Intraoperative sodium range affects white matter microstructure in neonatal congenital heart disease
Mirthe E.M. van der Meijden, Kim van Loon, Maaike Nijman, Hanna Talacua, Johannes M.P.J. Breur, Joppe Nijman, Nathalie H.P. Claessens, Serena J. Counsell, Manon J.N.L. Benders, Alexandra F. Bonthrone

TL;DR
Rapid changes in sodium levels during surgery in newborns with heart defects may harm white matter in the brain, suggesting the need to carefully manage sodium levels to protect brain development.
Contribution
This study is the first to show that intraoperative sodium fluctuations are linked to neonatal white matter microstructural changes after heart surgery.
Findings
A larger intraoperative sodium range was associated with reduced axial diffusivity in specific white matter regions.
No associations were found between diffusivity and sodium rate of change.
Findings suggest axonal injury may result from rapid sodium fluctuations in neonates with congenital heart disease.
Abstract
Intraoperative sodium changes and new postoperative white matter injury are prevalent in neonates with congenital heart disease (CHD) who undergo cardiopulmonary bypass surgery. Rapid sodium correction in hyponatremia is associated with white matter injury in adults. This study examined the potential effects of a rapid intraoperative sodium increase on white matter microstructure in neonates with CHD. 83 neonates with CHD underwent postoperative diffusion weighted magnetic resonance imaging within three weeks of cardiopulmonary bypass surgery as part of routine clinical practice. Mean diffusivity, radial diffusivity, and axial diffusivity were calculated using Diffusion Tensor Imaging. Voxel-wise associations within the core of white matter tracts were assessed using tract-based spatial statistics. Serum sodium measurements were extracted from clinical notes. Maximum intraoperative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
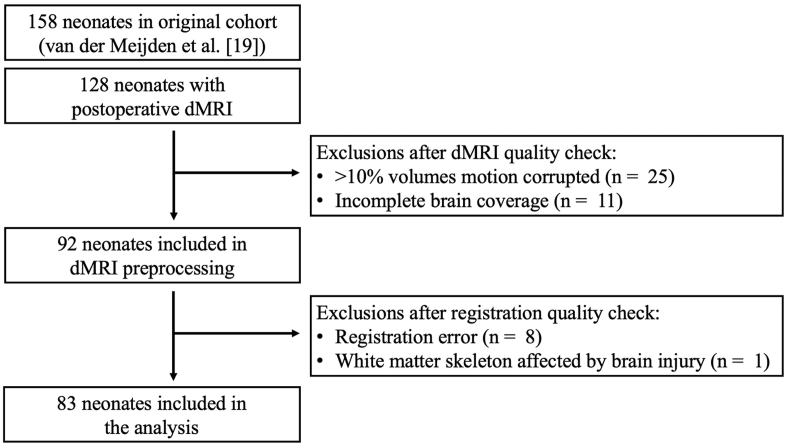 Figure 1
Figure 1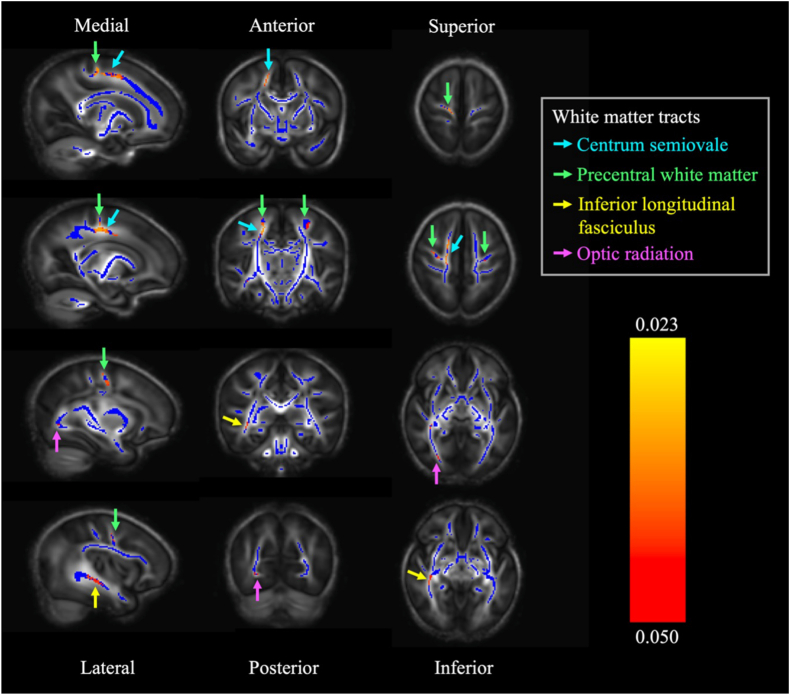 Figure 2
Figure 2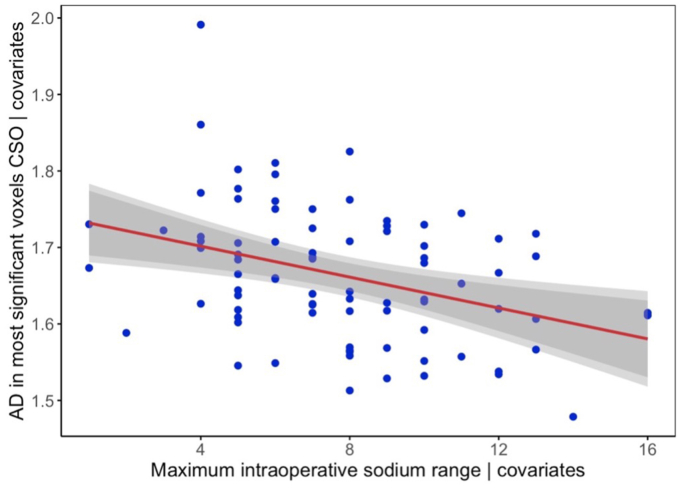 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Heart Failure Treatment and Management · Neonatal and fetal brain pathology
Introduction
1
