Summary of the best evidence for non-pharmacological interventions for dyslipidemia in patients with coronary heart disease
Zhi Zeng, Xin Zhou, Li Jiang, Yuan Huang, Xiaochun He, Huaili Luo

TL;DR
This study summarizes the best evidence for non-drug treatments to manage high cholesterol in heart disease patients, helping doctors create personalized care plans.
Contribution
A comprehensive synthesis of non-pharmacological evidence for dyslipidemia management in coronary heart disease patients.
Findings
31 studies were included, covering seven evidence themes for non-pharmacological interventions.
Findings support lifestyle changes, TCM, and multidisciplinary approaches for managing dyslipidemia.
The evidence can guide healthcare professionals in developing personalized intervention plans.
Abstract
Retrieve, evaluate, and summarize evidence from domestic and international sources regarding non-pharmacological interventions for dyslipidemia in patients with coronary heart disease (CHD), providing reference for clinical practice. Following the “6S” evidence pyramid model, a systematic search was conducted for literature on non-pharmacological interventions for dyslipidemia in CHD patients, both domestically and internationally, covering the period from January 2014 to December 2025. Two researchers independently screened and evaluated the studies for inclusion, after which the evidence was synthesized. A total of 31 studies were ultimately included, comprising 15 English-language publications and 16 Chinese-language publications. Thirty-one evidence points were summarized, covering seven evidence themes: multidisciplinary team formation, assessment, lipid-lowering targets,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
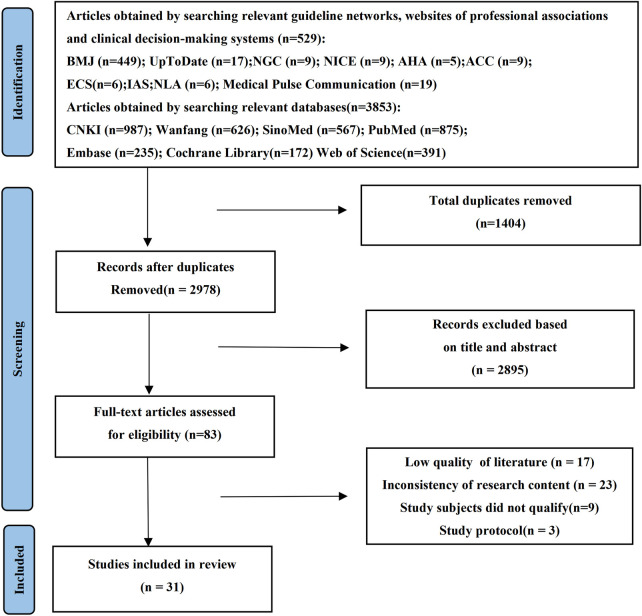 Figure 1
Figure 1| Author(s) | Year of Publication | Study Type | Source | Topic/Focus |
|---|---|---|---|---|
| Mach ( | 2025 | Guideline | PubMed | Management of Dyslipidemia |
| Virani ( | 2023 | Guideline | PubMed | Management of Chronic Coronary Disease |
| Kolber ( | 2023 | Guideline | PubMed | Prevention and Management of Cardiovascular Disease in Primary Care |
| Li ( | 2023 | Guideline | CNKI | Guideline for Blood Lipid Management |
| Yan ( | 2022 | Guideline | CNKI | Clinical Lipid Testing in China |
| Pearson ( | 2021 | Guideline | PubMed | Management of Dyslipidemia for Cardiovascular Disease Prevention in Adults |
| Gu ( | 2020 | Guideline | CNKI | Healthy Lifestyle for the Prevention of Cardiometabolic Diseases |
| Hu ( | 2020 | Guideline | CNKI | Chinese Guideline for Primary Prevention of Cardiovascular Diseases |
| Rhee ( | 2019 | Guideline | PubMed | Management of Dyslipidemia |
| Arnett ( | 2019 | Guideline | PubMed | Guideline on the Primary Prevention of Cardiovascular Disease |
| Gu ( | 2019 | Guideline | CNKI | Risk Assessment and Management of Cardiovascular Diseases |
| Grundy ( | 2018 | Guideline | PubMed | Guideline on the Management of Blood Cholesterol |
| Jellinger ( | 2017 | Guideline | PubMed | Management of Dyslipidemia and Prevention of Cardiovascular Disease |
| Li ( | 2024 | Expert Consensus | CNKI | Blood Lipid Management for Community-Dwelling Adults |
| Liu ( | 2023 | Expert Consensus | Wanfang | Medical Nutrition Therapy for Dyslipidemia |
| Liu ( | 2022 | Expert Consensus | CNKI | Management of Dyslipidemia in the Elderly |
| Wang ( | 2021 | Expert Consensus | Wanfang | Assessment, Detection, and Intervention of Common Risk Factors for Cardiovascular and Cerebrovascular Diseases |
| Hu ( | 2019 | Expert Consensus | Wanfang | Cholesterol Education Program: Lipid-Lowering Therapy to Reduce Cardiovascular Events |
| Sun ( | 2024 | Systematic Review | Pubmed | Efficacy of Acupuncture on Glucose and Lipid Metabolism in Patients with Coronary Heart Disease |
| Cui ( | 2024 | Systematic Review | Pubmed | Effect of Acupuncture-Related Therapies on Blood Lipid Levels in Patients with Coronary Heart Disease |
| Jin ( | 2019 | Systematic Review | Pubmed | Telehealth Interventions for Secondary Prevention of Coronary Heart Disease |
| Yu ( | 2022 | Meta-Analysis | CNKI | Effect of Resistance Exercise on Cardiovascular Risk Factors in Middle-Aged and Older Adults |
| Li ( | 2024 | Meta-Analysis | Wanfang | Effect of Low-Volume High-Intensity Interval Training on Cardiovascular Disease Risk Factors in Individuals with Obesity or Overweight |
