Noncommunicable chronic diseases and health challenges in 2050
Deborah Carvalho Malta, Guilherme Augusto Veloso, Crizian Saar Gomes, Maurício Lima Barreto, Deborah Carvalho Malta, Guilherme Augusto Veloso, Crizian Saar Gomes, Maurício Lima Barreto

TL;DR
This study projects that noncommunicable diseases will shift in focus by 2050, with cancer overtaking heart disease as the top cause of death.
Contribution
The study provides new projections of NCD trends and risk factors in Brazil up to 2050, highlighting policy implications.
Findings
Premature NCD mortality in Brazil dropped by 37.7% from 1990 to 2021.
Cardiovascular disease is projected to be overtaken by cancer as the leading cause of death by 2050.
Rising risk factors like obesity and poor diet may hinder global NCD reduction targets.
Abstract
The study aims to analyze the burden of diseases related to noncommunicable chronic diseases (NCDs) and their risk factors (RFs) from 1990 to 2021 and to project of NCDs and RFs for the years 2030 and 2050. Estimates of risk factors and mortality from NCDs in Brazil and its States were analyzed based on data from the Global Burden of Disease Study. There was a 37.7% reduction in premature mortality rates from NCDs and a 34% reduction in Disability-Adjusted Life Years (DALYs) between 1990 and 2021. Projections for 2050 indicate that mortality from cardiovascular diseases will continue to decline and that these will be supplanted by neoplasms. Mortality rates from diabetes tend to increase, while chronic respiratory diseases show a downward trend. In 2021, the main risk factors associated with premature deaths from NCDs were: high blood pressure, smoking, poor diet, high Body Mass Index…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
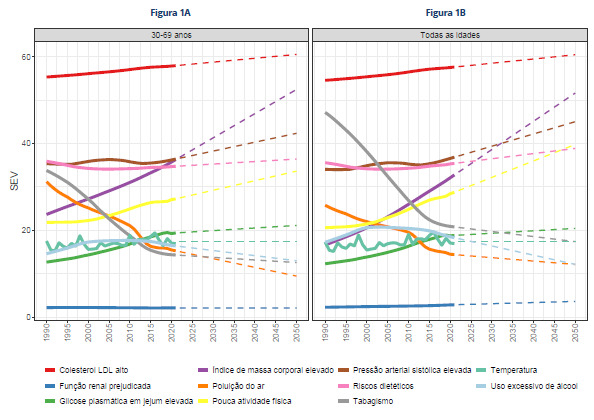 Figure 1
Figure 1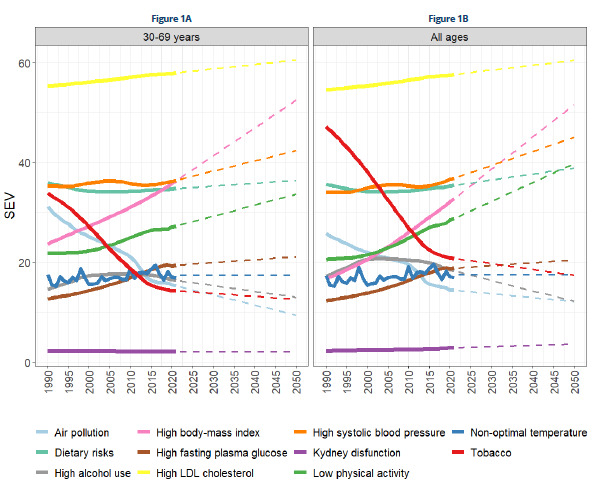 Figure 2
Figure 2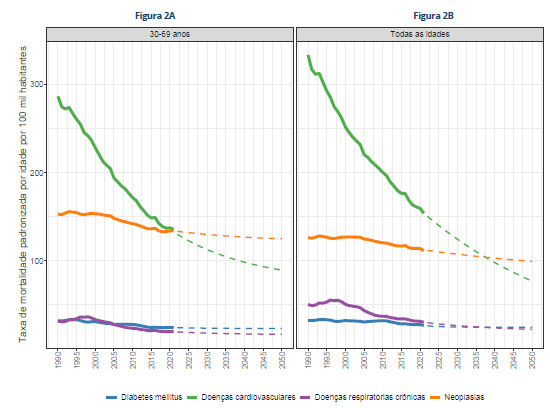 Figure 3
Figure 3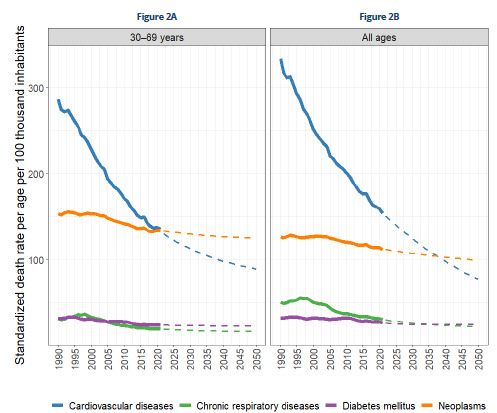 Figure 4
Figure 4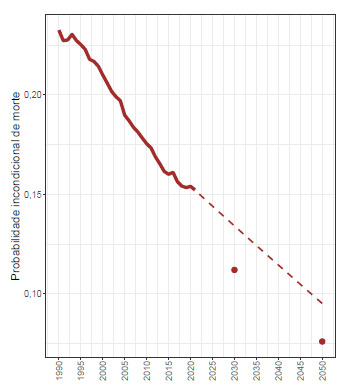 Figure 5
Figure 5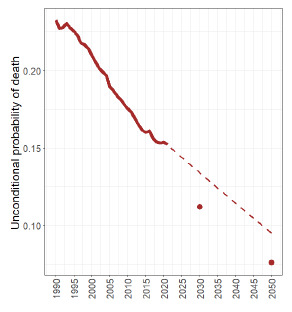 Figure 6
Figure 6- —FAPEMIG 011/2022 - “SUPPORT FOR EXTENSION PROJECTS IN INTERFACE WITH RESEARCH” PROCESS
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Public Health Policies and Epidemiology · Cardiovascular Health and Risk Factors · Chronic Disease Management Strategies
INTRODUCTION
Noncommunicable chronic diseases (NCDs) are the leading cause of global morbidity and mortality, resulting in premature deaths, disabilities, loss of quality of life, economic impacts, and burden on health systems1 ^,^ 2. NCDs are estimated to account for 75% of global mortality3 .
