayr, Anne-Valérie Burgener-Gasser

TL;DR
Amebic liver abscess with a bronchopleural fistula in a traveler was diagnosed quickly using PCR, avoiding unnecessary antibiotics.
Contribution
Rapid diagnosis of amebic liver abscess using PCR on abscess fluid is highlighted as a novel approach for targeted treatment.
Findings
PCR on abscess fluid enabled rapid diagnosis of amebic liver abscess.
Targeted therapy was initiated within 24 hours, avoiding broad-spectrum antibiotics.
Abstract
Amebic liver abscess with bronchopleural fistula caused by Entamoeba histolytica can mimic severe bacterial sepsis in a returning traveller. Rapid diagnosis via multiplex Polymerase Chain Reaction (PCR) on abscess fluid enabled targeted therapy within 24 h, avoiding unnecessary broad-spectrum antibiotics. Intestinal amebiasis should be considered in patients with compatible symptoms and relevant exposure.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
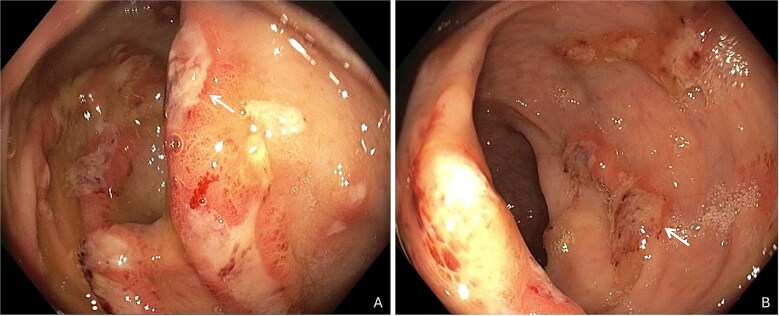 Figure 1
Figure 1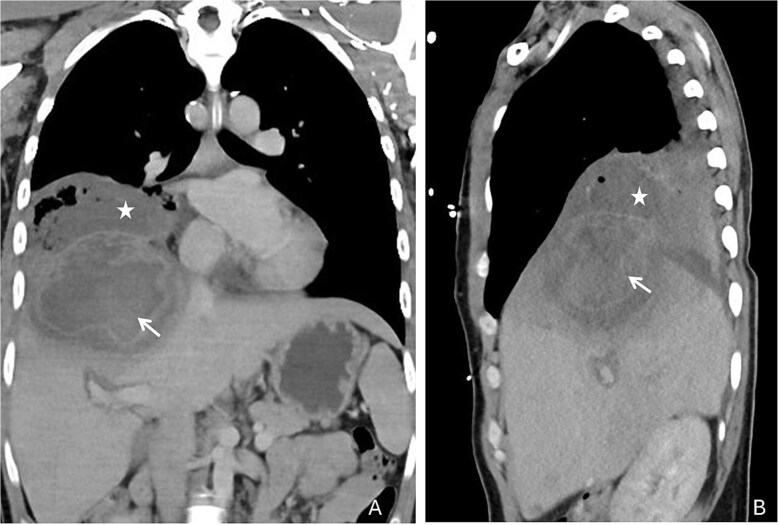 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmoebic Infections and Treatments · Diagnosis and treatment of tuberculosis · Parasites and Host Interactions
Case report
A 30-year-old Swiss male was admitted to the emergency department at the University Hospital of Basel in June 2025 with acute onset of fever, chills and severe hemoptysis.
The patient had no relevant medical history but had returned from rural Cambodia (district of Kampong Chhnang) two months prior to admission, where he worked at a hotel and lived in close contact to locals from November 2024 to April 2025. In January 2025, he experienced acute gastroenteritis with fever, diarrhoea and abdominal cramps which resolved quickly after treatment with ciprofloxacin (500 mg orally twice daily) for 5 days, prescribed by local physicians. Upon return to Switzerland, diarrhoea relapsed with 2–3 watery stools mixed with blood, mild abdominal cramps and 6 kg weight loss, this time without fever. In May 2025, colonoscopy revealed ulcerative lesions of the mucosa (Figure 1), with histological signs of inflammation and preserved glandular architecture. Stool culture for Shigella spp*., Salmonella spp., Campylobacter spp.* and Yersinia spp*.* was negative. A BIOFIRE® FILMARRAY® Gastrointestinal Panel was not performed, and histology slides could not be reviewed retrospectively. Diarrhoea improved spontaneously during the following weeks.