| Liu ( | 2021 | Meta-Analysis | CNKI | Efficacy and Safety of Acupuncture Therapy for Hyperlipidemia |
| Zhang ( | 2020 | Meta-Analysis | CNKI | Efficacy and Safety of Traditional Chinese Exercise Therapy for Stable Angina Pectoris in Coronary Heart Disease |
| Xu ( | 2020 | Meta-Analysis | Pubmed | Effect of Green Tea Consumption on Blood Lipids |
| Chen ( | 2017 | Meta-Analysis | Pubmed | Effectiveness of Endurance Exercise Training in Patients with Coronary Artery Disease |
| Wu ( | 2017 | Meta-Analysis | CNKI | Effect of Lifestyle Intervention on Lipid Profiles in Patients with Dyslipidemia |
| Liu ( | 2022 | Randomized Controlled Trial | CNKI | A Randomized Controlled Trial of Acupoint Catgut Embedding Combined with Atorvastatin Calcium for Hyperlipidemia in the Elderly |
| Chen ( | 2019 | Randomized Controlled Trial | Pubmed | Effect of Smoking and Smoking Cessation on High-Density Lipoprotein Function in Coronary Artery Disease |
| Zhang ( | 2017 | Randomized Controlled Trial | Pubmed | Effects of a Nurse-Led Transitional Care Program on Clinical Outcomes, Health-Related Knowledge, and Physical and Mental Health Status in Chinese Patients with Coronary Artery Disease |
| Included literature | Literature sources | Percentage of standardization by domain (100%) | ≥60% of the number of fields ( | ≤30% of the number of fields ( | Recommended level | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Scope and Purpose | Participants | Rigour of formulation | Clarity of presentation | Usefulness of the guide | Editorial independence | |||||
| Mach ( | Pubmed | 83.3 | 66.7 | 81.3 | 83.3 | 79.2 | 91.7 | 6 | 0 | A |
| Virani ( | Pubmed | 100.0 | 88.9 | 87.8 | 97.2 | 37.5 | 95.8 | 6 | 0 | A |
| Kolber ( | Pubmed | 95.9 | 90.3 | 88.4 | 98.6 | 85.7 | 95.5 | 6 | 0 | A |
| Li ( | CNKI | 77.8 | 61.1 | 66.7 | 66.7 | 62.5 | 58.3 | 5 | 0 | A |
| Yan ( | CNIK | 88.9 | 61.1 | 75.0 | 83.3 | 70.8 | 91.7 | 6 | 0 | A |
| Pearson ( | Pubmed | 83.3 | 61.1 | 81.3 | 77.8 | 75.0 | 91.7 | 6 | 0 | A |
| Gu ( | CNKI | 94.4 | 55.6 | 72.9 | 83.3 | 66.7 | 91.7 | 5 | 0 | A |
| Hu ( | CNKI | 88.9 | 55.6 | 85.4 | 100 | 79.2 | 91.7 | 5 | 0 | A |
| Rhee ( | Pubmed | 88.9 | 77.8 | 83.3 | 94.4 | 83.3 | 58.3 | 5 | 0 | A |
| Arnett ( | Pubmed | 95.4 | 88.7 | 98.5 | 90.3 | 82.8 | 90.5 | 6 | 0 | A |
| Gu ( | CNKI | 88.9 | 77.8 | 79.2 | 88.9 | 75.0 | 83.3 | 6 | 0 | A |
| Grundy ( | Pubmed | 95.4 | 90.7 | 98.2 | 92.6 | 85.6 | 88.3 | 6 | 0 | A |
| Jellinger ( | Pubmed | 90.5 | 85.6 | 88.9 | 92.4 | 80.7 | 85.8 | 6 | 0 | A |
| Criterion | Li ( | Liu ( | Liu ( | Wang ( | Hu ( |
|---|---|---|---|---|---|
| Are the sources of viewpoints clearly indicated? | + | + | + | + | + |
| Do the viewpoints originate from influential experts in the field? | + | + | + | + | + |
| Are the proposed viewpoints centered on the interests of the relevant study population? | + | + | + | + | + |
| Are the stated conclusions based on the results of analysis? | + | + | + | + | + |
| Is existing literature referenced? | + | + | + | + | + |
| Are there inconsistencies between the proposed viewpoints and previous literature? | ? | + | ? | + | ? |
| Criterion | Sun ( | Cui ( | Jin ( | Yu ( | Li ( | Liu ( | Zhang ( | Xu ( | Chen ( | Wu ( |
|---|---|---|---|---|---|---|---|---|---|---|
| Whether the evidence-based questions raised are clear and unambiguous | + | + | + | + | + | + | + | + | + | + |
| Whether the inclusion criteria were appropriate for this evidence-based question | + | + | + | + | + | + | + | + | + | + |
| Whether the search strategy is appropriate | + | + | + | + | + | + | + | + | + | + |
| Whether the database or resources for searching the literature are adequate | + | + | + | + | + | + | + | + | + | + |
| Whether the literature quality evaluation criteria used are appropriate | + | + | + | + | + | + | + | + | + | + |
| whether two or more reviewers independently completed the literature quality evaluation | + | + | + | + | + | ? | + | + | ? | ? |
| Whether certain measures were taken to reduce errors when extracting data | ? | ? | + | ? | + | ? | ? | ? | ? | ? |
| whether the method of pooling studies is appropriate | + | + | + | + | + | + | + | + | + | + |
| Whether the likelihood of publication bias was assessed | + | + | + | + | + | + | + | + | + | + |