Congenital heart disease (CHD) is the most prevalent congenital anomaly, affecting the development of cardiac structures and great vessels [1]. Although advances in neonatal cardiac surgery and critical care have increased survival rates throughout the past decades, long-term neurodevelopmental impairment remains prevalent [2].
Altered brain development in CHD originates in utero where altered circulation provides suboptimal cerebral substrate delivery [3], resulting in smaller brain volumes [3] and reduced cortical folding [4] that persists into the neonatal period [5,6]. Diffusion-weighted magnetic resonance imaging (dMRI) studies have shown pre- and postoperative white matter (WM) microstructural alterations in neonates with CHD, including high mean diffusivity (MD) and low fractional anisotropy (FA) compared to heart-healthy neonates [[7], [8], [9]]. White matter injury (WMI) is prevalent before and after surgery [10]. Surgical factors such as neonatal cardiopulmonary bypass (CPB) further increase the risk for new postoperative WMI [10] and altered brain development in early childhood [11]. However, risk factors for postoperative brain changes are multifactorial and not well understood, and studies examining the impact of other potential perioperative risk factors are required.
During CPB surgery, administration of hyperosmolar priming solutions induces a rapid sodium increase when baseline is low, which increases the risk for osmotic demyelination syndrome (ODS) in adults [12]. ODS is a phenomenon characterised by WMI and altered WM microstructure, most commonly related to a rapid correction of hyponatremia [13,14]. On dMRI, adults with ODS show a decrease of apparent diffusion coefficient (ADC), a comparable measure to MD, within the first week, followed by an increase to normal levels around one month after the rapid sodium increase [13,14]. A rapid increase of serum osmolality is hypothesised to induce transcellular water shifts, glial cell shrinkage, and compensatory upregulation of ion transporters and osmolyte synthesis, a metabolically taxing process that depletes adenosine triphosphate [15]. This osmotic stress disrupts tight junctions and the blood-brain barrier, allowing inflammatory mediators to enter the central nervous system and initiate oligodendrocyte apoptosis and demyelination.
