Unveiling the role of interleukin-13 in liver fibrosis of chronic hepatitis B patients: Development of a predictive model
Muhammad Begawan Bestari, Muhammad Palar Wijaya, Dolvy Girawan, Nenny Agustanti, Eka Surya Nugraha, Xiaosheng Tan, Xiaosheng Tan, Xiaosheng Tan, Xiaosheng Tan

TL;DR
This study explores how interleukin-13 affects liver stiffness in chronic hepatitis B patients and creates a model to predict it.
Contribution
The novel contribution is a predictive model for liver stiffness in CHB patients that includes interleukin-13 alongside age and platelet count.
Findings
A predictive model with R2 of 0.37 was developed using age, platelet count, and IL-13 levels.
Elevated IL-13 and lower platelet count are associated with increased liver stiffness.
The model met statistical criteria for reliability and normal distribution.
Abstract
Developing a non-invasive model is essential for assessing liver stiffness in conditions without transient elastography, which will determine further management in chronic hepatitis B (CHB) patients. This study aims to evaluate the interleukin-13 role in liver fibrosis and develop a new predictive model that includes interleukin-13 and standard data such as age and platelet count. Patients were recruited from Hasan Sadikin General Hospital’s CHB registry from October 2021 to January 2022. Patients underwent demographic data collection, complete blood count, interleukin-13, and transient elastography examinations on the same day. The platelet count variable was listed in ×109/ dL, and the interleukin-13 in pg/mL. Interleukin-13 values were categorized as positive for IL-13 with a cut-off of 5 pg/mL (ILcut5). The liver stiffness measurement was inverted to obtain a normal distribution…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2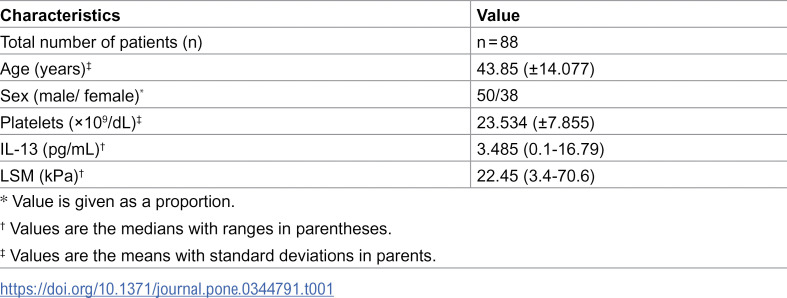 Figure 3
Figure 3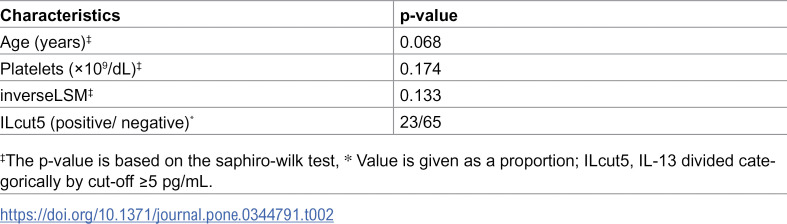 Figure 4
Figure 4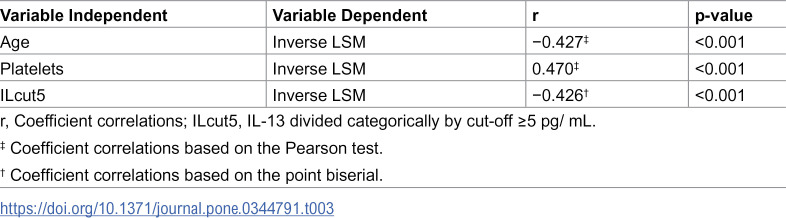 Figure 5
Figure 5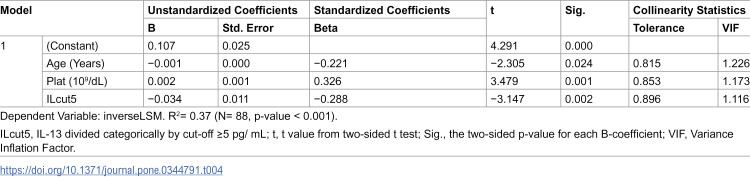 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease Diagnosis and Treatment · Inflammatory Biomarkers in Disease Prognosis · Liver Disease and Transplantation
Introduction
Chronic hepatitis B (CHB) occurs when hepatitis B surface antigen (HBsAg) is present in blood serum for over six months. Age of exposure is crucial for determining the risk of developing a chronic infection. [1] People who are HBsAg-positive need to be checked regularly to monitor indications for treatment. [2] Some necessary things that need attention include levels of Hepatitis B Envelope Antigen (HBeAg), aminotransferase, Hepatitis B Virus (HBV) DNA, and the importance of assessing the stage of liver fibrosis through several non-invasive tests (NITs). [1] CHB treatment is recommended for people with evidence of significant fibrosis/ cirrhosis, and it is explicitly stated to assess it through the aspartate aminotransferase (AST) to Platelet Ratio Index (APRI) score or transient elastography (TE) value. TE services require trained skills and significant effort in procuring the equipment [1].