The four main groups of NCDs - cardiovascular diseases (CVD), cancer, chronic respiratory diseases, and diabetes - share common and modifiable behavioral risk factors (RF), such as smoking, alcohol abuse, physical inactivity, and poor diet4 ^,^ 5. In addition to these, metabolic factors such as high blood pressure, obesity, high cholesterol, and high fasting plasm glucose also stand out2 ^,^ 5 ^,^ 6. Socioeconomic determinants play a strong role in the causality network of NCDs and their RF1 ^,^ 7 ^,^ 8.
The 2030 Agenda for Sustainable Development established a goal of reducing the “unconditional probability of premature death from NCDs” by one-third9. To date, only 19 countries - representing only 2.7% of the world’s population - are on track to achieve this goal. At the current pace, it would take approximately 45 years to achieve this goal10.
In Brazil, studies indicate that mortality rates from NCDs showed a downward trend between 2010 and 2015. However, this progress was interrupted in 2016 and worsened during the COVID-19 pandemic, compromising the possibility of achieving the 30% reduction target set by Plano de DANT, a Brazilian strategic action plan to tackle CNCDs2 ^,^ 11 ^,^ 12 ^,^ 13 .
In the face of persistent global challenges, new commitments have been proposed. In 2024, the Lancet Commission launched the goal of reducing the probability of premature death from selected diseases by 50% by 2050 - a proposal that became known as “50 by 50.” This goal can be achieved by addressing 15 priority conditions - 8 related to infectious diseases and maternal health, and 7 related to NCDs and injuries14.
The main proposals for achieving the 2050 targets would be
- a) concentrating resources on priority conditions, including NCDs, with a view to maximizing the impact on reducing premature mortality;
- b) increasing global health funding;
- c) tobacco control as a priority strategy, with tax increases, marketing bans, and other measures;
- d) reducing poverty and social inequalities;
- e) improving access to primary care and essential medicines;
- f) promoting healthy eating, physical activity, and healthy environments.
In this context, the Brazil Saúde Amanhã initiative, launched by Fundação Oswaldo Cruz (Fiocruz), stands out. It is based on the guiding question: “What is the future of health in Brazil?”. The initiative coordinates a multidisciplinary research network focused on investigation, strategic prospecting, and the formulation of public policies for the health sector, strengthening the Unified Health System (SUS)15 ^,^ 16.
