Cabozantinib versus placebo in patients with radioiodine-refractory differentiated thyroid cancer after prior vascular endothelial growth factor receptor-targeted therapy (COSMIC-311): outcomes by BRAF status
Marcia S. Brose, Bhumsuk Keam, Jolanta Krajewska, Ana O. Hoff, Fernanda Vaisman, Chia-Chi Lin, Erika Hitre, Daniel W. Bowles, Bruce Robinson, Steven I. Sherman, Nuttapong Ngamphaiboon, Xiang Guo, Andrew Simmons, Denise Williamson, Svetlana Andrianova, Nicholas Berry

TL;DR
This study shows that cabozantinib improves survival and response rates in thyroid cancer patients, regardless of a specific genetic mutation.
Contribution
The study provides evidence that cabozantinib is effective in radioiodine-refractory thyroid cancer patients with or without the BRAFV600E mutation.
Findings
Cabozantinib improved progression-free survival in both BRAF wild-type and BRAFV600E subgroups.
Objective response rates were observed with cabozantinib but not with placebo in both subgroups.
Adverse events were more common with cabozantinib but manageable.
Abstract
Cabozantinib is approved for previously treated radioiodine-refractory differentiated thyroid cancer (RAIR-DTC) based on improved progression-free survival (PFS) versus placebo in the COSMIC-311 study. The BRAFV600E mutation is common in DTC and is associated with poor prognosis. This planned exploratory analysis of COSMIC-311 reports outcomes by BRAF status. In this exploratory analysis, outcomes by BRAFwt (wild-type) or BRAFV600E status were evaluated in the COSMIC-311 phase 3 study in patients with RAIR-DTC who had previously received lenvatinib and/or sorafenib. BRAF status was available for 106 of 258 patients enrolled in COSMIC-311; of these, 74 had BRAFwt and 27 had BRAFV600E. Cabozantinib prolonged PFS versus placebo in both the BRAFwt (hazard ratio [HR] 0.23 [95% CI: 0.12–0.44]; median PFS, 11.1 versus 1.9 months) and BRAFV600E (HR 0.15 [95% CI: 0.04–0.59]; median PFS, 9.2…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
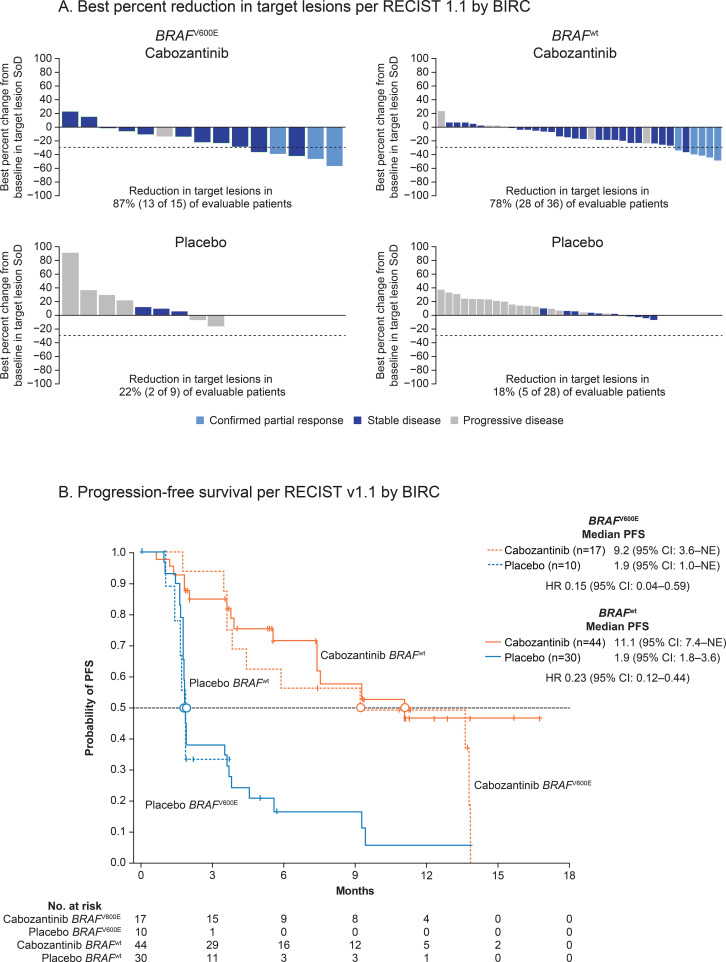 Figure 1
Figure 1| Characteristic |
|
| ||
|---|---|---|---|---|
| Cabozantinib (n = 17) | Placebo (n = 10) | Cabozantinib (n = 44) | Placebo (n = 30) | |