Through multivariate analysis of various primary patient data, prediction models were created to find the best model for determining the significance of liver fibrosis. [3,4] A systematic multivariate analysis formed a simple model involving platelet count and AST levels. [3] After a multivariate analysis, platelets, age, AST, and alanine aminotransferase (ALT) formed a Fibrosis-4 Index (FIB-4) model to predict liver fibrosis [4].
The patient’s age is the primary personal data that is always considered in the differential diagnosis of a disease. The likelihood of developing chronic liver disease (CLD) rises with age. Apart from that, old age is the main factor for complications and puts patients in dangerous conditions. [5] Platelet count is an accessible variable from a blood test. It is an uncomplicated marker for assessing the extent of liver fibrosis in individuals with CHB. Its diagnostic ability as a single marker can compete with FIB-4 and APRI. [6]
Interleukin-13 (IL-13) is a messenger substance in the immune system. [7] This compound plays a specific role in wound healing and steatohepatitis and has been identified in cohorts with CHB. [8] Multiple studies have demonstrated that IL-13 can influence fibrosis progression through increased collagen production, regulation of proteolytic enzymes, and activation of profibrotic signaling pathways. [8–12] To our knowledge, IL-13 has not been previously established as independently associated with liver fibrosis. Previous studies investigating the association between IL-13 and liver fibrosis have yielded conflicting results. [8–12] Therefore, further confirmation using a more comprehensive analytical approach, multiple linear regression analysis, is warranted. This study aims to evaluate the role of IL-13 in liver fibrosis and to develop a new predictive model that incorporates IL-13, age, and platelet count.
Materials and methods
Participants and data
This study employed a cross-sectional design with a population of CHB patients. Hasan Sadikin General Hospital is one of Indonesia’s premier national referral hospitals, providing the setting for patient selection. Patients were selected from Hasan Sadikin General Hospital’s CHB registry. The CHB registry has been functioning since October 2021 and includes patients over 18 with positive HBsAg results for at least six months. Patients with Hepatitis C, autoimmune liver disease, HIV, type 2 diabetes mellitus, heart disease, chronic kidney disease, pulmonary tuberculosis, cancer, history of alcohol use (20 grams per day), pregnant or breastfeeding women, body mass index (BMI) >27 kg/m^2^, hemoglobin <5 g/dL, pulmonary fibrosis, and chronic pancreatitis are not included in this registry. The participants for this study were drawn from the same registry as the Mac-2-Binding Protein Glycosylation Isomer (M2BPGi) study, which has been previously described in detail. [13] Blood samples and FibroScan® measurements were obtained from patients prior to the initiation of hepatitis B therapy.
