What is new in Freezing of Gait?
Eileen Gülke, Simon J. G. Lewis

TL;DR
This paper reviews recent advancements in understanding and managing freezing of gait in Parkinson's disease.
Contribution
The paper highlights new clinical definitions, outcome measures, and technological approaches for freezing of gait.
Findings
The ICFOG introduced updated definitions and a standardized testing protocol for FOG.
New ClinRO and PRO outcome measures are being developed for FOG assessment.
Technological advances are enabling personalized treatment strategies for FOG.
Abstract
Freezing of Gait (FOG) research is entering a rapidly evolving phase. Published in early 2026, the International Consortium for FOG (ICFOG) released updated clinical and technical definitions of FOG and introduced a consensus-based standardized testing protocol, the Giladi protocol (GP-FOG), which is currently still under evaluation in an ongoing study. Complementing these advances, two new outcome measures, the clinician-reported outcome (ClinRO) and the patient-reported outcome (PRO), are highlighted in this review. Recent technological developments in both detection and potential prevention of FOG are moving the field toward individualized, biomarker-based, on-demand treatment strategies. In addition, emerging insights into the pathophysiological mechanisms of FOG, particularly nondopaminergic contributions, are discussed. Together, these developments provide a contemporary framework…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
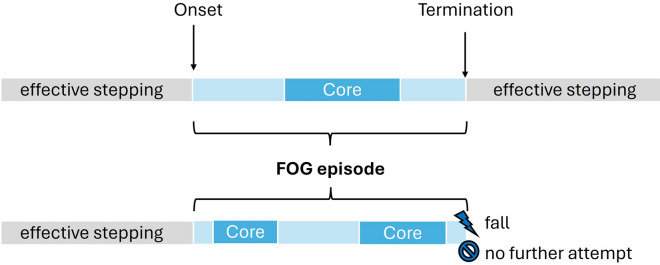 Figure 1
Figure 1- —http://dx.doi.org/10.13039/501100001659Deutsche Forschungsgemeinschaft
- —National Health and Medical Research Council Leadership Fellowship
- —Macquarie University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParkinson's Disease Mechanisms and Treatments · Balance, Gait, and Falls Prevention · Neurological disorders and treatments
Introduction
A substantial body of new work has emerged in the field of Freezing of Gait (FOG) in recent years, making an updated synthesis both timely and necessary. FOG is a common and highly disabling gait disturbance in Parkinson’s disease (PD), typically triggered during gait initiation, turning, or navigating narrow spaces, with around 80% of patients experiencing FOG across all disease stages [31]. In particular, FOG is strongly associated with reduced quality of life, an increased risk of falls and fractures, and greater loss of independence [59]. FOG is characterized by its paroxysmal and sudden onset, often described as a sensation of the feet being “glued” to the floor. Its episodic nature and clinical heterogeneity complicate experimental investigation, objective measurement, and reliable scoring in both clinical practice and research. These challenges have contributed to considerable heterogeneity in how FOG is defined, assessed, and reported across studies [25].
To address these limitations, the International Consortium for FOG (ICFOG) was established to bring together clinical and technical expertise and to develop a unified framework for FOG research. This review builds on these efforts by introducing the updated clinical and technical definitions of FOG, outlining a new testing protocol for accurately assessing FOG ‘on the fly’ and through video-based analysis, and presenting two upcoming rating scales: the clinician-reported (ClinRO) and patient-reported outcome (PRO). In addition, recent advances in technology-assisted assessment and treatment approaches are highlighted, reflecting the rapidly evolving landscape of FOG research and management. We conclude by reviewing current pathophysiological mechanisms, with a focus on nondopaminergic contributions.
The clinical and technical definition of FOG
Why are two distinct definitions of FOG required, and what are the differences? The previously widely used definition proposed by Nutt et al. from 2011, describing FOG as a brief, episodic absence or marked reduction of forward progression of the feet despite the intention to walk [67], led to ambiguity in FOG classification, particularly with respect to episode duration and the presence of effective forward progression. The updated 2026 ICFOG clinical definition describes FOG as *paroxysmal episodes wherein there is an inability to step effectively, despite attempting to do so *[25]. A major advantage of this revised clinical definition is that FOG may occur during any gait-related stepping movement, including turning, step initiation, and walking in any direction, and can be easily applied in clinical settings. The attempt to step can be verified through self-report, observable body movements, or sensor-based measures, while the inability to step effectively is judged by the assessor relative to the individual’s own normal stepping pattern.