| Age, median (range), y | 70.0 (54–82) | 62.0 (47–78) | 66.0 (31–79) | 65.5 (51–79) |
| ≥65 y, n (%) | 12 (71) | 4 (40) | 25 (57) | 17 (57) |
| Female, n (%) | 11 (65) | 5 (50) | 27 (61) | 15 (50) |
| Race, n (%) | ||||
| White | 12 (71) | 8 (80) | 41 (93) | 21 (70) |
| Asian | 3 (18) | 2 (20) | 2 (5) | 5 (17) |
| Black | 0 | 0 | 0 | 1 (3) |
| Other/unknown | 2 (12) | 0 | 1 (2) | 3 (10) |
| Geographic region, n (%) | ||||
| Europe | 8 (47) | 2 (20) | 28 (64) | 15 (50) |
| Asia | 2 (12) | 2 (20) | 1 (2) | 4 (13) |
| United States/Canada | 3 (18) | 2 (20) | 4 (9) | 8 (27) |
| Rest of the world | 4 (24) | 4 (40) | 11 (25) | 3 (10) |
| ECOG performance status, n (%) | ||||
| 0 | 8 (47) | 6 (60) | 21 (48) | 15 (50) |
| 1 | 9 (53) | 4 (40) | 23 (52) | 15 (50) |
| Histological subtype, n (%) | ||||
| Papillary | 17 (100) | 10 (100) | 17 (39) | 14 (47) |
| Follicular | 0 | 0 | 27 (61) | 16 (53) |
| Number of previous VEGFR-TKIs, n (%) | ||||
| 1 | 14 (82) | 9 (90) | 32 (73) | 20 (67) |
| 2 | 3 (18) | 1 (10) | 12 (27) | 10 (33) |
| Metastatic lesions, n (%) | ||||
| Bone | 6 (35) | 3 (30) | 23 (52) | 14 (47) |
| Liver | 2 (12) | 0 | 13 (30) | 3 (10) |
| Lungs | 13 (76) | 9 (90) | 35 (80) | 20 (67) |
| Other | 17 (100) | 7 (70) | 36 (82) | 27 (90) |
| Tumor response |
|
| ||
|---|---|---|---|---|
| Cabozantinib (n = 17) | Placebo (n = 10) | Cabozantinib (n = 44) | Placebo (n = 30) | |
| ORR, % (95% CI) | 18 (3.8–43.4) | 0 (0.0–30.8) | 11 (3.8–24.6) | 0 (0.0–11.6) |
| Best overall response, n (%) | ||||
| Complete response | 0 | 0 | 0 | 0 |
| Partial response | 3 (18) | 0 | 5 (11) | 0 |
| Stable disease | 12 (71) | 3 (30) | 28 (64) | 10 (33) |
| ≥16 wk | 8 (47) | 1 (10) | 18 (41) | 6 (20) |
| Progressive disease | 1 (6) | 6 (60) | 5 (11) | 19 (63) |
| No measurable disease | 0 | 0 | 1 (2) | 0 |
| Missing/not evaluable | 1 (6) | 1 (10) | 5 (11) | 1 (3) |
| Median duration of response (95% CI), months | 10.22 (NE–NE) | NE | NE (9.33–NE) | NE |
| DCR (CR+PR+SD), % (95% CI) | 88 (63.6–98.5) | 30 (6.7–65.2) | 75 (59.7–86.8) | 33 (17.3–52.8) |
| DSR (CR+PR+SD ≥16 wk), % (95% CI) | 65 (38.3–85.8) | 10 (0.3–44.5) | 52 (36.7–67.5) | 20 (7.7–38.6) |
| Event |
|
| ||||||
|---|---|---|---|---|---|---|---|---|