This study falls within this scope and has the following objectives: to analyze the burden of diseases related to NCDs and their RF in the period from 1990 to 2021; and to project the evolution of NCDs and RF for the years 2030 and 2050.
METHODS
This study analyzed estimates of RF and mortality from NCDs in Brazil and its States, based on data from the 2021 Global Burden of Disease (GBD) Study, from the Institute for Health Metrics and Evaluation (IHME), available at: http://ghdx.healthdata.org/.
Mortality
The GBD mortality estimates are based on data from the Mortality Information System (SIM) of the Ministry of Health17, with adjustments for so-called garbage codes, using algorithms for redistributing the underlying causes of death, considering age, sex, and year18 ^,^ 19.
The unconditional probabilities of premature death from NCDs were calculated. For each age group (𝑥 𝑥 +5), the probability of death during the interval was estimated based on the age-specific mortality rate, denoted by m _ x _ , using the approximation qx=5mx1+2,5mx. The unconditional probability of death was estimated as:
The metrics used to analyze the burden of NCDs in Brazil was: absolute number of deaths, age-standardized mortality rates, and years of life lost due to premature death and Disability-Adjusted Life Years (DALYs). These metrics were presented for all age groups and for premature deaths between 30 and 69 years of age, according to the World Health Organization (WHO) Global Plan1. The analyses covered all diseases and the four main groups of NCDs in Brazil in 1990 and 2021, as well as the percentage change (PC) over the period.
To verify subnational inequalities, premature mortality rates from NCDs were analyzed for the 26 Brazilian States and the Federal District in 1990 and 2021.
Risk factors
The main sources of data on RF for the Brazilian population used by the GBD were the National Health Survey (PNS), the Surveillance System for Risk and Protective Factors for Chronic Diseases (Vigitel), and the National School Health Survey (PeNSE)13 ^,^ 20.
The GBD study uses a hierarchical list of risk factors organized into four levels, ranging from broad groups (metabolic, behavioral, and environmental) to more detailed ones, totaling 87 factors analyzed in 202121.
Regarding RF, the Summary Exposure Value (SEV) was analyzed. The SEV represents the prevalence of exposure weighted by relative risk, ranging from 0% to 100%, in which 0% indicates a total absence of exposure and 100% corresponds to the maximum level of exposure observed in the population. A reduction in SEV indicates a decrease in population exposure to the risk factor, whereas an increase suggests the opposite. More information on SEV is available in other publications20 ^,^ 22.
Projections for 2050
Risk factors
SEV trends for risk factors related to NCDs between 1990 and 2021 were analyzed, including: smoking, poor diet, low physical activity, excessive alcohol consumption, high blood pressure, high cholesterol, impaired kidney function, high fasting blood glucose, high Body Mass Index (BMI), air pollution, and temperature. Based on the evolution observed during this period, projections for these indicators were calculated up to the year 2050.
Mortality projections
Projections were calculated for premature mortality rates and mortality rates at all ages by NCDs and their four main groups, as well as the probability of premature death for the years 2030 and 2050. These results were compared to the Sustainable Development Goals (SDGs) targets agreed upon in 2015, which estimate a 30% reduction in the unconditional probability of premature death from NCDs23. Projections were also made to compare with the target proposed by the Lancet Commission (50% reduction by 2050)14. The values observed from the years 2015 to 2021 were used as a reference for the projection calculations.
An ETS model was used. The term refers to the class of models that combine three fundamental components: Error (E), Trend (T), and Seasonality (S); of the type: Additive (A), Additive Trend (A), and No Seasonality (N) (AAN). This model is especially suitable for time series that exhibit a trend but do not show seasonal patterns. In addition, a dampened trend was used, which introduces a dampening factor to gradually reduce the influence of the trend on long-term projections.
The analyses were conducted in RStudio (RStudio Team, 2019) and the figures were produced using the ggplot214 package.
Ethical considerations
The GBD-Brazil project was approved by the Research Ethics Committee of Universidade Federal de Minas Gerais (UFMG), registered under Project number CAAE - 62803316.7.0000.5149.