| Whether the recommendations for policy or practice are based on the results of a systematic review | + | + | + | + | + | + | + | + | + | + |
| whether the proposed further research direction is appropriate | + | + | + | + | + | + | + | + | + | + |
| Criterion | Liu ( | Chen ( | Zhang ( |
|---|---|---|---|
| Randomization process | + | + | + |
| Deviations from intended interventions | − | + | + |
| Missing outcome data | + | + | + |
| Measurement of the outcome | + | + | + |
| Selection of the reported result | + | + | + |
| Evidence Theme | Evidence Content | Level of Evidence | Strength of Recommendation |
|---|---|---|---|
| 1. Establishing a Multidisciplinary Team | 1. A multidisciplinary team including nutrition professionals should be established to collaboratively manage lipid levels in patients with coronary heart disease ( | Level 5 | A |
| 2. Assessment | 2. Conduct a comprehensive cardiovascular risk assessment for patients with coronary heart disease as the basis for decision-making on lipid intervention. Develop individualized lipid intervention strategies according to the level of risk ( | Level 1 | A |
| 3. Low-density lipoprotein cholesterol (LDL-C) is recommended as the primary target. For patients with concurrent diabetes, metabolic syndrome, obesity, or high triglycerides, non-HDL-C should be used as the primary target instead ( | Level 1 | A | |
| 3. Lipid-Lowering Targets | 4. LDL-C is the primary target, with the following goals ( | Level 2 | B |
| 4. Lifestyle Modification | |||
| 4.1 Dietary Management | 5. Control total caloric intake while meeting daily essential nutritional needs, and appropriately select the proportion of various nutritional components ( | Level 2 | A |
| 6. Increase intake of fresh fruits and vegetables, whole grains, dietary fiber, and healthy proteins (low-fat dairy, legumes, skinless poultry, fish/seafood, nuts) ( | Level 1 | A | |
| 7. Limit total daily fat intake to 20−25 g, replace saturated fatty acids (animal fat, palm oil, etc.) with unsaturated fatty acids (fish, rapeseed oil, olive oil, etc.), and avoid trans fatty acids (hydrogenated vegetable oils, etc.) ( | Level 2 | A | |
| 8. Limit dietary cholesterol intake (<300 mg/day) ( | Level 2 | A | |
| 9. Limit intake of processed foods, red meat, sugar-sweetened beverages, and refined carbohydrates ( | Level 1 | A | |
| 10. Limit alcohol intake (men ≤25 g/d, women ≤15 g/d) ( | Level 1 | A | |
| 11. Long-term tea consumption helps lower blood lipids. Moderate consumption of green tea is recommended, with a monthly tea leaf consumption of 50−250 g. However, strong tea is not advised, and tea should not replace all drinking water ( | Level 5 | A | |
| 12. Intake of plant sterols, fish oil, and red yeast rice may help lower blood lipid levels ( | Level 5 | B | |
| 4.2 Exercise Management | 13. Moderate physical activity is beneficial for regulating lipid levels. Diversified exercise is recommended, and participation in group activities is encouraged ( | Level 1 | A |
| 14. Patients with coronary heart disease are recommended to perform aerobic exercise 3–4 times per week, for 40 min each session, at moderate to vigorous intensity ( | Level 1 | A | |
| 15. Examples of moderate-intensity aerobic exercise: walking, dancing, household chores, yoga, and Tai Chi. Examples of high-intensity aerobic exercise: brisk walking or running, jumping rope, swimming, basketball, soccer, hiking with load, etc. ( | Level 1 | A | |
| 16. A combination of the two intensities is permissible. Conversion: 1 min of high-intensity aerobic activity is equivalent to 2 min of moderate-intensity aerobic activity ( | Level 2 | B | |
| 17. Elderly patients who cannot meet exercise targets should still be as physically active as their condition allows and avoid sedentary behavior ( | Level 3 | B | |
| 4.3 Tobacco Management | 18. Avoid all forms of tobacco consumption and avoid exposure to secondhand smoke ( | Level 1 | A |
| 19. Emphasize the importance of smoking cessation repeatedly to smokers and assist them in quitting. However, electronic cigarettes are not recommended as first-line smoking cessation therapy ( | Level 1 | A | |
| 4.4 Weight Management | 20. Maintain a BMI of 20–25 kg/m2, with waist circumference <94 cm (men) and <80 cm (women), to reduce obesity and insulin resistance ( | Level 1 | A |