| Cabozantinib (n = 17) | Placebo (n = 10) | Cabozantinib (n = 44) | Placebo (n = 30) | |||||
| Any Gr | Gr 3/4 | Any Gr | Gr 3/4 | Any Gr | Gr 3/4 | Any Gr | Gr 3/4 | |
| Any event, n (%) | 17 (100) | 9 (53) | 9 (90) | 5 (50) | 44 (100) | 30 (68) | 26 (87) | 5 (17) |
| Diarrhea | 9 (53) | 2 (12) | 0 | 0 | 32 (73) | 1 (2) | 2 (7) | 0 |
| Palmar-plantar erythrodysesthesia | 10 (59) | 4 (24) | 0 | 0 | 20 (45) | 4 (9) | 0 | 0 |
| ALT increased | 9 (53) | 1 (6) | 1 (10) | 1 (10) | 11 (25) | 0 | 0 | 0 |
| AST increased | 9 (53) | 0 | 0 | 0 | 9 (20) | 0 | 1 (3) | 0 |
| Decreased appetite | 5 (29) | 1 (6) | 1 (10) | 0 | 13 (30) | 0 | 5 (17) | 0 |
| Hypertension | 9 (53) | 3 (18) | 1 (10) | 1 (10) | 11 (25) | 5 (11) | 1 (3) | 1 (3) |
| Hypocalcemia | 6 (35) | 3 (18) | 2 (20) | 2 (20) | 16 (36) | 5 (11) | 0 | 0 |
| Weight decreased | 4 (24) | 0 | 0 | 0 | 11 (25) | 2 (4) | 1 (3) | 0 |
| Nausea | 2 (12) | 0 | 0 | 0 | 19 (43) | 1 (2) | 1 (3) | 0 |
| Stomatitis | 1 (6) | 0 | 0 | 0 | 6 (14) | 1 (2) | 0 | 0 |
| Asthenia | 3 (18) | 1 (6) | 0 | 0 | 7 (16) | 1 (2) | 5 (17) | 0 |
| Fatigue | 9 (53) | 0 | 0 | 0 | 15 (34) | 5 (11) | 4 (13) | 0 |
| Mucosal inflammation | 3 (18) | 0 | 0 | 0 | 7 (16) | 1 (2) | 0 | 0 |
| Vomiting | 3 (18) | 0 | 0 | 0 | 7 (16) | 1 (2) | 4 (13) | 0 |
| Hypomagnesemia | 3 (18) | 0 | 0 | 0 | 9 (20) | 0 | 0 | 0 |
| Proteinuria | 5 (29) | 0 | 0 | 0 | 6 (14) | 3 (7) | 1 (3) | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Thyroid Disorders and Treatments · Cancer, Lipids, and Metabolism
Introduction
The prognosis for patients with differentiated thyroid cancer (DTC) is generally favorable (1). Treatment options include active surveillance, surgery, and radioiodine (RAI) therapy. However, up to 15% of patients can develop RAI-refractory DTC (RAIR-DTC) that has less favorable outcomes and requires more aggressive management (2, 3). Genetic mutations or rearrangements as well as signaling pathway dysregulation are shown to drive the evolution of RAIR-DTC (3). For example, activating mutations of B-type raf kinase (BRAF), neurotrophin receptor tyrosine kinase (NTRK), or receptor tyrosine kinase rearranged during transfection (RET), have been associated with poor prognosis in patients (3).