Data availability statement
All data supporting the results of this study are available at: http://ghdx.healthdata.org
RESULTS
Mortality
Table 1 shows the mortality and DALY burden caused by NCDs in Brazil in 1990 and 2021. Premature mortality rates from all causes decreased by 7.1%. In the same period, there was a 37.7% reduction in premature mortality rates from NCDs and a 34% reduction in DALY rates. Between 1990 and 2021, premature mortality rates from CVD, chronic respiratory diseases, diabetes mellitus, and neoplasms decreased by 52.7%, 38.5%, 24%, and 12.5%, respectively. DALY rates showed similar reductions (Table 1).
Table 1.Number of deaths and standardized mortality and DALY rates in the population aged 30-69 years and in all ages, for both sexes, in Brazil, in 1990 and 2021.Cause of deathAge groupNumber of deathsStandardized mortality rate (per 100 thousand)Standardized DALYs rate (per 100 thousand)19902021PC 19902021PC 19902021PC Todas as causas30-69 years350,153804,109129.6792.1735.8-7.144,64742,524-4.8All ages875,7091,796,921105.2926.4742.9-19.843,05033,056-23.2NCD30-69 years212,908342,93061.1502.6312.9-37.718,10311,942-34All ages433,065788,37982542.2321.8-40.713,2618,500-35.9Diabetes mellitus30-69 years13,19126,28999.331.524-241,6561,627-1.7All ages26,31964,839146.432.126.5-17.51,1041,080-2.2Cardiovascular diseases30-69 years121,486148,70922.4286.7135.7-52.79,9624,902-50.8All ages258,237374,76545.1333.7153.7-53.97,4283,639-51Chronic respiratory diseases30-69 years12,92721,2026431.519.4-38.51,227792-35.4All ages36,88172,31696.150.330.1-40.21,371846-38.3Neoplasms30-69 years65,304146,731124.7153133.9-12.55,2584,620-12.1All ages111,628276,459147.7126.1111.4-11.63,3582,935-12.6PC: Percentage of change; CNCDs: Chronic noncommunicable diseases.
Table 2 shows the standardized rates of premature mortality from NCDs in both sexes for Brazil and its 27 federal units in 1990 and 2021. A reduction in mortality rates from NCDs, CVDs, and chronic respiratory diseases was observed in most states. The largest declines in CVD mortality rates were recorded in the Federal District (-72.9%) and Roraima (-72.1%). For diabetes and neoplasms, patterns varied across States. Mortality rates from neoplasms, for example, showed the largest reductions in Roraima (-52.3%) and the largest increase in Rio Grande do Norte (+35.6%), remaining relatively stable in most states.
Table 2.Standardized rates of premature mortality from chronic noncommunicable diseases and selected causes of death in Brazil and its federal units in 1990 and 2021.LocationNCDCardiovascular diseaseChronic respiratory diseaseDiabetesNeoplasms19902021PC19902021PC19902021PC19902021PC19902021PCBrazil502.6312.9-37.7286.6135.7-52.731.519.4-38.531.524-24153133.9-12.5Acre366.2303.2-17.2190.8123.5-35.330.927.5-11.12525.83.2119.4126.55.9Alagoas437.9358.5-18.1259.3180.9-30.333.218.5-44.23943.611.8106.5115.68.5Amapá397.6272.2-31.5206.5108.5-47.523.917.1-28.62324.67.1144.3122-15.4Amazon379309.9-18.2191.1112.8-4122.116.9-23.525.732.928.1140.1147.35.1Bahia381.6291.2-23.7220.3124.2-43.624.317.5-2833.527.8-16.9103.5121.717.6Ceará300.5268.4-10.7154.2118.6-23.121.612.5-42.118.316.7-9106.4120.713.4Federal District481.2187.4-61267.172.4-72.925.39.8-61.528.412.5-56160.292.8-42.1Espírito Santo482.7289.9-39.9288.1129.2-55.226.115.8-39.426.220.5-21.7142.2124.3-12.6Goiás456.5303.2-33.6260.4134.9-48.23823.3-38.62322.3-3.1135122.6-9.2Maranhão414.9357.5-13.8252.7174.3-3120.916.6-20.535.545.628.4105.812114.4Mato Grosso400.3279.4-30.2229.2120.1-47.623.821.2-1125.225.72.1122.2112.4-8Mato Grosso do Sul475.7302.9-36.3288.1139.9-51.427.119.3-2923.218.9-18.3137.2124.7-9.1Minas Gerais510.4292.9-42.6297.6120.3-59.634.318.7-45.63321.9-33.6145.5132.1-9.3Paraná562.7311-44.7327.5122.9-62.542.522.4-47.226.423-12.9166.4142.8-14.2Paraíba332.8337.61.4183.7155-15.620.116.5-17.629.534.617.599.6131.532Pará374.7304.6-18.7216.4135.3-37.52018.8-5.821.93246116.5118.51.7Pernambuco475.4339.7-28.5286.5159.9-44.224.427.512.739.228.9-26.2125.3123.4-1.5Piauí331.1275-16.9202.3133.1-34.218.711.6-37.62528.112.285.1102.220.1Rio