Neonates [[16], [17], [18], [19]] and children [[16], [17], [18],20] with CHD show a rapid sodium increase throughout surgery, possibly increasing the vulnerability to new postoperative WMI [10] and WM microstructural alterations [[7], [8], [9]]. In our previous study quantifying the perioperative sodium course in neonates with CHD, the median maximum intraoperative sodium range was 7.0 mmol/L [19]. This approaches the daily threshold of 8.0 mmol/L for a safe sodium correction in adults [21]. Currently, there is no agreed threshold in neonates. We did not report an association between intraoperative sodium changes and new postoperative WMI on qualitative imaging [19]. However, it is plausible that osmotic stress may result in altered WM microstructure rather than overt WMI visible on structural MRI.
This study aimed to assess the relationship between a rapid sodium increase during cardiac surgery with CPB and WM microstructural alterations in neonates with CHD using Diffusion Tensor Imaging (DTI). We hypothesised reduced postoperative diffusion across the WM in neonates with larger intraoperative sodium changes, reflected by decreased MD, radial diffusivity (RD), and axial diffusivity (AD).
Methods
2
Ethical approval and consent
2.1
The Dutch institutional review board approved the study protocol on February 17, 2016 (MREC:16-093). The study adheres to the moral and ethical principles described in the Declaration of Helsinki and good clinical practice [22]. Informed written consent was provided by parents regarding the usage of imaging and clinical data for research purposes.
Study population and design
2.2
From the original cohort described by van der Meijden et al. [19], neonates were eligible for inclusion if they were born after 36.0 gestational weeks and underwent dMRI within three weeks after CPB surgery. Of 158 neonates in the original cohort, 128 neonates who underwent surgery within the first six weeks of life between February 2016 and September 2021 at the Wilhelmina Children's Hospital, Utrecht, The Netherlands, were eligible for inclusion in the study.
Sodium data collection
2.3
Sodium data collection was conducted according to the methods described by van der Meijden et al. [19]. Briefly, per clinical protocol, serum sodium levels of neonates were obtained throughout their hospital stay, primarily by point-of-care testing (Abbott iSTAT). The maximum intraoperative sodium range was calculated per neonate by subtracting the lowest from the highest serum sodium level during surgery. This measure reflects the effects of both the exposure to high sodium fluids (e.g., CPB-priming solution, blood products, and intravenous fluids) and low-sodium cardioplegia (Custodiol-Köhler solution). The time difference in hours between the minimum and maximum intraoperative sodium measure was computed. The rate of the maximum intraoperative sodium change was calculated by dividing the maximum intraoperative sodium range by the time difference. Clinical data were extracted from electronic medical records.
MRI acquisition
2.4
Scanning procedures have previously been reported by Claessens et al. [23]. Neonates were placed in a vacuum mattress and received dual-layer hearing protection before scanning (adhesive ear covers and over-ear muffs). Heart rate, saturation, and breathing were continuously monitored. Neonates were scanned in natural sleep where possible or sedated with oral chloral hydrate before scanning when necessary (50-60 mg/kg). MRI was acquired as part of routine clinical care. Axial dMRI (TR 6500 ms; TE 66 ms; flip angle 90°; slice thickness 2 mm; acquired voxel size 2.25 x 2.25 × 3.00 mm; reconstructed voxel size 2.00 x 2.00 × 2.00 mm, diffusion gradients 45 directions, one b = 0 s/mm^2^ image, b value = 800 s/mm^2^) was acquired on a Philips 3 T system (Philips Medical Systems, Best, Netherlands), using a 32-channel head coil.
dMRI preprocessing
2.5
An overview of participant exclusions is provided in Fig. 1. In preparation of dMRI preprocessing, images were visually quality checked for major motion artefacts.Fig. 1. Diagram summarizing exclusions.Abbreviations: dMRI, diffusion-weighted Magnetic Resonance Imaging.Fig. 1
DMRI images underwent denoising [24,25] and Gibbs de-ringing [26] using the MRtrix3 software package (http://www.mrtrix.org) [27]. Images underwent eddy current distortion and motion correction with outlier rejection and replacement using Eddy from the FSL software package (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki) [28]. A quality check report regarding Eddy corrections was generated using Eddy QUality Assessment for DMRI (QUAD). The mean square residuals plot was used to identify volumes for which motion correction was inadequate. These volumes were visually inspected and excluded when major motion artefacts remained apparent. One or more volumes were removed from 51 (55.4%) datasets (median 2, range 1-4 vol).