First-line treatment options for RAIR-DTC, in the absence of NTRK or RET fusion, are the vascular endothelial growth factor receptor (VEGFR)-targeted tyrosine kinase inhibitors (TKIs) lenvatinib or sorafenib (4, 5). However, most patients eventually develop treatment resistance and experience disease progression. Until recently, no treatment options were available for patients experiencing disease progression after VEGFR-targeted therapy (6).
Cabozantinib, a multitargeted TKI, has been approved for previously treated patients with RAIR-DTC (7). In the United States, cabozantinib is indicated for patients aged ≥12 years who progressed after VEGFR-targeted therapy (7). In the EU, it is approved for adults who progressed after systemic therapy (8). These approvals were based on the findings of the phase 3 COSMIC-311 clinical trial (NCT03690388) in which cabozantinib significantly prolonged progression-free survival (PFS) and increased objective response rate (ORR) compared with placebo, with a manageable safety profile, in previously treated patients with RAIR-DTC (6). This clinical benefit was maintained during the extended follow-up period (median, 10.1 months) with no new safety signals (9, 10). Cabozantinib inhibits tyrosine kinases VEGFR, AXL, and MET, which are known to mediate tumor growth and angiogenesis in DTC (11). MET and AXL also promote resistance to VEGFR-pathway inhibition (12–14). Thus, the observed clinical benefits of cabozantinib in DTC previously treated with VEGFR-targeted therapies such as lenvatinib or sorafenib may result from cabozantinib targeting pathways associated with resistance.
The BRAF^V600E^ pathogenic variant is a constitutively active form of the BRAF kinase that drives disease evolution in multiple tumor types including DTC (15). Although there are other BRAF mutations, BRAF^V600E^ is the most common, occurring in 30–90% of DTCs, with the higher prevalences occurring in papillary or papillary-follicular histological subtypes (16–20). BRAF^V600E^ is the most common genetic change in RAIR-DTC, where it drives dedifferentiation and impairs expression and trafficking of proteins needed for iodine uptake (3, 15). BRAF^V600E^ is associated with aggressive tumor phenotypes, reduced response to RAI, and worse prognosis in RAIR-DTC (16–21).
Cabozantinib is approved for patients with RAIR-DTC whose disease has progressed after prior VEGFR-targeted therapy (22). As the BRAF^V600E^ mutation is prevalent and pathogenically important in RAIR-DTC, we explored the impact of BRAF status on cabozantinib outcomes in RAIR-DTC in a planned exploratory analysis of COSMIC-311 trial data.
Methods
Design, ethics, eligibility criteria, stratification, randomization, treatment, assessments, and outcome measures of the COSMIC-311 randomized, double-blind, placebo-controlled phase 3 trial have been published previously (6). In brief, patients with RAIR-DTC ≥16 years of age previously treated with lenvatinib or sorafenib, never exposed to selective BRAF small-molecule inhibitors, and experiencing disease progression were randomized 2:1 to receive oral cabozantinib 60 mg/day or placebo. A blinded independent radiology committee (BIRC) adjudicated ORR and PFS as co-primary endpoints and determined best percent reduction in target lesion size according to Response Evaluation Criteria in Solid Tumors (RECIST) v1.1 as in the primary publication (6, 23). Other endpoints included disease control rate (DCR), the total proportion of patients who achieved a confirmed complete or partial response or stable disease (SD) at any time, and disease stabilization rate (DSR), the proportion of patients achieving a confirmed complete response, partial response, or SD lasting ≥16 weeks (6).
Tumor biopsy at the time of enrollment was optional. Tumor tissue (fresh or archival) from the most recently collected sample prior to enrollment was obtained for biomarker analysis. BRAF status was determined centrally for patients with available tissue via whole exome sequencing from formalin-fixed paraffin-embedded tumor tissue and paired blood samples. Somatic variants were determined using the variant caller VarDict (24).