Grande do Norte286295.73.4150.4130.2-13.512.711.2-11.430.629.2-4.692.3125.235.6Rio Grande do Sul565.4321.7-43.1283.5109-61.649.627.1-45.523.723.80.4208.6161.9-22.4Rio de Janeiro680.4367.2-46407.4168.7-58.633.919.2-43.446.330.6-33.9192.7148.7-22.9Rondônia431198.7-53.924984.2-66.22814.3-48.928.818.3-36.5125.381.9-34.6Roraima632.7229.8-63.7348.597.3-72.132.511.5-64.85426.8-50.3197.894.3-52.3Santa Catarina514.9291-43.5270.5108.1-604721.2-54.924.617.8-27.4172.8143.9-16.7Sergipe366.2279-23.8189.3119.9-36.721.115.9-24.740.630.6-24.5115.1112.6-2.2São Paulo556.9327.7-41.2316.5148.4-53.131.119.2-38.231.817.3-45.6177.6142.8-19.6Tocantins318.2268.1-15.8193.2128-33.823.215-35.622.128.529.179.796.621.2PC: Percentage of change; NCDs: noncommunicable chronic diseases.
Risk factors
Supplementary Table 1 shows the age-standardized SEV for RF related to NCDs in Brazil from 1990 to 2021. Between these years, the largest reductions in SEV for both sexes combined and all ages occurred for tobacco (-55.9%) and air pollution (-44.13%). In contrast, increases in SEV were observed for the following RFs: high BMI (+96.94%), high fasting blood glucose (+53.28%), and low physical activity (+39.68%). Similar results were found when analyzing the population aged 30 to 69 years.
Projections for 2030 and 2050
When analyzing SEV projections until 2050, it was observed that high LDL cholesterol, blood pressure, fasting glucose, BMI, low physical activity, risks related to diet/nutrition, temperature, and renal function show an upward trend between 30 and 69 years of age and across all ages. Smoking, although declining at the beginning of the series, tended to stabilize between the ages of 30 and 69. Excessive alcohol consumption and exposure to air pollution showed a downward trend (Figure 1).
Figure 1.Trends and projections of risk factors, according to the Summary Exposure Value*, for Chronic Noncommunicable Diseases from 1990 to 2021 and projections until 2050.*The Summary Exposure Value (SEV) was considered.
Figure 2 shows the trends and projections for mortality rates for the four main groups of CNCDs until 2050. Premature deaths from CVD continue to decline steadily and, from 2024/2025 onwards, these will be lower than those from neoplasms (the latter will reach the highest rates among all CNCDs in the coming decades). Mortality rates from chronic respiratory diseases and diabetes show more modest declines. When all age groups are considered, there will be declines in CVD, which remains in first place, followed by cancer and chronic respiratory diseases. In addition, there is an increase in diabetes rates, which will take the third place.
Figure 2.Trends in mortality rates for the four main groups of chronic noncommunicable diseases and projections for 2050, 1990-2021.
Figure 3 shows the trends in the probability of premature death from these diseases, with projections for 2030 and 2050. The global targets of reducing premature mortality from NCDs by 30% by 2030, based on data from 2015 to 2021, may not be achieved if the behavior observed during this period continues.
Figure 3.Mortality rates and probability of premature death from chronic noncommunicable diseases: trends (1990-2021) and projections (2030 and 2050), 1990-2021.
DISCUSSION
The study pointed to significant decline in mortality from NCDs between 1990 and 2021, reflecting improved overall living conditions, expanded access to health care - such as the expansion of primary care24 , income distribution programs25 ^,^ 26, access to medicines, and improvements in medium- and high-complexity care - as well as the reduction of RFs, such as the prevalence of smoking and increased physical activity4. The fundamental role of SUS, which contributed to the improvement of various health indicators and outcomes27, should also be highlighted.