| 21. Adjust diet based on individual calorie needs, food preferences, and medical conditions to avoid weight gain. Overweight and obese individuals should limit staple food intake and control total calories ( | Level 3 | B | |
| 22. Even for individuals who are not overweight, at least 30 min of moderate-intensity physical activity per day is recommended ( | Level 1 | A | |
| 23. Assist overweight/obese patients with coronary heart disease to lose weight in order to reduce cholesterol levels. Pharmacological or surgical intervention may be considered if necessary ( | Level 1 | A | |
| 4.5 Sleep and Psychological Management | 24. Maintain high-quality sleep for 6–8 h, avoiding excessively short or long sleep duration ( | Level 1 | A |
| 25. Mental stress can increase serum free fatty acids, which is detrimental to lipid control. It can be managed through psychotherapy, meditation, yoga, etc. ( | Level 1 | A | |
| 26. Patients with coronary heart disease who have psychological disorders such as depression, anxiety, or sleep disorders are advised to seek active treatment ( | Level 1 | A | |
| 5. Non-Pharmacological Interventions in Traditional Chinese Medicine (TCM) | 27. Acupuncture therapy ( | Level 1 | A |
| 28. TCM exercise therapies such as Tai Chi and Baduanjin also aid in lipid control ( | Level 1 | A | |
| 6. Health Education | 29. Disseminate knowledge about coronary heart disease and lipid control, emphasize the importance of adhering to a healthy lifestyle, and support patients in making beneficial behavioral changes ( | Level 1 | A |
| 7. Follow-up Management | 30. Regular lipid testing is crucial for lipid management. For patients on non-pharmacological therapy, lipid levels should be rechecked within the initial 3–6 months. If targets are met, continue non-pharmacological therapy with follow-up tests every 6–12 months. For those consistently meeting targets long-term, annual testing is sufficient ( | Level 1 | A |
| 31. Provide regular follow-up guidance to patients with coronary heart disease. Follow-up methods include home visits, telephone calls, and telehealth ( | Level 1 | A |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLipoproteins and Cardiovascular Health · Diabetes, Cardiovascular Risks, and Lipoproteins · Health Promotion and Cardiovascular Prevention
Introduction
1
Coronary heart disease (CHD) is a cardiac condition caused by atherosclerosis of the coronary arteries, leading to narrowing, spasm, or even occlusion of the vessel lumen, which in turn triggers myocardial ischemia, hypoxia, or necrosis (1). It is characterized by high morbidity and mortality rates (2). Research indicates that in developed countries, effective control of risk factors and rational allocation of medical resources have led to a declining trend in CHD prevalence. Conversely, in developing nations, accelerated urbanization and lifestyle changes have driven a rapid increase in its prevalence (3). As a developing nation, China follows the global trend among similar countries, with CHD affecting 11.39 million individuals (4), imposing significant economic burdens on patients’ families and healthcare institutions (5). With an aging population, its incidence and mortality rates are projected to continue rising (6). Dyslipidemia is a major risk factor for CHD recurrence and mortality and is primarily manifested as elevated serum levels of total cholesterol, low-density lipoprotein cholesterol (LDL-C), and triglycerides, coupled with reduced levels of high-density lipoprotein cholesterol (HDL-C) (7, 8). Multiple studies (9–11) demonstrate that effective lipid-lowering therapy not only significantly reduces LDL-C levels in CHD patients but also improves their cardiovascular health outcomes. Currently, guidelines and expert consensus documents on lipid management for CHD patients are increasingly abundant, providing critical references for clinical practice. However, most of this evidence focuses on pharmacotherapy (12–14), and in real-world application, suboptimal patient adherence and insufficient treatment intensity often lead to poor rates of lipid control (15–17). Therefore, actively exploring non-pharmacological interventions to manage lipid levels in CHD patients has become an urgent research priority (18, 19).