The number of patients studied was 88 from 21 October 2021 until 21 January 2022. According to the rule of thumb method, 5−10 subjects per independent variable were enough for multivariate linear regression analysis. Thus, 15−30 subjects are needed for three independent variables. Using the α of 5%, β of 20%, and R^2^ of 0.25, with three independent variables, the minimum sample size is 37 subjects. A sample size of 88, if included in the equation to assess the minimum sample size needed to create a prediction model, also met the criteria. [14] Following a systematic review and adherence to research and professional ethics guidelines, the Research Ethics Committee of Dr. Hasan Sadikin General Hospital in Bandung approved this research (LB.02.01/X.6.5/299/2021). All patients received research information and completed a written consent form. Patients would undergo demographic data collection, complete blood count, IL-13 serum examinations, and TE on the same day. All laboratory examinations were carried out in the clinical pathology laboratory of Hasan Sadikin General Hospital.
Predictors
Three independent variables were used as predictors. The age variable was calculated from the examination date minus the date of birth. Numbers were rounded down so that the age variable could be collected without decimal places. The platelet count variable was listed in new units (×10^9^/ dL) to assess changes per 10,000 platelets in international units (×10^9^/ L). Age and platelet count were analyzed as numerical variables.
IL-13 was measured with the IL-13 ELISA Kit (Elabscience Biotechnology Co., Ltd., Catalog number: E-EL-H0104, Lot: CV05V22Z9069), which uses the Sandwich-ELISA principle method. The serum was mixed with the antibodies specific to Human IL-13, biotinylated detection antibodies specific to Human IL-13, and Avidin-Horseradish Peroxidase (HRP) conjugate. Furthermore, the optical density (OD) was measured spectrophotometrically at 450 nm ± 2 nm to assess the concentration of human IL-13. IL-13 values were analyzed as the nominal variable.
Outcomes
The outcome variable in this research is Liver Stiffness Measurement (LSM), which was obtained from TE results expressed in kPa units. This examination was performed with the FibroScan® 502 Series F00734 (Echosen, Paris, France) with the M probe. The TE method required a minimum of 10 valid readings, ensuring a 60% success rate and an interquartile range below 30% of the median values obtained. A gastroenterohepatologist performed the TE examination on the same day as other examinations at the Hasan Sadikin General Hospital. From now on, the LSM variable underwent data transformation to obtain a normal distribution called the inverseLSM variable.
Statistical analysis
Initially, a normality test was carried out to see the distribution of each variable used. The IL-13 variable was made into categorical data (ILcut5) based on the cut-off value previously obtained through receiver operating characteristic (ROC) curve analysis and the implementation of the Youden index calculation. Bivariate analysis was performed on inverseLSM as the dependent variable and age, platelets, and ILcut5 as independent variables. Multiple linear regression (MLR) analysis was done with the three predictor variables (age, platelet count, and IL-13) at once to see their role in determining the inverseLSM value.
We checked all assumptions during the multiple linear regression (MLR) analysis to validate the results. The Durbin-Watson statistics were used to assess the independence of observations within the model. Scatterplots were analyzed to examine the relationships between the predictors and the outcomes. The homoscedasticity of the model was evaluated through scatterplots and the Breusch-Pagan test. We detected multicollinearity using the bivariate correlation test, variance inflation factor (VIF), and tolerance metrics derived from the collinearity statistics. Outliers were identified using Cook’s distance, standardized residuals, and scatterplots. The distribution of residuals was assessed through the P-P plot, normality tests, and standardized residuals. SPSS version 20 (IBM Corp. 2011. Armonk, NY, USA, RRID: SCR_00286) was used for statistical analysis, and a p-value <0.05 was statistically significant.
Results
Subject characteristics
From October 2021 until January 2022, 102 patients were found with complete data. Every patient who was willing to participate would be included in the study. Then, 88 patients were analyzed. The overall characteristics of the 88 participants are explained in Table 1.
Table 1: Overall characteristics of 88 study participants.
Model development
Through ROC curve analysis followed by computing the Youden index to maximize sensitivity and specificity, the cut-off for IL-13 was obtained at 5 pg/ mL in the diagnosing HR group. Any IL-13 values greater than or equal to 5 pg/ mL will be categorized as positive for the IL-13 examination (ILcut5 = 1). The outcome variable became normally distributed after transforming the LSM variable into the inverseLSM. The normality test results after the transformation of the outcome variable and the selection of the predictor variable type are listed in Table 2.