With regards to the technical definition of FOG, video scoring remains the gold-standard method for assessing FOG in clinical trials and research studies, typically quantified as the percentage of time spent with FOG in relation to the total task duration (%TF) [24]. Within the ICFOG framework, the onset of a FOG episode is defined as either the moment when any part of the foot lifts off the ground as part of the first ineffective step or the first attempt to initiate a step that does not result in any observable foot movement. A FOG episode ends with 1) no further attempt to take a step, 2) two consecutive effective steps that resemble typical stepping performance, or 3) a FOG-induced fall. Importantly, as FOG does not always involve a complete cessation of forward progression, the core of the episode, formerly referred to as motor blocks [22], may be additionally labeled and may occur once or repeatedly at any point during the FOG episode. The technical definition, therefore, distinguishes between FOG onset, FOG termination, the FOG core, and different FOG manifestations (Fig. 1). These manifestations include akinetic, kinetic-trembling, and kinetic-no-trembling FOG. Akinetic FOG is characterized by a complete cessation of lower-limb movement, whereas kinetic-trembling FOG is defined by rapid oscillatory movements. Kinetic-no-trembling FOG includes any other ineffective movements, such as paroxysmal shuffling or festination-freezing. Notably, continuous gait impairments, such as persistent shuffling or reduced step length, are not considered FOG under this definition. For further details and supplementary video material, please refer to Gilat et al., 2026 [25].Fig. 1. Visualization of the technical definition of FOG. A FOG episode begins with the first ineffective step or attempt to take a step and ends with 1) no further attempt to take a step, 2) two consecutive effective steps that resemble typical stepping performance, or 3) a FOG-induced fall. During the FOG episode, core events, referring to a complete cessation of movement, may occur. Based on Gilat et al. [25]
The Giladi protocol to objectively measure FOG in clinic and research settings
In addition to an updated FOG definition, a standardized measurement protocol is essential, since current patient-reported outcomes are not sufficiently reliable, and existing FOG testing protocols diverge across studies [25]. A variety of clinical observation measures or instrumented gait assessments have used a range of different tools to assess FOG [56, 73, 94]. However, the utility of these approaches is constrained by several limitations, including insufficient standardization and gold-standard validation, extensive test batteries, no representation of common triggers of freezing (e.g., turning, dual-tasking, navigating doorways), as well as the impression that scores (e.g. the Ziegler FOG score) do not truly reflect clinical severity [30, 53]. To resolve these issues, a newly developed consensus-based FOG-provoking protocol, the Giladi protocol (GP-FOG), using a clinician-reported outcome (ClinRO) to quantify FOG severity in real-time, is currently being validated in an international, multicenter study (FOG-COA, NCT06519279). The Giladi protocol is named in memoriam of our dear colleague Nir Giladi, who made substantial contributions to the ICFOG and the development of these new definitions, the protocol, and outcomes scores. The test itself comprises a series of eight walking trials of varying complexity, as well as common FOG triggers, such as turning on the spot [5, 26] or walking through a doorway [2, 57]. Notably, walking in fast, short steps (“shuffling”) as well as full, rapid turns have been identified as the most sensitive ways to provoke FOG [66]. The GP-FOG consists of eight walking trials, including walking, dual-task walking, carrying a ball, turning, dual-task turning, shuffling around a box, box agility, which includes performing small forward, backward, and lateral steps around a ground-marked square, and walking through a doorway [55]. Dual-tasking involves performing the movement task simultaneously with a serial-3 subtraction task, i.e., counting backward from a randomly selected three-digit number in threes. The test is user-friendly, can be completed within 20 minutes, and does not require any additional equipment. The participants are asked to accomplish each task as quickly and safely as possible, while avoiding any strategies or techniques to prevent FOG.