Neonatal data processing was undertaken using previously published methods [29]. A diffusion tensor model was fit per voxel using the dtifit tool in FSL (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki) [30]. The outputs of dtifit were converted to tensor images compatible with DTI-ToolKit (DTI-TK v2.3.3 https://dti-tk.sourceforge.net/pmwiki/pmwiki.php). Registration of dMRI tensor images was undertaken using DTI-TK, a validated tool for accurate registration of neonatal dMRI [31]. First, an initial population-specific template was created using dMRI datasets of five neonates that were visually evaluated to be of high-quality and adequate anatomical alignment. Subsequently, rigid-body, affine, and deformable registration were used to align the dMRI data. A high-resolution study specific template was computed by averaging the aligned dMRI images. Commonly used DTI metrics include MD, FA, RD, and AD, corresponding to the average magnitude of water molecular diffusion, the degree of directionality of water molecular motion, and magnitude of water molecular motion perpendicular and parallel to the principal vector per voxel, respectively [32]. The template was used to extract the WM skeleton, comprising the locally maximal FA values reflective of the centre of the WM tracts of the population. MD, RD, and AD maps were computed per neonate and projected onto the skeleton, enabling voxel-wise analyses across neonates. FA was not assessed, as this metric was not expected to change within the short observational period [33].
Statistical analysis
2.6
Analyses were carried out using FSL (v6.0 https://fsl.fmrib.ox.ac.uk/fsl/fslwiki) and RStudio (v1.3.1093) [34]. Normality of continuous variables was evaluated using the Shapiro-wilk test. Normally distributed variables are presented as mean ± SD, non-normally distributed variables as median (IQR), and categorical variables as number (%). In order to assess voxel-wise relationships between maximum sodium range and rate of change, and postoperative MD, RD, and AD, permutation testing was carried out using the randomise tool in FSL (v6.0 https://fsl.fmrib.ox.ac.uk/fsl/fslwiki), using 10000 permutations and Threshold-Free Cluster Enhancement [35], accounting for sex, gestational age at birth, postnatal age at surgery, postmenstrual age at scan, interval between surgery and scan, presence of single ventricle physiology, and CPB duration. To improve model fit, all numerical variables were standardised by subtracting the mean from the observed value and dividing by the standard deviation.
When a significant relationship was identified between intraoperative sodium range and diffusivity metrics, three TBSS models were run as sensitivity analyses with the following additional covariates: (1) use of selective cerebral perfusion (SCP) or deep hypothermic cardiac arrest (DHCA); (2) total intensive care length of stay; (3) cyanotic heart defect, adjusted for sex, gestational age at birth, postnatal age at surgery, postmenstrual age at scan, interval between surgery and scan, presence of single ventricle physiology, and duration of cardiopulmonary bypass.
Results
3
The final cohort consisted of 83 neonates with a total of 2533 validated plasma sodium observations. Baseline characteristics are summarized in Table 1.Table 1. Baseline characteristics.Table 1N = 83Male, n (%)62 (74.7)Gestational age, weeks39.0 ± 1.3Birthweight, grams3360 (3081 – 3545)Duct-dependent CHD subtype78 (94.0)Preoperative administration of diuretics30 (36.1)Age at surgery, days7.0 (5.0 – 9.5)Postmenstrual age at surgery, weeks40.3 ± 1.4Primary surgical procedure, n (%) Arterial switch operation30 (36.1) Aortic arch repair14 (16.9) Norwood procedure18 (21.7) Arterial pulmonary shunt7 (8.4) Arterial switch operation + aortic arch repair5 (6.0) Correction of TAPVC4 (4.8) Aortic arch repair + Ross-Konno procedure2 (2.4) Truncus arteriosus repair2 (2.4) Biventricular repair1 (1.2)Cardiopulmonary bypass duration, min152 (130 – 177)Selective cerebral perfusion, n (%)36 (43.4)Selective cerebral perfusion duration, min38 (31 – 43)Deep hypothermic cardiac arrest, n (%)21 (25.3)Deep hypothermic cardiac arrest duration, min21 (9 – 24)Aortic cross-clamping time, min83 (64 – 112)Time between surgery and MRI, days7.4 (6.4 – 9.3)Values are presented as mean ± SD when distributed normally, as median (IQR) when distributed non-normally, and as number (%) when categorical. Abbreviations: CHD, congenital heart disease; TAPVC, total anomalous pulmonary venous connection; MRI, magnetic resonance imaging.