The current exploratory subgroup analysis evaluated ORR and PFS in patients randomized to cabozantinib versus placebo by BRAF^wt^ (wild-type) or BRAF^V600E^ status. Best reduction in target lesion size per BIRC was visualized as waterfall plots. Kaplan-Meier curves were drawn for PFS and median PFS times estimated using the Kaplan-Meier method, hazard ratio (HR) for BIRC-adjudicated PFS was determined by a Cox proportional hazards model, and BIRC-adjudicated ORR was compared using an unstratified two-sided Fisher’s exact test (6).
Results
Among 258 patients randomized into the COSMIC-311 trial, BRAF status was available for 106. Of these, 74 were BRAF^wt^ and 27 had the BRAF^V600E^ pathogenic variant. Of the 74 patients with BRAF^wt^, 44 were in the cabozantinib arm and 30 were in the placebo arm, and of the 27 patients with BRAF^V600E^, 17 were in the cabozantinib arm and 10 were in the placebo arm. Patients with BRAF^wt^ had papillary or follicular histology; papillary tumor histology was universal among patients with BRAF^V600E^ (Table 1). Baseline demographic and clinical characteristics are shown in Table 1 and were consistent with those previously reported for the overall population of the COSMIC-311 trial (9).
Clinical responses to cabozantinib were observed irrespective of patients’ BRAF status (Table 2). The ORR was 11% (95% CI: 3.8%–24.6%) and 18% (95% CI: 3.8%–43.4%) in the BRAF^wt^ and BRAF^V600E^ groups, respectively; all were partial responses. Patients randomized to placebo did not exhibit any responses irrespective of BRAF status. DCR and DSR were higher with cabozantinib than placebo irrespective of BRAF status. The DCR observed with cabozantinib was 75% in the BRAF^wt^ group and 88% in the BRAF^V600E^ group, contrasting with placebo DCRs of 33% in the BRAF^wt^ group and 30% in the BRAF^V600E^ group. DSR in patients in the cabozantinib arm were 52% and 65% in the BRAF^wt^ and BRAF^V600E^ groups, respectively, compared with 20% and 10% in the corresponding groups in the placebo arm.
Cabozantinib also reduced target lesions in a higher percentage of evaluable patients than placebo irrespective of BRAF status. In the cabozantinib arm, 78% and 87% of patients with BRAF^wt^ and BRAF^V600E^, respectively, exhibited target lesion reductions compared with 18% and 22% in the corresponding groups in the placebo arm (Figure 1A).
(A) Best percent reduction in target lesions per RECIST v1.1 by BIRC. Included only evaluable patients who had baseline and at least one post-baseline tumor assessment. (B) Progression-free survival per RECIST v1.1 by BIRC. BIRC, blinded independent radiology committee; BRAF, B-type raf kinase; CI, confidence interval; HR, hazard ratio; NE, not estimable; PFS, progression-free survival; RECIST, Response Evaluation Criteria in Solid Tumors; SoD, sum of diameters; wt, wild type.
Cabozantinib was associated with prolonged PFS versus placebo irrespective of BRAF status. Among patients with BRAF^wt^, median PFS was 11.1 months in the cabozantinib arm versus 1.9 months in the placebo arm (HR 0.23 [95% CI: 0.12–0.44]). Among patients with BRAF^V600E^, median PFS was 9.2 months in the cabozantinib arm versus 1.9 months in patients in the placebo arm (HR 0.15 [95% CI: 0.04–0.59]; Figure 1B).