New rating scales: ClinRO & PRO
Along with the new Giladi FOG-provoking protocol (GP-FOG), a new rating scale, the clinician-reported outcome (ClinRO) is currently being developed by the ICFOG and is being validated in the FOG-COA study above. Current FOG rating scales fall short in rating the complexity of FOG: the MDS-UPDRS part III item 3.11. [29] is often used to evaluate the presence of FOG. Therefore, the participant walks for at least 10 m, turns 180°, and returns to the examiner, which is not a very sensitive approach to assess FOG [45, 66]. Although widely used, the Ziegler FOG score, covering 360° turns, doorway walking, and a dual-task (counting backward) with or without carrying water, also fails to differentiate between episodes of varying frequency or duration [30, 94]. Thus, there is a pressing need for a reliable clinical assessment outcome that can be widely implemented in both clinical and research settings to evaluate FOG severity, incorporating both frequency and duration of freezing episodes.
The patient-reported outcome (PRO) is also currently being developed and validated to evaluate the impact of FOG on a patient’s quality of life and to capture ‘the voice of the patient’, which will be critical when seeking FDA approvals for future therapies. This validation is also part of the ongoing FOG-COA study, described above. Current patient-reported outcome questionnaires, including the Giladi Freezing of Gait Questionnaire [23], the new Freezing of Gait Questionnaire (NFOGQ) [65], and the MDS-UPDRS part II item 2.13. [29] have limited validity and insufficient sensitivity to detect small effect sizes, rendering them unsuitable for clinical trials [37, 74]. The novel PRO that is being evaluated will potentially capture information based on the last 4 weeks from patients and their partners, addressing aspects of emotion, confidence, and self-worth, which could then be correlated with objective measures of FOG.
Advances in technology to measure FOG
While ClinRO and gold-standard video-based ratings remain task-specific, emerging technologies offer the potential for more sensitive and comprehensive FOG assessments across both supervised and unsupervised settings. Notably, objective accelerometry-based measures provide a reliable quantification of freezing severity and mitigate the variability inherent with subjective clinical ratings [62].
Inertial measurement units (IMUs) are among the most commonly used and easily deployable tools for quantifying movement [55]. However, considerable variability remains in sensor number and placement, with current recommendations favoring five sensors in supervised laboratory settings and a single lumbar sensor for unsupervised assessments [55]. Despite their potential, IMU-based FOG detection is limited by the absence of a robust, validated analytical framework [55]. Moreover, unsupervised, continuous at-home IMU monitoring alone is not sufficiently sensitive to capture all aspects of FOG, highlighting the need to combine patient-reported outcomes, in-home FOG-provoking tests, and continuous monitoring to comprehensively assess FOG severity [15]. The Gait Advisors Leading Outcomes for Parkinson’s (GALOP) committee, an advisory committee for the Michael J. Fox Foundation for Parkinson’s Research (MJFF), recommended a minimum set of metadata to accompany standardized gait protocols, including pace, rhythm, asymmetry, variability, and turning measures [54].
The ultimate goal is to sensitively detect FOG in home-based environments, as PD patients’ gait performance in supervised laboratory settings often overestimates patients’ real-life gait abilities [36]. Besides, IMUs need to be permanently worn on the body, and the recording duration is limited by battery life [49]. One promising technology for continuous gait assessment is the potential use of a radar system where electromagnetic waves are transmitted, and the shift in reflected waves is measured, using the Doppler effect to measure the velocity of a participant. Radar provides multiple benefits, being independent of lighting, ensuring participant anonymization, and offering a cost-effective solution [87]. It was initially demonstrated to reliably capture gait characteristics, such as gait speed and step time, in a laboratory setting [87]. A three-node radar network featuring one torso node and two feet nodes has been shown to be the most adequate to extract spatiotemporal gait parameters in PD patients [49]. A recent study applied a low-power radar system in the homes of 50 participants, with and without PD, using a signal strength 1000 times lower than typical home Wi-Fi [46]. Combined with advanced signal processing and machine learning algorithms, this approach successfully assessed in-home gait. Strikingly, radar-measured gait speed correlated with PD severity, including MDS-UPDRS part III total scores, axial symptoms, and Hoehn and Yahr stage. Furthermore, the radar system captured disease progression by monitoring gait decline in a small sub-cohort of two participants over one year and motor fluctuations in response to levodopa intake, with gait speed increasing following medication administration [46]. These novel findings suggest the potential for automatic, wearable-free detection of freezing episodes in home environments.