Non-pharmacological interventions primarily lower lipid levels through weight control, regular exercise, and smoking cessation (20). Relevant guidelines particularly emphasize (21) that comprehensive non-pharmacological interventions should be highly prioritized and recommended in the management of dyslipidemia in patients with CHD to optimize treatment outcomes. However, evidence regarding non-pharmacological interventions for individuals with both CHD and dyslipidemia remains fragmented and lacks systematic, standardized evidence-based guidance, which severely hinders the translation of evidence into clinical practice. Although existing guidelines on lipid management provide a theoretical basis for non-pharmacological interventions, their practical application presents the following limitations: (1) They are mostly confined to macro-level descriptions of basic principles and elements, lacking specific lifestyle intervention measures; moreover, intervention protocols in original studies vary widely, with no unified guidance standards. (2) While they offer detailed descriptions of intervention content and outcomes, the applicability of their recommendations is limited by cultural differences and regional variations in disease profiles. (3) Current evidence lacks systematic synthesis and standardized guidance, making it difficult to meet the urgent needs of clinical practice. Summarizing best evidence is a crucial component of evidence-based nursing, as it synthesizes the highest-quality and most relevant research findings to provide clear and actionable insights for clinical decision-making (22). Therefore, this study aims to conduct a graded retrieval and synthesis of evidence based on the “6S” pyramid evidence resource model (23). In this model, each “S” represents a type of evidence, categorized hierarchically into six levels from the highest to the lowest: computerized decision support systems, evidence-based synopses of topics, synopses of systematic reviews, systematic reviews, synopses of original studies, and original studies. By rigorously evaluating and systematically integrating evidence on non-pharmacological interventions for CHD patients with dyslipidemia according to this model, this study seeks to provide a reference for developing scientific, precise, and efficient clinical intervention protocols.
Materials and methods
2
Research design
2.1
This study adopted a best-evidence summary design. This methodology aims to address specific clinical questions that require urgent evidence-based answers by systematically retrieving and critically appraising existing evidence resources, such as guidelines and systematic reviews, in order to provide efficient and reliable support for rapid decision-making. It differs in both objectives and scope from systematic reviews, which focus on quantitative synthesis of original research, and from scoping reviews, which aim to map the scope and characteristics of an evidence field. To ensure rigor and transparency, the design and reporting of this study strictly followed the PRISMA-ScR guidelines. Although these guidelines are primarily intended for scoping reviews, their core requirements for systematic searching, screening, data extraction, and reporting transparency align closely with the objective of this study: to comprehensively and transparently summarize and present high-quality evidence. The study protocol was registered with the Center for Evidence-Based Nursing at Fudan University (Registration Number: ES20246942). This study is a secondary analysis of the existing literature and is considered exempt from ethical review.
Establishment of problems
2.2
Evidence-based questions were constructed following the PIPOST model proposed by the Evidence-Based Nursing Center of Fudan University (24): (1) Population (P): patients with coronary atherosclerotic heart disease; (2) Intervention (I): non-pharmacological interventions aimed at controlling dyslipidemia in patients with coronary heart disease; (3) Evidence users (P): healthcare professionals, patients, and their families; (4) Outcomes (O): lipid-monitoring indicator measurements; (5) Settings (S): hospitals, communities, and households; (6) Types of evidence (T): clinical decisions, best practices, clinical guidelines, systematic reviews, evidence summaries, expert consensus documents, and relevant original studies.
Literature search strategy
2.3
Following the top-down retrieval principle of the “6S” evidence model (23), we searched the following evidence-based resources using a combination of subject headings and free-text terms: (1) Clinical decision support systems: BMJ Best Practice and UpToDate; (2) Guideline websites: the Guidelines International Network (GIN), the National Institute for Health and Care Excellence (NICE), the Scottish Intercollegiate Guidelines Network (SIGN), the New Zealand Guidelines Group (NZGG), the National Guideline Clearinghouse (NGC), and Medlive; (3) Professional association websites: the American Heart Association (AHA), the American College of Cardiology (ACC), the European Society of Cardiology (ESC), the International Atherosclerosis Society (IAS), and the National Lipid Association (NLA); (4) Comprehensive databases: China National Knowledge Infrastructure (CNKI), Wanfang Data, China Biology Medicine disc (CBM), PubMed, Web of Science, CINAHL, and Embase. The search period was set from January 2014 to December 2025. Search terms encompassed: Coronary Disease, Coronary Heart Disease, Coronary Atherosclerotic Heart Disease, Ischemic Heart Disease, Myocardial Ischemia, Acute Coronary Syndrome, Myocardial Infarction, Angina Pectoris; Lipids, Cholesterol, Hyperlipidemias, Dyslipidemias, Hypercholesterolemia, Lipidosis, Blood Lipid Management, and Blood Fat Management. The detailed search strategy is provided in Supplementary Material 1.