The safety profile of cabozantinib in both BRAF status groups was consistent with that seen in earlier reports of the overall population (6, 9). Among patients treated with cabozantinib, 68% of the BRAF^wt^ group and 53% of the BRAF^V600E^ group reported grade 3/4 treatment-emergent adverse events (TEAEs); the incidences were 17% and 50% in the corresponding groups treated with placebo. The most common grade 3/4 TEAEs in patients treated with cabozantinib (BRAF^wt^ and BRAF^V600E^ subgroups, respectively) were palmar-plantar erythrodysesthesia (9% and 24%), hypertension (11% and 18%), and hypocalcemia (11% and 18%) (Table 3). The most common grade 3/4 TEAEs in corresponding groups of patients treated with placebo were hypocalcemia (0% and 20%), hypertension (3% and 10%), and increased alanine aminotransferase (0% and 10%).
Discussion
In this planned exploratory subgroup analysis of COSMIC-311, treatment with cabozantinib improved efficacy outcomes versus placebo irrespective of BRAF status. The ORR in the cabozantinib arm was 11% in the BRAF^wt^ group and 18% in the BRAF^V600E^ group, contrasting with 0% in both groups in the placebo arm, with substantially higher DCR and DSR among patients treated with cabozantinib. Cabozantinib prolonged median PFS to 11.1 months in the BRAF^wt^ group and 9.2 months in the BRAF^V600E^ group, contrasting with 1.9 months in both corresponding groups assigned to placebo. Thus, the co-primary outcomes of COSMIC-311 showed efficacy across BRAF subgroups at a comparable magnitude to the full study population (ORR: cabozantinib 11%, placebo 0%; median PFS: 11.0 months with cabozantinib, 1.9 months with placebo) (9). These findings are particularly important since the BRAF^V600E^ variant has been associated with poor prognosis, tumor aggressiveness, persistence, recurrence, and short survival in DTC (3).
A combination of dabrafenib (BRAF inhibitor) and trametinib (MEK inhibitor) currently has a tumor agnostic approval in the United States for patients with BRAF^V600E^ mutations, including anaplastic thyroid cancer but not specifically for RAIR-DTC, based on efficacy in the phase 2 ROAR and NCI-MATCH basket studies (25–27). The first prospective clinical trials with vemurafenib or dabrafenib provided evidence of activity of BRAF inhibitors in patients with RAIR-DTC and BRAF pathogenic variants (28, 29). Objective responses were generally higher in TKI-naïve patients compared with previously TKI-treated patients, but comparisons are limited due to small sample size and the variability and number of prior therapies. A more recent phase 2 trial of dabrafenib or dabrafenib plus trametinib in BRAF-mutated RAIR-DTC confirmed similar activity between single-agent BRAF therapy and combination BRAF plus MEK therapy in predominantly TKI-naïve patients (30). A global phase 3 study is ongoing to evaluate dabrafenib in combination with trametinib versus placebo in TKI-refractory BRAF^V600E^ RAIR-DTC (NCT04940052), which may provide evidence for utilizing BRAF and MEK*-*targeted therapy in TKI-exhausted RAIR-DTC patients. While these studies provide evidence of activity for the BRAF plus MEK inhibitor combination in BRAF-altered RAIR-DTC, the safety and efficacy of BRAF-targeted therapies have not been directly compared to TKIs (25–27). In the absence of randomized trials comparing BRAF-targeted agents to VEGFR-TKIs in BRAF^V600E^ RAIR-DTC, relative safety and efficacy of these agents, as well as the optimal sequencing of these treatment options remains unknown. To this end, a randomized phase 3 ECOG-ACRIN study EA3231 (NCT06475989) has been initiated to compare cabozantinib versus dabrafenib plus trametinib in patients with BRAF^V600E^ RAIR-DTC who have progressed on one or two prior VEGFR-TKI therapies. Results of this study will provide insight into the relative benefit of maintaining VEGFR inhibition after progressing on initial VEGFR-TKI therapy versus switching to BRAF and MEK inhibition. Further studies are needed to inform the appropriate sequencing of TKI and BRAF plus MEK inhibitors, with the goal of maximizing activity and safety of each therapeutic agent across the patient treatment journey.
