Dermoscopic Examination of Generalized Lichen Nitidus in a Patient With Down Syndrome
Karina Okamura, Natsuko Aoki, Tomoko Uemura, Mayuko Yamamoto, Kozo Nakai

TL;DR
This paper describes a case where dermoscopy helped diagnose generalized lichen nitidus in a patient with Down syndrome.
Contribution
The study presents the first description of dermoscopic findings in generalized lichen nitidus in a Down syndrome patient.
Findings
Dermoscopy aided in the accurate clinical diagnosis of generalized lichen nitidus.
This case highlights the potential utility of dermoscopy in diagnosing skin conditions in individuals with Down syndrome.
Patients with Down syndrome are prone to various dermatological conditions, including lichen nitidus.
Abstract
Down syndrome, also known as trisomy 21, is the most frequently identified chromosomal disorder. Patients with Down syndrome frequently present with a broad spectrum of dermatological conditions, including atopic dermatitis, nonspecific dermatitis, folliculitis, seborrheic dermatitis, and cutaneous infections. Several cases of generalized lichen nitidus in individuals with Down syndrome have been reported. However, dermoscopic findings have not been previously described in these cases. We report a case in which dermoscopy contributed significantly to the clinical diagnosis, illustrating its potential role in improving diagnostic accuracy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
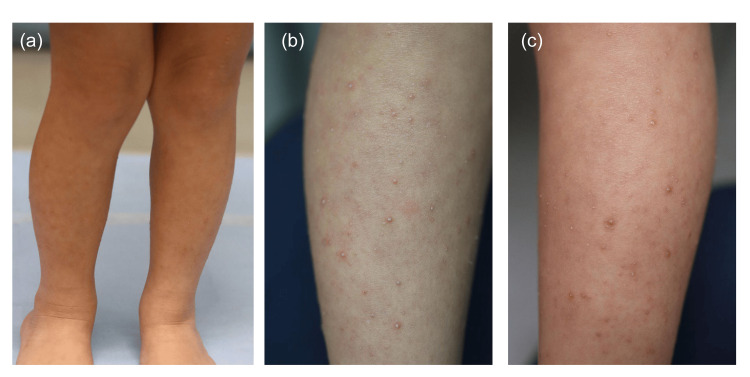 Figure 1
Figure 1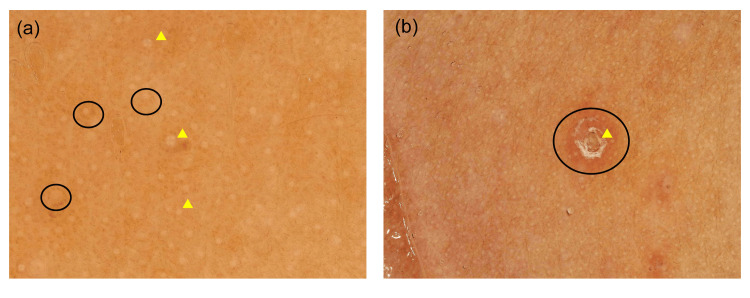 Figure 2
Figure 2| Disease | Dermoscopy |
| Folliculitis | Central follicular pustule or yellow-white structure. |
| Lichen planus | Wickham striae (whitish reticular lines) over a violaceous background with characteristic vascular patterns. The papules are usually larger and polygonal compared with lichen nitidus. |
| Papular eczema (lichenified dermatitis) | Dotted vessels and yellowish scales, usually accompanied by marked pruritus and less uniform papules. |
| Keratosis pilaris | Characterized by follicular keratotic plugs with perifollicular erythema. Coiled hairs and perifollicular scaling. |
| Verruca plana | Dotted or globular vessels on a light brown or yellowish background. |
| Journal | Year | Author | Sex | Age | Distribution | Dermoscopy | Biopsy | |
| Case 1 | Indian J Dermatol Venereol Leprol | 2009 | Agarwal et al. | Female | 4 | Legs, thigh | Not perfomed | Performed |
| Case 2 | An Bras Dermatol | 2012 | Botelho et al. | Female | 4 | Face, trunk, upper and lower limbs, genitalia | Not perfomed | Performed |
| Case 3 | SKINmed | 2019 | Guliani et al. | Male | Preschool | Whole body | Not perfomed | Performed |
| Case 4 | Pediatr Dermatol | 2009 | Henry et al. | Male | 3 | Whole body | Not perfomed | Not perfomed |
| Case 5 | J Eur Acad Dermatol Venereol | 2006 | Laxmisha et al. | Female | 2 | Whole body | Not perfomed | Performed |
| This case | Female | 6 | Upper and lower limbs | Performed | Not perfomed |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral Health Pathology and Treatment · Osteomyelitis and Bone Disorders Research · Cancer Diagnosis and Treatment
Introduction