However, this decline has not been continuous over time; in 2016 and 2021, there was an increase in mortality rates from NCDs. These are attributed to deepening socioeconomic inequalities, fiscal austerity policies, and underfunding of SUS5 ^,^ 28. The increase observed in 2021 was attributed to the effects of the COVID-19 pandemic, which resulted in both a worsening of the population’s lifestyles - with an increase in sedentary lifestyles and feelings of sadness and loneliness, as well as a deterioration in diet - and an increase in mortality, especially from cardiovascular diseases. This scenario can be explained, in part, by the interruption or reduction in clinical follow-up and monitoring of people with NCDs during the pandemic, in addition to the possible effects of long COVID-19, which may have contributed to the worsening of health conditions and increased mortality from NCDs in the post-pandemic period30 ^,^ 31.
The largest reductions in CVD mortality rates can be explained by several factors, including the expansion of primary health care; income distribution programs; the reduction in smoking prevalence; and improvements in care, both through increased access to primary care services13 and expanded access to medications for the control of high blood pressure32.
The study showed that cancer will become the leading cause of premature death from NCDs in Brazil within a few years, signaling the continuation of the epidemiological transition process in the country. Neoplasms are already the second leading cause of death in most countries21. In Uruguay and Argentina, cancer is the leading cause of death33. In Brazil, studies point to an increasing trend in the incidence of some types of cancer between 1990 and 2015, such as lung cancer in women (+20.7%) and colon and rectal cancer in men (+29.5%)34. This change reflects alterations in patterns of exposure to risk factors, therapeutic advances, and early screening and diagnosis systems35.
Diabetes is associated with increased mortality from cardiovascular diseases, with systemic effects that impact various organs and functions of the body23. There is consistent evidence that the growth in the prevalence of diabetes is strongly associated with the increase in obesity in the population23.
The significant reduction in mortality rates from chronic respiratory diseases can be attributed, in large part, to the decline in the prevalence of smoking4 ^,^ 36. Other factors that may have contributed to this trend include increased access to health services, especially with the expansion of Primary Health Care (PHC) in the country37.
According to the analysis by federal units, the patterns show some similarity between States. As for diabetes and neoplasms, there is a trend of increase or stabilization in most States. It is noteworthy that the States in the North and Northeast regions tend to show smaller reductions or even increases in rates, which may be related to worse living conditions, but also to possible limitations in the quality of information in mortality registration systems, especially in previous years13 ^,^ 38 ^,^ 39.
Risk factors
The results show a significant reduction in the main RFs, especially behavioral ones, with an emphasis on smoking. Evidence indicates that the control of risk factors and NCDs is more effective when regulatory measures are implemented by the State2 ^,^ 4 ^,^ 40 . In the case of tobacco, several regulatory actions have been adopted, such as accession to the Framework Convention on Tobacco Control (FCTC) in 2006; and Presidential Decree No. 8,262, of 2014, which expanded warnings on cigarette packs and regulated smoke-free environments and taxation on tobacco products4 ^,^ 13 . However, since 2016, the country has experienced a weakening of public policies to control smoking, with stagnation in pricing and taxation policies, as well as growing interference by the tobacco industry in the political and legal spheres, highlighting the influence of commercial determinants on health8 and resulting in poorer policy performance36 ^,^ 41 ^,^ 42.
Metabolic risk factors project high risks in the future, posing a threat to the health of the population in the coming years. In the last decade, Brazil has implemented important policies to strengthen PHC, such as the creation of the Mais Médicos (More Doctors) Program, expansion of free access to medicines for NCDs, health promotion actions, and income transfer programs6 ^,^ 32.
Obesity is a serious public health problem in Brazil, with a tendency to increase in prevalence among the adult population. It is estimated that approximately one-third of adults in Brazilian State capitals are obese and about 60% are overweight11. This rapid growth reinforces the need to expand access to obesity treatment; encourage regular physical activity; promote exclusive breastfeeding; and advance fiscal policies, such as increasing taxation on ultra-processed foods. These measures aim to strengthen access to healthy eating throughout life, in accordance with the guidelines of the Food Guide for the Brazilian Population.
Inadequate nutrition is projected to increase the SEV by 2050. Evidence shows an increase in ultra-processed foods and a reduction in the consumption of fresh foods, such as fruits, vegetables, and beans, as a result of changes in eating patterns, the economic crisis, and the adoption of austerity policies since 20165 ^,^ 44.