Table 2: The normality test results of each variable.
Age, platelet count, and inverseLSM were normally distributed, so they were valid for inclusion in multivariate linear regression analysis as numerical data (Table 2). Before developing the prediction model, the correlations between variables were analyzed (Table 3).
Table 3: Bivariate correlation results between dependent and independent variables.
Based on Table 3, there was a correlation between each variable. The highest correlation between variables did not exceed 0.7, indirectly indicating no multicollinearity if further analysis was conducted. Moreover, each independent variable had a p-value of <0.25, which can be included in the subsequent multivariate analysis. MLR analysis was performed using the age and platelet count as continuous variables, and the IL-13 was applied as a nominal variable using the cut-off value obtained, the ILcut5. Through MLR analysis, a prediction model for inverseLSM was formulated. (Table 4).
Table 4: Multivariate analysis to identify independent predictors of inverseLSM value.
The model had an R-squared of 0.37, which means that this model covered 37% of the variance in the inverseLSM results. Significant results were obtained from ANOVA analysis to predict inverseLSM (p-value < 0.001). The Durbin-Watsons test result was 1.686. Two conclusions were obtained from the analysis of the Durbin-Watson table: there was no negative autocorrelation, but it was still inconclusive for positive autocorrelation. Plotting the dependent variable against the regression standardized predicted value gave a linear impression. The scatterplot involving standardized predicted values and standardized residual data was equal in the four quadrants. It can be concluded that the residuals did not increase with the increment of the independent variable. A computerized Breusch Pagan analysis yielded a p-value greater than 0.05. The Cook’s distance was between 0.00 and 0.062, and the standardized residual values were (−2.5) to (+2.45). When plotted on a P-P plot, the standardized residual values sufficiently aligned to create a straight diagonal line, indicating that both the residuals and standardized residuals followed a normal distribution. Analysis of the tolerance value was always greater than 0.1, and the VIF values were always smaller than 10, sufficient to prove that no multicollinearity was found in our model. From the MLR analysis, a predictive equation for inverseLSM was produced as follows:
ILcut5 = 1, if IL-13 ≥ 5 pg/ mL
The model had no autocorrelation, no multicollinearity, no significant outliers, had the appearance of a normal distribution, and met the homoscedastic criteria. In exploratory analyses, we observed statistically significant interactions between IL-13 and age (p = 0.02) and between IL-13 and platelet count (p = 0.022). However, each interaction explained only a small proportion of the overall variance (R² = 0.06) (S1 Table).
Discussion
Our study showed a significant correlation between age, platelet, and IL-13 to LSM values. (Table 4). Aging will increase LSM values, assuming that young age is still in the immunotolerant phase and significant fibrosis has not been found. There was a significant difference in LSM values in each age group. [15] The increase in LSM will be accompanied by a decrease in platelets in this study. Platelet count was found to have a correlation coefficient of −0.495 with LSM from a Spearman test.(15) We obtained a correlation coefficient 0.326 for platelet count in an inverseLSM predictive model from multiple linear regression analysis. Another study also supports this possibility; the platelet count decreased with each increase in the METAVIR score from F0 to F4 in patients with CHB. [6] The rise in IL-13 levels also increased LSM values. IL-13 later induces connective tissue growth factor (CTGF) in HSCs. [16] Another effect of IL-13 release is to cause HSCs proliferation and simultaneously increase the expression of TGF-β and platelet-derived growth factor (PDGF), which play a significant role in the chronic course of liver fibrosis [17].