Intraoperative sodium characteristics
3.1
The intraoperative sodium course is summarized in Table 2. The mean maximum sodium range was 7.7 mmol/L (SD 3.2), within a median surgery duration of 5.6 h (IQR 4.8–6.1). The advised daily limit of safe sodium correction of 8 mmol/L for adults [21] was exceeded by 37.3% of neonates. The corresponding rate of safe sodium correction for the median surgery duration was 1.9 mmol/L (calculated as 8/24∗5.6), which was exceeded by 97.6% of neonates. The median rate of the maximum intraoperative sodium increase was 2.86 mmol/h (IQR -5.3–5.0), which was almost 9 times larger than the hourly rate of safe sodium correction of 0.33 mmol/L/h in adults (calculated as 8/24).Table 2. Intraoperative sodium course.Table 2NAverageMin-MaxSodium level, mmol83139.0 (135.0 – 141.0)125.0 – 152.0Pre-CPB sodium, mmol67137.4 ± 3.5128.0 – 144.0CPB priming solution, mmol76167.8 ± 3.4158.0 - 178.0Max. sodium range, mmol837.7 ± 3.21.0 – 16.0Max. sodium range interval, h830.67 (−0.80 – 1.81)−3.88 – 4.30Max. sodium increase rate, mmol/h832.86 (−5.29 – 5.0)−50.0 – 34.29Values are presented as mean ± SD when distributed normally, as median (IQR) when distributed non-normally, and as number (%) when categorical. Abbreviations: CPB, cardiopulmonary bypass.
Voxel-wise analyses
3.2
Voxel-wise analysis of postoperative AD revealed that a higher maximum intraoperative sodium range was associated with lower AD values in the right centrum semiovale, precentral WM (right > left), right inferior longitudinal fasciculus, and right optic radiation (p < 0.05) (Fig. 2). The relationship between mean AD within the significant voxels of the centrum semiovale and the maximum intraoperative sodium range adjusted for the covariates is presented in Fig. 3. The inclusion of SCP/DHCA, total intensive care length of stay, or cyanotic heart defect as an additional covariate in the TBSS model did not affect the association between maximum intraoperative sodium range and AD (p < 0.05) (Supplementary Figs. 1, 2, & 3). MD and RD were not associated with maximum intraoperative sodium range. No relationship was evident between postoperative MD, AD, or RD and the rate of the maximum intraoperative sodium increase.Fig. 2. White matter regions that show a significant negative relationship between maximum intraoperative sodium range and postoperative axial diffusivity (red/orange/yellow, p < 0.05), overlaid on fractional anisotropy skeleton (blue) and mean fractional anisotropy map (grey). All sagittal images are selected from the right hemisphere.Fig. 2. Fig. 3Scatterplot showing the relationship between mean axial diffusivity in the significant voxels within the centrum semiovale and maximum intraoperative sodium range adjusted for the covariates.Abbreviations: CSO, centrum semiovale; AD, axial diffusivity.Fig. 3
Discussion
4
To our knowledge, this is the first study examining the effects of serum sodium rise during cardiac surgery on WM microstructure in neonates with CHD. Concordant with our hypothesis, we report that larger intraoperative sodium ranges were associated with decreased AD in the right centrum semiovale, bilateral precentral WM, right inferior longitudinal fasciculus, and right optic radiation. Of note, SCP/DHCA, total intensive care length of stay, and presence of a cyanotic heart defect did not affect the relationship between maximum intraoperative sodium range and AD. The rate of the maximum intraoperative sodium change was not associated with MD, AD, or RD.