Colonoscopy with ulcerative lesions (white arrows) of the mucosa in the ascending colon (A) and right hepatic flexure (B)
Upon admission to the emergency department, the patient presented with a temperature of 40°C, respiratory distress and hemoptysis. Blood pressure was 140/90 mmHg, heart rate 120/min, respiratory rate 26/min and peripheral oxygen saturation was 91% with 4 litres of supplemental oxygen. Clinical examination revealed abdominal tenderness and decreased breath sounds over the right lung. Laboratory results showed anaemia (98 g/l, reference range 140–180 g/l) elevated leukocytes (14.3 G/l, reference range 3.5–10.0 G/l) with 85% neutrophils, CRP (140 mg/l, reference <10 mg/l), hypoalbuminemia (19 mg/l), normal liver enzymes and bilirubin. A thoracoabdominal computed tomography revealed a large abscess in liver segments VII/VIII (81 × 96 mm) with transdiaphragmatic breakthrough, pleural effusion and pulmonary infiltrates (Figures 2 and 3). Massive hemoptysis required intubation and transfer to the Intensive Care Unit. Empiric intravenous therapy with meropenem (1 g intravenous, three times daily) and metronidazole (10 mg/kg intravenous, three times daily) was initiated, targeting suspected amebiasis and pyogenic liver abscess (covering pathogens like hypervirulent Klebsiella spp*.* and Burkholderia pseudomallei).
Coronal (A) and sagittal (B) reconstructions of the thoracoabdominal computed tomography revealed a peripherally contrast-enhancing collection with perifocal edema in liver segments VII/VIII (white arrows) communicating with the right broncho-pleural space (white stars)
Thoracic computed tomography in axial view revealing dense infiltrates in the right lower lobe (black arrow)
Bronchoscopy showed signs of bronchial inflammation with discrete brownish secretion without haemorrhage. Percutaneous drainage of the liver abscess yielded anchovy-paste–like fluid. A multiplex PCR (BIOFIRE® FILMARRAY® GastrointestinalPanel), validated for stool samples applied to the drainage fluid, tested positive for Entamoeba histolytica with results available within 12 h. Meropenem was discontinued, and metronidazole continued, leading to rapid clinical improvement. Diagnosis of extraintestinal amebiasis with amebic liver abscess and bronchopleural involvement was confirmed by specific PCR for E. histolytica from both liver abscess and bronchial fluid samples, as well as by serology, with results available four days after specimen collection. Clinical follow-up in July 2025 showed complete recovery.
Infection with E. histolytica remains a significant global health burden, increasingly relevant beyond low- and middle-income countries due to international travel.1^,^2
Although rare, amebic liver abscess with thoracic extension is a serious complication, usually caused by diaphragmatic rupture into the pleural space. This can lead to pleuropulmonary manifestations such as empyema, lung abscess or broncho-hepatic fistula, which often require surgical drainage when conservative treatment proves insufficient. With prompt anti-amebic therapy and intervention, the prognosis is favourable.3^,^4
This case highlights the importance of considering intestinal and extraintestinal amebiasis in patients with compatible symptoms and relevant epidemiological exposure. Application of targeted molecular diagnostics enabled early pathogen identification, leading to targeted therapy within 24 h after admission. Here, BIOFIRE® multiplex PCR was successfully applied to abscess fluid, despite being validated only for stool specimen, highlighting the need for further evaluation of this off-label application.5
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shirley DAT, Farr L, Watanabe K, Moonah S. A review of the global burden, new diagnostics, and current therapeutics for Amebiasis. Open forum. Infect Dis 2018;5:ofy 161. 10.1093/ofid/ofy 161.PMC 605552930046644 · doi ↗ · pubmed ↗
- 2Cooney J, Siakavellas SI, Chiodini PL et al. Recent advances in the diagnosis and management of amoebiasis. Front Gastroenterol 2025;16:37–50.10.1136/flgastro-2023-102554 PMC 1296996841809248 · doi ↗ · pubmed ↗
- 3Shamsuzzaman SM, Hashiguchi Y. Thoracic amebiasis. Clin Chest Med 2002;23:479–92.12092041 10.1016/s 0272-5231(01)00008-9 · doi ↗ · pubmed ↗
- 4Ragheb MI, Ramadan AA, Khalil MAH. Intrathoracic presentation of Amebic liver abscess. Ann Thorac Surg 1976;22:483–9.999374 10.1016/s 0003-4975(10)64458-x · doi ↗ · pubmed ↗
- 5Weitzel T, Cabrera J, Rosas R et al. Enteric multiplex PCR panels: a new diagnostic tool for amoebic liver abscess? N Microbes N Infect 2017;18:50–3. 10.1016/j.nmni.2017.05.002.PMC 546074128626584 · doi ↗ · pubmed ↗