TEAEs reported by patients in both BRAF status groups treated with cabozantinib were comparable, manageable, and consistent with observations in the full safety population of COSMIC-311 (6, 9), in which the most common grade 3/4 TEAEs were palmar-plantar erythrodysesthesia, hypertension, fatigue, diarrhea, and hypocalcemia. Although over half of patients required dose reductions due to adverse events (AEs), <10% discontinued treatment due to AEs unrelated to DTC, supporting the appropriate management of TEAEs is through proactive AE management and dose modifications (6, 9).
Limitations of this subgroup analysis include its exploratory nature and a relatively small subgroup size that may introduce biases. The results are to be considered hypothesis-generating because subgroups were not powered to show differences between treatment arms. Our observations nevertheless may have clinical implications for cabozantinib treatment of RAIR-DTC, in which BRAF^V600E^ is prevalent.
In conclusion, this subgroup analysis of the COSMIC-311 phase 3 trial showed that treatment with cabozantinib improved clinical outcomes, including a prolonged PFS and higher ORR, compared with placebo in patients with either BRAF^wt^ or BRAF^V600E^. The magnitude of clinical outcomes was similar to that seen in the intention-to-treat population regardless of the BRAF mutational status. The observed efficacy along with a manageable safety profile further supports cabozantinib as an efficacious treatment following VEGFR-targeted therapy in patients with RAIR-DTC including those with BRAF^V600E^ mutations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Cancer Institute . Cancer stat facts: Thyroid cancer. Bethesda, MD, USA: National Institutes of Health (2025). Available online at: https://seer.cancer.gov/statfacts/html/thyro.html (Accessed April 24, 2025).
- 2Lirov R Worden FP Cohen MS . The treatment of advanced thyroid cancer in the age of novel targeted therapies. Drugs. (2017) 77:733–45. doi: 10.1007/s 40265-017-0733-1, PMID: 28361210 PMC 5683961 · doi ↗ · pubmed ↗
- 3Shen H Zhu R Liu Y Hong Y Ge J Xuan J . Radioiodine-refractory differentiated thyroid cancer: molecular mechanisms and therapeutic strategies for radioiodine resistance. Drug Resist Updat. (2024) 72:101013. doi: 10.1016/j.drup.2023.101013, PMID: 38041877 · doi ↗ · pubmed ↗
- 4Fugazzola L Elisei R Fuhrer D Jarzab B Leboulleux S Newbold K . 2019 European thyroid association guidelines for the treatment and follow-Up of advanced radioiodine-Refractory thyroid cancer. Eur Thyroid J. (2019) 8:227–45. doi: 10.1159/000502229, PMID: 31768334 PMC 6873012 · doi ↗ · pubmed ↗
- 5Haugen BR Alexander EK Bible KC Doherty GM Mandel SJ Nikiforov YE . 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the american thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. (2016) 26:1–133. doi: 10.1089/thy.2015.0020, PMID: 26462967 PMC 4739132 · doi ↗ · pubmed ↗
- 6Brose MS Robinson B Sherman SI Krajewska J Lin CC Vaisman F . Cabozantinib for radioiodine-refractory differentiated thyroid cancer (COSMIC-311): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. (2021) 22:1126–38. doi: 10.1016/S 1470-2045(21)00332-6, PMID: 34237250 · doi ↗ · pubmed ↗
- 7United States Food and Drug Administration . CABOMETYX® (cabozantinib) tablets, for oral use, revised 10/2025. (2025). Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/208692 s 019lbl.pdf (Accessed February 2, 2026).
- 8European Medicines Agency . Cabometyx®, INN-cabozantib Summary of Product Characteristics, last updated October 28, 2025 (2025). Available online at: https://www.ema.europa.eu/en/documents/product-information/cabometyx-epar-product-information_en.pdf (Accessed February 2, 2026).