Advances in technology to prevent FOG
In FOG research, one important aim is to detect freezing episodes before they occur and ultimately prevent them. With emerging approaches, this objective is becoming increasingly attainable. In recent years, electrophysiological signals have been analyzed to identify a typical “freezing signature” with abnormal activity preceding and accompanying FOG episodes. These signals include cortical measures such as electroencephalography (EEG) and functional near-infrared spectroscopy (fNIRS), local field potentials (LFP), and kinematic signals, which may enable the development of multimodal systems for individualized monitoring and prevention of FOG [40].
Electrical activity of cortical neurons can be measured using EEG, which provides high temporal resolution, whereas fNIRS captures hemodynamic responses with better spatial resolution. During a Timed-Up-and-Go (TUG) task, EEG power in the alpha and beta bands increased in the central sensorimotor and occipital regions before the onset of freezing episodes, compared with normal walking, and the actual freezing episodes were associated with significantly increased theta and alpha band power within the central and occipital areas [10]. Furthermore, freezing episodes could be distinguished from voluntary stopping periods, which were associated with increased high-beta power in frontal, central, parietal, and occipital regions, as well as decreases in delta to low-beta power relative to FOG episodes. These findings were corroborated by fNIRS, which demonstrated that turning and doorway negotiation elicit cortical activity patterns resembling those observed during voluntary stopping, characterized by activation of the supplementary motor area (SMA) and prefrontal regions. In contrast, during freezing episodes, prefrontal cortical activation was reduced compared with voluntary stopping. Based on these observations, the authors hypothesized that freezing-provoking tasks may engage a stopping network with increased susceptibility to freezing [14]. However, due to the low signal-to-noise ratio of fNIRS and EEG, a large number of gait cycles must be recorded and analyzed using advanced algorithms to reliably distinguish gait-related from movement-related neural activity [55].
One of the major advances in Deep Brain Stimulation (DBS) technology in recent years has been the introduction of local field potential (LFP) sensing using the SenSight™ electrodes (Medtronic). LFPs reflect the summed postsynaptic activity of neuronal populations in the vicinity of the stimulation target. Within this signal, beta-band oscillations in the subthalamic nucleus (STN) have been consistently associated with motor impairment, particularly bradykinesia, and are modulated by dopaminergic and DBS therapy, with increased beta power serving as a marker of greater motor symptom severity [17, 42, 43]. Current DBS therapy uses continuous, 24/7 stimulation, which may lead to stimulation-related side effects such as dysarthria, stimulation-induced dyskinesia, or neuropsychiatric adverse effects [16, 80, 92]. By leveraging patient-specific beta-band activity, the newly available approach of adaptive DBS (aDBS) enables automatic adjustment of stimulation parameters based on predefined thresholds. However, movement-related LFP fluctuations [63] as well as ECG-artifacts [76] still remain challenging, complicating subsequent analyses. The successful implementation of aDBS still requires substantial clinical experience and research.
Despite overall improvements in global motor outcomes, gait worsening after bilateral subthalamic nucleus (STN) stimulation has been reported in approximately 42% of patients [85]. Furthermore, while DBS generally provides sustained long-term improvement in bradykinesia and tremor, gait performance often declines within the first five years post-implantation [77]. DBS programming troubleshooting strategies include low-frequency stimulation, lateralized subthalamic stimulation, and STN-substantia nigra costimulation [60] [47] [70, 90]. However, these approaches yield mixed results and are often associated with worsening of overall motor scores. A recent approach is to program aDBS for STN-DBS patients experiencing FOG [3]. In fact, a small pilot study confirmed the safety, tolerability, and feasibility of beta-burst driven aDBS for FOG [91]. Theoretically, identifying the FOG spectral biomarker in real time may allow DBS to be dynamically adjusted to either prevent a freezing episode or alleviate freezing episodes [55].