Down syndrome, also known as trisomy 21, is the most frequently identified chromosomal disorder, occurring globally in approximately one out of every 1,000 live births [1]. Chromosome 21 contains roughly 200-300 genes, and the presence of an extra copy leads to increased gene expression, which may contribute to a wide range of associated medical complications [2,3,4]. Despite receiving relatively limited attention in research and clinical guidelines, dermatologic manifestations can be an important concern in individuals with Down syndrome [5,6]. In one study evaluating health conditions among young adults with Down syndrome, 56% of participants reported having skin-related findings [7], including atopic dermatitis, nonspecific dermatitis, folliculitis, seborrheic dermatitis, and cutaneous infections [8]. These skin manifestations are typically evaluated initially by pediatricians; however, the diagnostic frequencies reported by pediatricians often differ from those identified by dermatologists. This discrepancy suggests that certain dermatological diseases may be underrecognized or misclassified in pediatric practice due to subtle clinical features or limited use of specialized diagnostic tools. Among the conditions that may escape accurate recognition is lichen nitidus, an uncommon, chronic inflammatory dermatosis characterized by discrete, tiny papules. The lesions are usually skin-colored to slightly erythematous, shiny, and dome-shaped, typically measuring 1-2 mm in diameter. They most frequently involve the trunk, genitalia, and flexor aspects of the extremities, but may occasionally become generalized. Most patients are asymptomatic or experience only mild pruritus. Although the exact etiology remains unclear, the disease is generally benign and self-limited, often resolving spontaneously over months to years. Although several cases of generalized lichen nitidus in individuals with Down syndrome have been reported, dermoscopic findings have not been previously described. We report a case in which dermoscopy contributed significantly to the clinical diagnosis, illustrating its potential role in improving diagnostic accuracy.
Case presentation
A six-year-old Japanese girl with Down syndrome was referred to our dermatology department with a persistent and progressively enlarging pruritic eruption that had been present for over one year. Prior to presentation, she had been treated with oral oxatomide and topical diflucortolone under presumed diagnoses of atopic dermatitis or chronic eczema; however, these therapies resulted in no clinical improvement. On examination, numerous (several hundred) reddish-white, flat-topped, partially keratotic papules measuring 1-2 mm in diameter were symmetrically distributed, predominantly on the flexor surfaces of the extremities (Figures 1a-1c).
Clinical presentation of the patient. (a) Reddish-white, flat-topped, partially keratotic papules were observed on the limbs. (b) Magnified view of right leg. (c) Magnified view of left leg.
Dermoscopic evaluation revealed multiple, well-circumscribed, structureless hypopigmentation with brown shadow corresponding to the papules, surrounded by diffuse erythema and subtle red-brown pigmentation. No dotted vessels or scaling suggestive of eczema or folliculitis were observed. These findings are consistent with previously reported dermoscopic patterns of lichen nitidus, which represent focal inflammatory infiltrates under an acanthotic epidermis (Figure 2a-2b).
Dermoscopic examination (a) Numerous hypopigmentation (three representative lesions are indicated with arrowheads) accompanied by diffuse brown pigmentation (three representative lesions are encircled). (b) Papules with crusting (arrowhead) and erythema (encircled).
Although a skin biopsy was recommended to confirm the diagnosis histopathologically, her family declined the procedure. Based on the typical clinical morphology combined with dermoscopic characteristics, a diagnosis of generalized lichen nitidus was made. Continuing topical corticosteroids led to gradual improvement over several months, and no recurrence was observed during follow-up.