Most previous studies analyzed predictors for liver fibrosis using logistic regression analysis. Therefore, their analyses could not be directly compared to our results, which resulted from a multivariate linear regression analysis. The coefficient correlation from the highest to lowest were defined by platelet count, IL-13, and Age with 0.326, −0.288, and −0.221, respectively, in predicting inverseLSM. In an analysis of various independent variables in patients with CLD, age was only proven to be a predictor of LSM > 7 kPa in the univariate logistic regression analysis with OR: 1.05 (95%CI 1.03–1.07). Platelet count showed more vital ability in a multivariate logistic regression analysis with OR: 0.981 (95%CI 0.972–0.99). [18] Similar results were seen in CHB-only patients; age was only significant in univariate logistic regression predicting Batts and Ludwig score ≥F2. The Platelet count had a p-value of 0.01 in the multivariate logistic regression with OR: 0.994 (95%CI 0.99–0.999). [19] In predicting Ishak score ≥F2, Platelet count was the only independent predictor in multivariate logistic regression with OR: 0.9 (95%CI 0.9–1). Meanwhile, the age variable was insignificant from univariate or multivariate logistic regression. [20] Although no one used the MLR analysis method as we did, there were quite different results from ours, which found that platelet count and age could predict LSM synchronously.
The role of IL-13 in hepatitis B was recently discovered in a Malaysian cohort. Plasma IL-13 was independently associated with increasing hepatic steatosis as assessed by the controlled attenuation parameter (CAP) examination. In that study, IL-13 was unrelated to LSM outcome scores. [8] Our optimal IL-13 cut-off was identified using the Youden index, which selects the threshold that maximizes the combined sensitivity and specificity on the ROC curve. [21] This approach was applied to our internal dataset to derive a cut-off that provides a balanced discrimination performance while maintaining clinical interpretability within the characteristics of the studied cohort. A positive for ILcut5 was associated with a decrease in inverseLSM of 0.288; in other words, an increase in IL-13 was associated with an increase in LSM. (Table 4) Recent studies have shown that fibrogenesis in CLD patients depends on the effects of IL-13. [9] In patients with HCV, IL-13 expression decreased proteinase and collagenase expression, thus correlated with fibrosis stage. [10] HIV-HCV coinfected patients showed a higher IL-13 value in severe liver fibrosis condition determined by FIB-4 > 3.25. [11] Through receptor, gene, and protein expression analysis, IL-13 induces type I collagen production in IL-13 receptor subunit α2 – positive (IL-13Rα2-positive) HSC via the transforming growth factor-β (TGF-β) pathway. [12] Another related receptor is IL-13 receptor subunit α1 (IL-13Rα1) for Janus kinase/signal transducer and activator of transcription-6 (JAK-STAT-6) signal transduction which causes the production of Eotaxin-1 (CCL11), an eosinophil chemotactic protein. CCL11 was always independently associated with LSM in all models through the MLR analysis [8].
Potential interaction effects were explored by incorporating interaction terms between IL-13 and clinically relevant variables. Although both the IL-13–age interaction and the IL-13–platelet count interaction reached statistical significance in our study, their modest effect sizes, together with the limited sample size, warrant cautious interpretation. Further studies in larger population are needed to clarify whether these interactions represent meaningful biological or clinical effect modification.
Single, indirect liver fibrosis biomarkers were significant in determining liver fibrosis status; notable examples include AST, ALT, Albumin, alkaline phosphatase (ALP), gamma-glutamyl transferase (GGT), bilirubin, total leukocytes, and INR. [19,22] Our analysis did not incorporate these potential predictors when constructing the liver fibrosis model, which may explain the low R-squared value obtained. Liver fibrosis is a series of complex processes based on chronic injury to the liver, which will later trigger oxidative stress and, if left untreated, will cause chronic inflammation. This process will cause wound healing in the liver, which, if repeated, will cause liver fibrosis [23].