Literature inclusion and exclusion criteria
2.4
Inclusion Criteria: (1) Patients aged ≥18 years with a diagnosis of coronary heart disease and comorbid dyslipidemia; (2) Interventions involving any structured non-pharmacological strategy (e.g., exercise training, dietary modification, comprehensive lifestyle intervention, or patient education) aimed at improving lipid profiles; (3) Reported outcomes including absolute values or changes in key lipid parameters (e.g., LDL-C, TC, TG, HDL-C); (4) Publication types: clinical guidelines, expert consensus statements, systematic reviews, meta-analyses, evidence summaries, randomized controlled trials, non-randomized controlled trials, or prospective cohort studies; (5) Publications in Chinese or English. Exclusion Criteria: (1) Literature for which the full text is unavailable; (2) Literature deemed to be of low methodological quality (for example, RCTs with an overall high risk of bias per Cochrane RoB tool); (3) Duplicate publications.
Literature quality evaluation
2.5
Four researchers independently assessed the included guidelines, while two other researchers independently evaluated the quality of expert consensus documents, standards, and systematic reviews. Discrepancies were resolved through discussion or by consultation with a third researcher. All four researchers had received systematic training in evidence-based methods. The criteria for assessing the quality of the literature were as follows: (1) Clinical Decision Support Tools: As the highest-level resources in evidence-based practice, they are authoritative and comprehensive. Evidence directly relevant to the study topic from clinical decision support tools or evidence summaries was included. (2) Guidelines: Evaluated using the Appraisal of Guidelines for Research and Evaluation (AGREE) II tool (25), which consists of 23 items across 6 domains and 2 global rating items. Each item is scored on a scale from 1 to 7 points. The standardized percentage for each domain was calculated as: (Actual Score − Minimum Possible Score)/(Maximum Possible Score − Minimum Possible Score) × 100%. The recommendation levels were categorized into: Grade A (strongly recommended, with standardized scores ≥60% in all 6 domains), Grade B (recommended, with ≥3 domains scoring ≥30% and <60%), and Grade C (not recommended, with ≥3 domains scoring <30%). Guidelines rated as Grade C were excluded. (3) Expert Consensus: Evaluated using the expert consensus evaluation criteria of the Australian JBI Evidence-Based Health Care Center (2016) (26), which includes 6 assessment items. Each assessor independently selected one of the following responses: “Yes,” “No,” “Unclear,” or “Not applicable.” (4) Systematic Reviews and Meta-Analyses: Methodological quality was assessed using the Assessment of Multiple Systematic Reviews (AMSTAR) tool (27). This instrument consists of 11 items: Was an a priori design provided? Was there duplicate study selection and data extraction? Was a comprehensive literature search performed? Was the publication status (e.g., grey literature) used as an inclusion criterion to minimize publication bias? Was a list of included and excluded studies provided? Were the characteristics of the included studies (e.g., design, sample size, outcomes) provided? Was the scientific quality of the included studies assessed and documented appropriately? Was the scientific quality of the included studies used appropriately in formulating conclusions? Were appropriate methods used to combine the findings of studies? Was the likelihood of publication bias assessed? Was any potential conflict of interest stated? For each item, two independent assessors selected one of the following responses: “Yes,” “No,” “Unclear,” or “Not Applicable.” (5) Randomized Controlled Trials: The risk of bias was evaluated using the Cochrane Risk of Bias tool for randomized trials, version 2 (RoB 2) (28). The assessment covered seven specific domains: randomization process; deviations from intended interventions; missing outcome data; measurement of the outcome; and selection of the reported result. For each domain, two independent assessors made a judgment of “Low risk,” “High risk,” or “Unclear risk.”
Summary, classification, and recommendation level of evidence
2.6
Two researchers independently extracted evidence, collecting information including publication date, study type, source of evidence, topic of evidence, and specific content. All researchers were involved in the translation, extraction, and synthesis of evidence. The principles for evidence synthesis were as follows (29): (1) When evidence contents were consistent, concise, clear, and professional evidence was prioritized. (2) When evidence contents complemented each other, they were merged into logically structured statements. (3) When evidence contents differed, priority was given based on evidence-based, high-quality, authoritative, and recently published evidence. In this study, evidence was graded using the Australian JBI Centre for Evidence-Based Health Care Evidence Grading and Recommendation System (2014 version), which classifies evidence into levels 1 to 5. Subsequently, two evidence-based nursing experts and three cardiovascular field experts were invited to determine the recommendation level (Grade A: strong recommendation or Grade B: weak recommendation) for each piece of evidence based on the principles of validity, feasibility, appropriateness, and clinical significance (30, 31).
Results
3
Literature search results
3.1
A total of 5,212 records were identified through the initial literature search. After screening, a total of 31 studies were ultimately included, comprising 15 English-language publications and 16 Chinese-language publications. The study selection process is presented in Figure 1. The basic characteristics of the included studies are summarized in Table 1.
PRISMA flowchart.