The observation of reduced AD in WM of neonates with a larger intraoperative sodium range is partially aligned with adult ODS case reports, showing reduced ADC, a measure of average diffusivity, approximately one week after a rapid sodium increase [13,14]. However, to our knowledge, adult ODS studies have not assessed changes in AD and RD. The observation of reduced AD, but not MD and RD, may therefore be better understood by considering diffusion changes in other neonatal conditions in which oligodendrocyte injury is prevalent, such as hypoxic-ischemic encephalopathy. Neonates with hypoxic-ischemic encephalopathy show an initial decrease of MD after ischemia [36], similar to the decrease of ADC observed in adult ODS. Additionally, a neonatal mouse model of retinal ischemia has provided a more detailed pattern of diffusivity changes, indicating initial reduced AD and MD within the first three days after ischemia, followed by increased RD and MD [37]. These diffusivity changes are reflective of axonal injury and demyelination, respectively, corroborated by histological reports. It is possible that our observations reflect the phase of axonal injury where AD remains low, but RD and MD have started to normalize. However, adults with ODS show normalization of ADC approximately one month after the rapid sodium increase [13,14], whereas normalization in neonates with hypoxic-ischemic encephalopathy occurs between 6 and 12 days after ischemia [36]. We are unaware of any studies assessing the relationship between sodium changes, diffusivities and histological changes in the neonatal brain. Neonates in the current cohort were scanned median 7.4 days after surgery, hence the observed decreased AD could be more aligned with the slower time course of diffusivity changes in adult ODS. Nonetheless, despite the shared biological stressor of rapid sodium increase, adult ODS typically follows rapid correction of hyponatremia and is influenced by additional clinical factors [15], whereas only 31% of neonates are hyponatremic in the 72h before CPB surgery [19], and the sodium increase occurred intraoperatively. More research is needed to clarify the exact time course and underlying mechanisms of WM microstructure alterations in relation to intraoperative sodium changes in neonates with CHD. MRI at 3 months post-surgery could provide valuable insight into the time course of WM microstructure alterations in response to intraoperative sodium change.
The reasons underlying the regional specificity of the effect of maximum intraoperative sodium range in our study are unclear. It is possible that some WM regions are more susceptible to osmotic stress than others. One study examining brain injury in neonatal hypernatremic dehydration, a condition where water is transported from the body at a faster rate than sodium, reported cytotoxic edema in the centrum semiovale [38]. Although the underlying conditions differ, this finding supports the current finding that the centrum semiovale may be particularly sensitive to osmotic fluctuations. However, there have been no previous studies linking the precentral WM, inferior longitudinal fasciculus, or optic radiation to sodium changes. Further investigation is needed to understand why these regions may be particularly vulnerable to osmotic stress.
Current findings expand on our previous work [19], underscoring the importance of close monitoring and minimization of osmotic stress during CPB surgery in neonates with CHD. To limit the range of intraoperative sodium observations and reduce fluid shifts, low- and high-sodium fluids should be administered with caution. The perioperative protocol at the Wilhelmina Children's Hospital, Utrecht, The Netherlands, has been changed accordingly, by diluting vasoactive medication in glucose 10% to reduce sodium load.
Interpretation of our results is complicated by the complex multifactorial origin of perioperative brain alterations in CHD, where it is difficult to isolate the effects of osmotic stress maximum intraoperative sodium range on WM microstructure from other surgical and clinical factors. Hemodynamically unstable neonates receive more intraoperative fluids, possibly increasing the range of sodium values and potentiating fluid shifts. Moreover, indicators of hemodynamic instability such as low cardiac output, are associated with increased risk of brain injury [24]. Maximum sodium range could be a marker of hemodynamic instability rather than a causal factor for alterations in WM. However, sensitivity analyses assessing the influence of SCP/DHCA, total intensive care length of stay, and cyanotic heart defect did not alter the results of our study. Further studies with larger sample sizes are required to disentangle factors across fetal, preoperative and postoperative periods associated with brain development in this population. Additionally, we did not account for all surgical variables in the TBSS model, as diagnosis, surgical procedure, and perioperative factors are highly correlated. We included presence of single ventricle physiology and duration of cardiopulmonary pass, due to their established association with new WMI [10,39]. Lastly, not all neonates from the original cohort [19] had dMRI available. Clinical instability was the primary reason MRI was not obtained within three weeks after surgery, this cohort therefore likely reflects the effects of sodium in more clinically stable neonates with CHD. Moreover, the implications of sodium-related WM microstructural changes for long-term neurodevelopment remain unclear. Large prospective studies integrating disease complexity indices, perioperative neuroimaging, and long-term follow-up are required to understand how sodium-related WM alterations evolve and relate to later WM injury and long-term neurodevelopmental outcomes.