An alternative but well-established clinical strategy to prevent and overcome FOG is through the phenomenon of cueing [72]. Visual and auditory cues help focus attention on walking and shift gait control from habitual to goal-directed motor patterns [28]. In general, visual cues tend to improve stride length, whereas auditory cues primarily enhance cadence [78]. Externally generated cues can even improve gait performance during dual-task conditions [48]. Various, often expensive, cueing devices have been shown to improve gait, such as laser pointers [93] and laser-light shoes with foot pressure and inertial sensors [11]. Nevertheless, repeated exposure can result in habituation, reducing their long-term utility [28]. Moreover, no single cue is universally optimal, as effectiveness depends on individual factors such as cognitive function, and it remains unclear which patients benefit most from specific types of cues [27, 28]. Accordingly, the multicenter UNITE-PD study is currently investigating patient characteristics, changes in cueing efficacy, and the neural correlates of cueing [1]. Additionally, externally generated cues may be less effective than internally generated cues, such as singing [32], highlighting the need for more advanced cueing technologies [68] that integrate electrophysiological and kinematic signals. In line with the concept of aDBS, providing each patient with individually tailored, on-demand stimulation, adaptive cueing could offer similar benefits by responding to a patient’s unique ‘freezing signature’ and potentially preventing FOG before it occurs. Early approaches have shown promising results. For example, a novel on-demand cueing system using instrumented insoles detects FOG episodes via increased variability in step time, and delivers visual cues on demand, resulting in reduced freezing and increased walking speed [68]. Another innovative device, Cue2Walk, employs a single sensor worn on the lateral side of the shank below the knee to provide auditory and/or vibratory cues. Cueing can be triggered manually via a button press or hands-free gesture, such as a heel tap, or automatically, based on real-time detection of FOG episodes using a tri-axial integrated accelerometer and a specialized algorithm [84]. Notably, a model combining IMU and plantar pressure features accurately identified the shift from preFOG to FOG, highlighting its potential application in real-time FOG detection and adaptive cueing [69]. Additionally, analyses using fNIRS and EEG indicated higher parietal alpha activity during cueing in patients at later Hoehn and Yahr stages, which could be used as an electrophysiological signal to identify cueing responders [86]. Together, these findings further underscore the need for an individualized, biomarker-based cueing approach.
Updates on FOG pathophysiology
The pathophysiology of FOG is still not well understood, but likely relates to a loss of automated motor control when there is a processing overload across disseminated neural networks, resulting in gait disturbances [83]. The Neural Reserve or Cross-Talk Hypothesis proposed by Lewis and Barker considers FOG as the momentary breakdown of normal gait, when there is an inability to concurrently process motor, cognitive, and limbic information, which overloads the system [44, 64]. The proposed model further asserts that in overcoming a freezing episode, the patient is able to suspend their performance of additional cognitive and limbic processes. By focusing on a goal-directed behavior, there is a reduction in the degree of over-activation within the output nuclei of the basal ganglia, allowing this circuitry to be ‘‘reset’’, once again facilitating movement. Thus, FOG appears to reflect a lack of neural reserve across shared pathways dealing with incoming information and functional output. A recent review from Tosserams and colleagues highlights the core pathophysiological principles of FOG: (1) loss of gait automation due to basal ganglia neurodegeneration with high inhibitory basal ganglia output, (2) degeneration of compensatory cortical areas, and 3) impaired integration of cerebral compensatory networks [83].
While dopaminergic therapies can improve FOG in some individuals, they do not fully ameliorate FOG symptoms [50]. Levodopa-unresponsive FOG suggests the involvement of nondopaminergic pathways, as does the clinical heterogeneity observed in patients with FOG [19]. Current evidence suggests that noradrenergic, cholinergic, and serotonergic systems might be involved in the pathophysiology of FOG. Beyond dopaminergic contribution, the role of the neurotransmitter noradrenaline has been recently implicated in FOG. An increase in arousal is associated [18, 52] and biologically linked to states of brain network integration implicated in this phenomenon [81, 82]. Effective integration of distinct and segregated brain networks critically relies on the noradrenergic ascending arousal system, which appears to be impaired to varying degrees in patients with FOG [58, 75, 88]. Widespread noradrenergic denervation has been observed in patients with FOG, particularly involving the Locus coeruleus and the thalamic noradrenergic system, both of which are closely linked to limbic circuits implicated in FOG pathophysiology [58]. Atomoxetine is a promising noradrenergic drug, as it is safe and well-tolerated in PD [71, 89]. It is a selective noradrenaline transporter inhibitor (SNRI), which prevents the cellular reuptake of noradrenaline, and is widely used for the treatment of attention-deficit hyperactivity disorder (ADHD) [41]. Atomoxetine has been shown to improve attention, response inhibition, executive functions, and anxiety in PD [89], which are all clinical features that have been associated with FOG severity. However, to date, only inconsistent reports of improvements in FOG have been reported in small samples [39, 71]. The Antifreeze trial (NCT07316296), sponsored by the MJFF, is a multicenter, single-dose, double-blind, placebo-controlled clinical trial with a cross-over design. The goal of this clinical trial is to investigate whether atomoxetine can reduce FOG and identify potential biomarkers for freezing responders.