Discussion
Patients with Down syndrome frequently present with a broad spectrum of dermatological conditions, including atopic dermatitis, nonspecific dermatitis, folliculitis, seborrheic dermatitis, and cutaneous infections. These cutaneous manifestations are often assessed initially by pediatricians; however, the diagnostic frequencies documented in pediatric practice may differ from those determined by dermatologists. This discrepancy implies that some dermatological disorders may be underrecognized or inaccurately categorized in pediatric settings because of subtle clinical presentations or limited application of specialized diagnostic tools. A recent multi-site retrospective study of 1,529 patients with Down syndrome identified eczematous dermatitis (26%) and folliculitis (19.3%) as the most prevalent dermatological conditions [8]. Although lichen nitidus is generally considered uncommon in the pediatric population, it has been repeatedly reported in association with Down syndrome. A systematic review estimated its prevalence in individuals with Down syndrome to be approximately 1.1%, suggesting that this condition may occur more frequently than in the general population [9]. According to a systematic review that included 40 observational studies and 99 case reports, lichen nitidus has been reported in approximately 1.1% of individuals with Down syndrome to date [10]. Because lichen nitidus can clinically mimic other papular dermatoses, such as follicular eczema or early eczematous eruptions, misdiagnosis may occur in the absence of dermoscopic or histopathological evaluation. Dermoscopy is regarded as a non-invasive and reliable method for evaluating lichen nitidus. According to a study of 20 cases with lichen nitidus, the dermoscopic findings were shiny elevated surface with absence of skin markings (100%), scaling (70%), radial ridges (50%) and central depression (35%), hypopigmentation (100%), brown shadow (70%), linear vessels (65%), accentuation of surrounding reticulate pigment network (65%), diffuse erythema (45%) [11,12]. Such features may be particularly useful when biopsy is impractical due to patient age, clinical circumstances, or caregiver preference. Although a biopsy was not performed in our case, the diagnosis was based on the characteristic clinical presentation and typical dermoscopic findings, which were consistent with previously reported features of lichen nitidus. When diagnosing lichen nitidus based on dermoscopic findings, several papular dermatoses should be considered in the differential diagnosis, including folliculitis, lichen planus, papular eczema, keratosis pilaris, and verruca plana (Table 1).
Importantly, while several cases of generalized lichen nitidus in Down syndrome have been documented, dermoscopic descriptions have not been previously reported, as shown in Table 2.
Our case demonstrates that dermoscopy can provide valuable diagnostic support, especially when biopsy is impractical. This non-invasive strategy may improve diagnostic accuracy.
Conclusions
We describe a case of generalized lichen nitidus in a child with Down syndrome diagnosed using dermoscopy in the absence of histological confirmation. This case highlights the importance of dermoscopic assessment in improving diagnostic precision and underscores its utility as a non-invasive method in clinical scenarios where biopsy cannot be performed. Increased awareness of this entity among pediatricians and dermatologists may facilitate earlier recognition, avoid unnecessary treatments, and contribute to a more accurate epidemiological understanding of dermatological manifestations in patients with Down syndrome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global, regional, and national burden and trends of Down syndrome from 1990 to 2019 Front Genet Chen L Wang L Wang Y Hu H Zhan Y Zeng Z Liu L 9084821320223591021810.3389/fgene.2022.908482 PMC 9337874 · doi ↗ · pubmed ↗
- 2Chromosome 21 and down syndrome: from genomics to pathophysiology Nat Rev Genet Antonarakis SE Lyle R Dermitzakis ET Reymond A Deutsch S 725738520041551016410.1038/nrg 1448 · doi ↗ · pubmed ↗
- 3"Down syndrome: an insight of the disease"J Biomed Sci Asim A Kumar A Muthuswamy S Jain S Agarwal S 412220152606260410.1186/s 12929-015-0138-y PMC 4464633 · doi ↗ · pubmed ↗
- 4Health comorbidities and cognitive abilities across the lifespan in Down syndrome J Neurodev Disord Startin CM D'Souza H Ball G 41220203197369710.1186/s 11689-019-9306-9PMC 6979347 · doi ↗ · pubmed ↗
- 5Health supervision for children with Down syndrome Pediatrics Bull MJ 39340612820112178821410.1542/peds.2011-1605 · doi ↗ · pubmed ↗
- 6Medical care of adults with Down syndrome: a clinical guideline JAMA Tsou AY Bulova P Capone G 1543155632420203307915910.1001/jama.2020.17024 · doi ↗ · pubmed ↗
- 7Health conditions and their impact among adolescents and young adults with Down syndrome P Lo S One Pikora TJ Bourke J Bathgate K Foley KR Lennox N Leonard H 09201410.1371/journal.pone.0096868 PMC 401843624818963 · doi ↗ · pubmed ↗
- 8Dermatologic conditions in Down syndrome: a multi-site retrospective review of International Classification of Diseases codes Pediatr Dermatol Rakasiwi T Ryan C Stein A 104710524120243932764710.1111/pde.15757 · doi ↗ · pubmed ↗