In conclusion, the current study suggests a large intraoperative sodium range is associated with altered WM microstructure in the centrum semiovale, precentral WM, inferior longitudinal fasciculus, and optic radiation. This finding may have important implications for perioperative sodium regulation protocols to support WM microstructure development in neonates with CHD undergoing CPB surgery.
CRediT authorship contribution statement
Mirthe E.M. van der Meijden: Writing – review & editing, Writing – original draft, Visualization, Investigation, Formal analysis, Data curation, Conceptualization. Kim van Loon: Writing – review & editing, Supervision, Data curation, Conceptualization. Maaike Nijman: Writing – review & editing, Data curation. Hanna Talacua: Writing – review & editing. Johannes M.P.J. Breur: Writing – review & editing. Joppe Nijman: Writing – review & editing. Nathalie H.P. Claessens: Writing – review & editing. Serena J. Counsell: Writing – review & editing, Supervision, Funding acquisition, Conceptualization. Manon J.N.L. Benders: Writing – review & editing, Supervision, Funding acquisition, Conceptualization. Alexandra F. Bonthrone: Writing – review & editing, Supervision, Methodology, Conceptualization.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1van der Linde D.Konings E.E.M.Slager M.A.Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis JACC (J Am Coll Cardiol)5820112241224710.1016/j.jacc.2011.08.02522078432 · doi ↗ · pubmed ↗
- 2Moons P.Bovijn L.Budts W.Belmans A.Gewillig M.Temporal trends in survival to adulthood among patients born with congenital heart disease from 1970 to 1992 in Belgium Circulation 12220102264227210.1161/CIRCULATIONAHA.110.94634321098444 · doi ↗ · pubmed ↗
- 3Sun L.Macgowan C.K.Sled J.G.Reduced fetal cerebral oxygen consumption is associated with smaller brain size in fetuses with congenital heart disease Circulation 13120151313132310.1161/CIRCULATIONAHA.114.01305125762062 PMC 4398654 · doi ↗ · pubmed ↗
- 4Ortinau C.M.Rollins C.K.Gholipour A.Early-emerging sulcal patterns are atypical in fetuses with congenital heart disease Cerebr Cortex 2920193605361610.1093/cercor/bhy 235PMC 664486230272144 · doi ↗ · pubmed ↗
- 5Ortinau C.Alexopoulos D.Dierker D.Van Essen D.Beca J.Inder T.Cortical folding is altered before surgery in infants with congenital heart disease J Pediatr 16320131507151010.1016/j.jpeds.2013.06.04523988135 PMC 3905308 · doi ↗ · pubmed ↗
- 6Claessens N.H.P.Khalili N.Isgum I.Brain and CSF volumes in fetuses and neonates with antenatal diagnosis of critical congenital heart disease: a longitudinal MRI study AJNR 40201988589110.3174/ajnr.A 602130923087 PMC 7053893 · doi ↗ · pubmed ↗
- 7Hagmann C.Singer J.Latal B.Knirsch W.Makki M.Regional microstructural and volumetric magnetic resonance imaging (MRI) abnormalities in the corpus callosum of neonates with congenital heart defect undergoing cardiac surgery J Child Neurol 31201630030810.1177/088307381559121426129977 · doi ↗ · pubmed ↗
- 8Mulkey S.B.Ou X.Ramakrishnaiah R.H.White matter injury in newborns with congenital heart disease: a diffusion tensor imaging study Pediatr Neurol 51201437738310.1016/j.pediatrneurol.2014.04.00825160542 PMC 4147255 · doi ↗ · pubmed ↗