The primary and assumptions tests indicated that our overall analysis was unbiased, consistent, and efficient in estimating the regression coefficients and the standard errors. However, this study has several limitations. Firstly, the participants were exclusively CHB patients, meaning our findings only apply to this group. Consequently, external validation studies are necessary to evaluate the applicability of our model to other CLD groups. Despite this limitation, developing a predictive model for liver fibrosis is essential to supporting health services without TE and developing the treasure of science. Second, because some previous studies showed that the role of IL-13 was only related to liver steatosis, further confirmation is needed to investigate its role in liver fibrosis. Discrepancies between our findings and prior reports may be attributable to biological variability across populations, differences in patient characteristics, variations in IL-13 measurement techniques, and heterogeneity in analytical approaches. In addition, the IL-13 cut-off obtained was derived from our internal cohort and may be influenced by population characteristics and assay differences, while dichotomizing a continuous variable may reduce statistical power and lead to population-specific thresholds. Although our sample size met the minimum requirements for model development, the relatively small number of participants may limit model stability and reduce the ability to detect interaction effects. Therefore, both the proposed IL-13 cut-off and the predictive model require validation in larger and independent populations before broader application.
Conclusion
In conclusion, it has been established that IL-13 is independently associated with liver fibrosis, making it a significant part of the predictive model for liver fibrosis in CHB. Higher IL-13 levels, reduction in platelet count, and advanced age appear to play a role in enhancing liver stiffness. The application of MLR analysis in this study provides a very important methodological basis for future research. This study is anticipated to broaden scientific insights and support the advancement and acceleration of CHB management.
Supporting information
S1 TableExploratory Interaction Analyses in Multiple Linear Regression Models.Available at https://doi.org/10.6084/m9.figshare.31479409.(DOCX)
S2 TableThe Raw Study Data.Available at https://doi.org/10.6084/m9.figshare.28388003.v1.(XLSX)
S3 TableThe TRIPOD Checklist for the Development of A Prediction Model.Available at https://doi.org/10.6084/m9.figshare.28425002.v1.(PDF)
S4 TableThe Statistical Analysis Step.Available at https://doi.org/10.6084/m9.figshare.28425038.v1.(DOCX)
S1 FigThe Supporting Plot for the Model.Available at https://doi.org/10.6084/m9.figshare.31479883.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO). Guidelines for the prevention, diagnosis, care and treatment for people with chronic hepatitis B infection. 2024. 1–272.40424433 · pubmed ↗
- 2Dusheiko G, Agarwal K, Maini MK. New approaches to chronic hepatitis B. N Engl J Med. 2023;388(1):55–69. doi: 10.1056/NEJ Mra 2211764 36599063 · doi ↗ · pubmed ↗
- 3Wai C-T, Greenson JK, Fontana RJ, Kalbfleisch JD, Marrero JA, Conjeevaram HS, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38(2):518–26. doi: 10.1053/jhep.2003.50346 12883497 · doi ↗ · pubmed ↗
- 4Sterling RK, Lissen E, Clumeck N, Sola R, Correa MC, Montaner J, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006;43(6):1317–25. doi: 10.1002/hep.21178 16729309 · doi ↗ · pubmed ↗
- 5Georgieva M, Xenodochidis C, Krasteva N. Old age as a risk factor for liver diseases: Modern therapeutic approaches. Exp Gerontol. 2023;184:112334. doi: 10.1016/j.exger.2023.112334 37977514 · doi ↗ · pubmed ↗
- 6Zhong L-K, Zhang G, Luo S-Y, Yin W, Song H-Y. The value of platelet count in evaluating the degree of liver fibrosis in patients with chronic hepatitis B. J Clin Lab Anal. 2020;34(7):e 23270. doi: 10.1002/jcla.23270 32363594 PMC 7370727 · doi ↗ · pubmed ↗
- 7Roeb E. Interleukin-13 (IL-13)—a pleiotropic cytokine involved in wound healing and fibrosis. Int J Mol Sci. 2023;24(16).10.3390/ijms 241612884 PMC 1045484437629063 · doi ↗ · pubmed ↗
- 8Wong S-W, Ting Y-W, Yong Y-K, Tan H-Y, Barathan M, Riazalhosseini B, et al. Chronic inflammation involves CCL 11 and IL-13 to facilitate the development of liver cirrhosis and fibrosis in chronic hepatitis B virus infection. Scand J Clin Lab Invest. 2021;81(2):147–59. doi: 10.1080/00365513.2021.1876245 33528280 · doi ↗ · pubmed ↗