The “best evidence” indicated by the WHO for the prevention and control of NCDs includes regulatory and health promotion measures, such as taxation of beverages, tobacco, and ultra-processed foods, as well as a ban on the marketing of products harmful to health45. Therefore, they depend on investment in public policies and political decisions to advance the proposed agendas, including confronting the interests of industrial and commercial lobby45.
Projections for 2030 and 2050
The study indicates that projections of NCD mortality rates for 2030 and 2050 signal the possibility of failure to meet the established reduction targets. This scenario reinforces the need for continuous monitoring to identify possible changes in disease patterns, their determinants, and risk factors, and to adjust coping strategies in a timely manner over the coming years.
What are the global and national challenges to achieving the 2050 targets?
Investment in health promotion and NCD prevention actions can result in significant advances, provided there is political will and effective implementation of preventive measures10. A concrete example is the global reduction in smoking by about 25% in most countries since the adoption of the FCTC in 200710 ^,^ 46. In China, levels of fine particulate matter (PM2.5) in the air have been reduced by almost 50% in the last decade, demonstrating the effectiveness of strict environmental policies47.
In this context, the measures approved in Brazil regarding tax reform on tobacco and soft drinks represent a strategic opportunity to strengthen fiscal measures on products that are harmful to health, with a potential impact not only on mortality projections until 2050, but also on the sustainability of NCD prevention and control in the long term.
Study limitations
Among the limitations of the study, the projections for 2030 and 2050 were based on trends observed in previous years, assuming the continuity of past patterns as a parameter for the future. However, the future is uncertain and may include unpredictable events, as demonstrated by the COVID-19 pandemic. Incomplete data sources, such as the SIM, have made progress in coverage and improvement of record quality, although underreporting and a high proportion of garbage codes persist19. Additionally, social determinants are not directly incorporated into causal analyses48.
The study points out that global targets may not be achieved, raising an alert to the urgent need to strengthen public policies aimed at the prevention and control of CNCDs. It highlights the importance of intensifying intersectoral actions and strategies for health promotion, early diagnosis, timely access to treatment, and continuous monitoring - especially in the context of PHC.
Supplementary Materials
Table 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Global action plan for the prevention and control of noncommunicable diseases 2013-2020 Genebra World Health Organization 2013
- 2Malta DC Duncan BB Schmidt MI Teixeira R Ribeiro ALP Felisbino-Mendes MS Trends in mortality due to non-communicable diseases in the Brazilian adult population: national and subnational estimates and projections for 2030 Popul Health Metr 202018 Suppl 1161610.1186/s 12963-020-00216-132993685 PMC 7525955 · doi ↗ · pubmed ↗
- 3World Health Organization Commercial determinants of health Genebra World Health Organization 2023
- 4Malta DC Flor LS Machado IE Felisbino-Mendes MS Brant LCC Ribeiro ALP Trends in prevalence and mortality burden attributable to smoking, Brazil and federated units, 1990 and 2017 Popul Health Metr 202018 Suppl 1242410.1186/s 12963-020-00215-232993660 PMC 7526090 · doi ↗ · pubmed ↗
- 5Malta DC Duncan BB Barros AMB Katikireddi SV Souza FM Silva AG Medidas de austeridade fiscal comprometem metas de controle de doenças não transmissíveis no Brasil Ciênc Saúde Colet 201823103115312210.1590/1413-812320182310.2522201830365830 · doi ↗ · pubmed ↗
- 6Malta DC Gomes CS Stopa SR Andrade FMD Prates EJS Oliveira PPV Inequalities in health care and access to health services among adults with self-reported arterial hypertension: Brazilian National Health Survey Cad Saude Publica 202238 Suppl 1e 0012542110.1590/0102-311Xe 0012542135613254 · doi ↗ · pubmed ↗
- 7Pearce N Ebrahim S Mc Kee M Lamptey P Barreto ML Matheson D The road to 25×25: how can the five-target strategy reach its goal?Lancet Glob Health 201423 e 126e 12810.1016/S 2214-109X(14)70015-425102837 · doi ↗ · pubmed ↗
- 8Gilmore AB Fabbri A Baum F Bertscher A Bondy K Chang HJ Defining and conceptualising the commercial determinants of health Lancet 2023401103831194121310.1016/S 0140-6736(23)00013-236966782 · doi ↗ · pubmed ↗