Quality evaluation results of the included literature
3.2
Quality evaluation results of the guideline
3.2.1
This study included a total of 9 guidelines. The standardized scores and evaluation results for each guideline domain are presented in Table 2.
Quality evaluation results of the expert consensus
3.2.2
This study included a total of 5 expert consensus documents. The results of the quality assessment are presented in Table 3.
Quality assessment results of systematic reviews and meta-analyses
3.2.3
This study included 3 systematic reviews and 7 meta-analyses. The quality assessment results are presented in Table 4.
Quality evaluation results of randomized controlled trials
3.2.4
This study included a total of 3 randomized controlled trials. The results of the quality assessment are presented in Table 5.
Evidence description and summary
3.3
Based on the principle of evidence synthesis, researchers summarized the evidence. A total of 31 pieces of evidence were summarized, covering seven evidence themes: establishment of a multidisciplinary team, assessment, lipid-lowering targets, lifestyle modification, traditional Chinese medicine non-pharmacological interventions, health education, and follow-up management as shown in Table 6.
Discussion
4
Setting lipid management targets based on cardiovascular risk levels is scientifically sound
4.1
Evidence summaries 1–3 outline the assessment and lipid-lowering targets for patients with CHD. These targets are closely related to the patient's cardiovascular risk level, with stricter LDL-C control goals required for individuals at higher risk (7). This indicates that applying “normal” reference ranges intended for the general population to CHD patients may fail to achieve adequate risk control. Therefore, clinical practice recommends setting lipid-lowering targets according to the patient's specific risk level. Moreover, since the primary goal of lipid management is the prevention and treatment of CHD, and given the pivotal role of LDL-C in the development of atherosclerosis and the progression of CHD (63), current evidence (39) recommends LDL-C as the primary intervention target in lipid testing—a view widely accepted in clinical practice (64). However, it should be noted that individual responses to lipid-lowering therapy vary. Thus, when establishing lipid-lowering goals, the patient's actual clinical situation should be taken into account to ensure both scientific soundness and clinical feasibility. Evidence summary 4 suggests that lipid management for CHD patients requires multidisciplinary collaboration. In the future, healthcare professionals may refer to this evidence summary to form multidisciplinary management teams that include nutrition, nursing, cardiology, and other relevant disciplines (65). By developing scientific, standardized, and individualized lipid management protocols for CHD, along with comprehensive implementation strategies, the effective integration of lipid management into clinical practice can be promoted.
Strengthen non-pharmacological interventions for patients and promote the adoption of a healthy lifestyle
4.2
Evidence Recommendations 5–26 suggest that patients with coronary heart disease can achieve a healthy lifestyle transformation through measures such as dietary control, regular exercise, and smoking cessation, thereby improving lipid management outcomes. Existing literature indicates that a reasonable diet and sustained regular exercise can improve body composition, enhance immunity, and prevent or delay disease progression (66, 67). These practices also exert positive effects on the physical and mental health as well as the quality of life of patients with coronary heart disease (68, 69). The recommendations presented in this study integrate multiple guidelines and are largely consistent with the healthy lifestyles currently advocated (70, 71). However, in real-world clinical practice, to ensure long-term patient benefit, the development of specific plans should fully take into account patient preferences, physical condition, and resource availability. Whenever feasible, dietary and exercise guidance should be provided under supervision to enhance patient adherence and long-term persistence. It is worth noting that the currently recommended dietary patterns are primarily the DASH (Dietary Approaches to Stop Hypertension) diet (in the United States) and the Mediterranean diet (in Europe) (72), which may differ from the traditional dietary habits of populations in various countries. Therefore, future work should actively explore lipid-management dietary patterns that align with local patient preferences and eating habits, and should further evaluate the effectiveness of each dietary model. Evidence Recommendations 27–28 summarize non-pharmacological interventions in Traditional Chinese Medicine (TCM). Modalities such as acupuncture and acupoint catgut embedding, as traditional Chinese non-pharmacological therapies, not only offer advantages including demonstrated efficacy, few adverse reactions, and low cost, but also align well with China's national context and patients’ healthcare practices (73). However, owing to differences in ethnicity, healthcare systems, and cultural backgrounds, the effectiveness and applicability of these non-pharmacological interventions in other countries remain uncertain and require further validation through subsequent research.