Regarding cholinergic involvement, the striatum, the pedunculopontine nucleus (PPN), and the nucleus basalis of Meynert (NBM) represent the principal cholinergic sources in the brain and are affected by α-synuclein-related neurodegeneration [6]. Levodopa-unresponsive PD patients experiencing FOG have been shown to exhibit bilateral reductions in cholinergic terminals, predominantly in extrastriatal regions, using vesicular acetylcholine transporter positron emission tomography (VAChT-PET)[12]. Cholinergic deficits have also been demonstrated in patients with PD and a history of falls, suggesting a shared underlying mechanism for falls and FOG within a framework of impaired cognitive integration [7]. Therefore, the PPN has emerged as a promising DBS target, with small pilot studies reporting reductions in FOG and falls in subsets of patients [21, 61]. A currently ongoing clinical trial (NCT04605263) is comparing bilateral STN-PPN DBS with conventional STN-DBS. However, interim results from an exploratory randomized, double-blind, crossover trial did not demonstrate gait improvement after two months of combined STN-PPN DBS in patients with levodopa-resistant gait and balance impairments [9]. Pharmacologically, a randomized, double-blind, placebo-controlled phase II trial (ReSPonD) reported promising results with improved step-time variability in patients treated with rivastigmine, an acetylcholinesterase inhibitor [33]. Nevertheless, the results of the CHIEF-PD trial (NCT04226248), a multicenter, randomized, double-blind, placebo-controlled study evaluating rivastigmine for fall prevention, are still pending.
Apart from noradrenergic and cholinergic deficits, depression, a symptom commonly associated with FOG [20], is linked to the serotonergic dysfunction in PD [4]. Notably, reduced cerebrospinal fluid serotonin levels have been observed in advanced PD patients with gait disorders [38]. Clinical data on serotonergic drug effects on gait function remain limited. However, previously, ritanserin, a highly selective 5-HT2 receptor antagonist, significantly improved gait in 7 out of 10 patients in one small clinical trial [34]. Similarly, a short-term randomized, placebo-controlled 4-week trial found an improved walking speed in patients treated with paroxetine, a serotonin reuptake inhibitor (SSRI), compared to placebo [13]. With regard to FOG, functional MRI studies have revealed reduced functional connectivity between the dorsal raphe nucleus (DRN) and cortical structures, such as the supplementary motor area (SMA), a key region implicated in gait control and FOG [51]. Furthermore, preliminary evidence suggests that both selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) may improve FOG [79].
In summary, nondopaminergic mechanisms underlying FOG may help delineate specific freezer subtypes and inform tailored noradrenergic, cholinergic, or serotonergic treatment strategies.
Conclusion
Altogether, rapid progress in the field is enabling greater standardization in both clinical and research settings. The emergence of on-demand treatment strategies offers new hope for patients with Parkinson’s disease affected by FOG. Beyond identifying freezing episodes and developing potential interventions, the mechanisms underlying why and when nonfreezers transition to freezers remain poorly understood. Several risk factors have been identified and can be categorized into modifiable factors, such as more severe motor and cognitive impairment, and nonmodifiable factors, including older age and longer disease duration [35]. A recent machine-learning-based study further highlighted specific gait characteristics, including step length and stride width across both medication states, that are associated with freezing severity [8]. Understanding these predictors represents a pressing step toward elucidating the mechanisms behind freezing conversion and ultimately guiding targeted, individualized interventions.