Strengthen health education and follow-up management to improve lipid management outcomes
4.3
Evidence-based recommendation No. 29 advocates implementing lipid management-related health education for patients with CHD. Previous studies have shown (74) that the treatment rate and control attainment rate for dyslipidemia among CHD patients are 14.1% and 26.6%, respectively. This indicates that improving patients’ knowledge of lipid management and treatment adherence can help enhance the achievement of lipid control targets (75). Regarding implementation approaches, on one hand, the importance of lipid management should be communicated to patients and their families through methods such as distributing educational brochures, sharing instructional videos, and organizing health lectures (76). This helps increase adherence to lipid-lowering therapy, thereby improving lipid management outcomes (77). On the other hand, information technology can be utilized to establish “Internet+” health education platforms, which overcome the temporal and spatial limitations of traditional health education and allow patients and their families to access lipid management-related health education resources anytime and anywhere (78, 79). Evidence summaries No. 30–31 compile the recommended frequency and methods of follow-up. Continuously monitoring lipid levels in CHD patients aids in preventing and managing CHD and reduces the risk of disease recurrence (80). These recommendations define lipid monitoring intervals based on patients’ lipid control attainment rates. However, in clinical practice, it is also advisable to comprehensively consider patients’ lipid levels, treatment regimens, and medication responses to develop more personalized lipid monitoring plans for CHD patients. Regarding follow-up methods, in addition to traditional models such as telephone calls, text messages, and home visits, internet-based follow-up models not only significantly improve patients’ knowledge awareness, health behaviors, and quality of life but also effectively reduce the workload of healthcare professionals (81). Therefore, it is recommended to further investigate internet-based follow-up models in the future, continue to integrate and standardize the informatized follow-up management platform for CHD patients, and build an informatized follow-up platform that enables real-time information sharing and full-process coverage management, thereby advancing traditional follow-up models toward greater informatization.
Limitations
4.4
This evidence summary comprehensively focuses on evidence regarding the non-pharmacological management of dyslipidemia in patients with coronary heart disease. It aims to assist healthcare practitioners in efficiently accessing and understanding the evidence, improving lipid control in patients with coronary heart disease, and enhancing their cardiovascular health outcomes. However, our review has several limitations. First, since the literature search was restricted to publications in Chinese and English, studies in other languages were not included, which may introduce language bias. Second, the diversity of patient populations, cancer types, and clinical practices across different healthcare settings may affect the generalizability of our recommendations. Finally, certain innovative non-pharmacological intervention strategies might not have been incorporated into our evidence-based recommendations because their scientific validity, generalizability, and precise effectiveness have not yet been fully established. This limitation highlights the necessity for continued research and evaluation to support these emerging approaches.
Summary
5
This study synthesizes evidence from 31 non-pharmacological interventions for dyslipidemia in patients with coronary heart disease, providing valuable resources for clinical practitioners. The findings presented herein are based on existing research conclusions. However, individual patient circumstances may vary, necessitating personalized lipid management strategies tailored to specific clinical situations. When integrating this evidence into clinical practice, healthcare professionals should leverage their expertise, consider unique clinical contexts, and make informed decisions grounded in the best available evidence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kim YJ Malhi J Trost J Leucker T Virani SS Newby LK A case-based approach to the management of patients with chronic coronary disease: updates from the 2023 AHA/ACC guidelines. Am J Med. (2025) 138(2):204–8. 10.1016/j.amjmed.2024.09.01339284478 · doi ↗ · pubmed ↗
- 2Al-Lamee RK. Angina pectoris 2023: with and without obstructive coronary artery disease: epidemiology, diagnosis, prognosis, and treatment. Vasc Pharmacol. (2024) 155:107285. 10.1016/j.vph.2024.10728538431201 · doi ↗ · pubmed ↗
- 3Zhu KF Wang YM Zhu JZ Zhou QY Wang NF. National prevalence of coronary heart disease and its relationship with human development index: a systematic review. Eur J Prev Cardiol. (2016) 23(5):530–43. 10.1177/204748731558740225976715 · doi ↗ · pubmed ↗
- 4Lan Y Luo FK Yu Y Wang XY Wang PQ Xiong XJ. Coronary heart disease: innovative understanding from traditional Chinese medicine and treatment by classic formulas. Zhongguo Zhongyao Zazhi/China J Chin Mater Med. (2024) 49(13):3684–92. 10.19540/j.cnki.cjcmm.20240326.50139041141 · doi ↗ · pubmed ↗
- 5Mi Y Xue Z Qu S Yin Y Huang J Kou R The economic burden of coronary heart disease in mainland China. Public Health. (2023) 224:140–51. 10.1016/j.puhe.2023.08.03437797560 · doi ↗ · pubmed ↗
- 6Li Q Zhang H Xiao N Liang G Lin Y Yang X Aging and lifestyle modifications for preventing aging-related diseases. FASEB J. (2025) 39(9):e 70575. 10.1096/fj.202402797 RR 40293686 · doi ↗ · pubmed ↗
- 7Brunham LR Lonn E Mehta SR. Dyslipidemia and the current state of cardiovascular disease: epidemiology, risk factors, and effect of lipid lowering. Can J Cardiol. (2024) 40(8S):S 4–S 12. 10.1016/j.cjca.2024.04.01739111899 · doi ↗ · pubmed ↗
- 8Pirillo A Casula M Olmastroni E Norata GD Catapano AL. Global epidemiology of dyslipidaemias. Nat Rev Cardiol. (2021) 18(10):689–700. 10.1038/s 41569-021-00541-433833450 · doi ↗ · pubmed ↗