Impact of Dobbs v. Jackson on Abortion Access in Colorado: An Analysis of Incidence and Demographic Shifts Post-Roe
Abigail Bryer, Thomas McAndrew, Fathima Wakeel, Christine Daley

TL;DR
This paper analyzes how the Dobbs v. Jackson ruling affected abortion access in Colorado, showing increased demand from out-of-state residents and later gestation abortions.
Contribution
The study is among the first to quantify the impact of the Dobbs decision on abortion access in a state with protective legislation.
Findings
Non-resident abortions increased in Colorado after the Dobbs decision.
The increase was driven by residents from surrounding states with restrictive abortion laws.
Abortion gestation times increased, suggesting delays in care access.
Abstract
To estimate the impact of the Dobbs v. Jackson decision on the number of incident abortions. We fit an interrupted time series model to annual incident abortions from 2004 to 2023 in the state of Colorado. In addition, we computed the proportion of residents that received abortive care from outside Colorado before and after the Dobbs v. Jackson decision. Finally, we estimated the proportion of abortions over time stratified by gestation week of the mother. We found that in the state of Colorado, after Dobbs v. Jackson (compared to before): (1) an increase in non-resident incident abortions immediately after the decision (2) which is driven by residents in the states surrounding Colorado with the most restrictive abortion laws. The uptick in non-resident abortions has likely led to longer wait times, a higher burden on facilities, and (3) later gestation times for the mother. Shifts…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
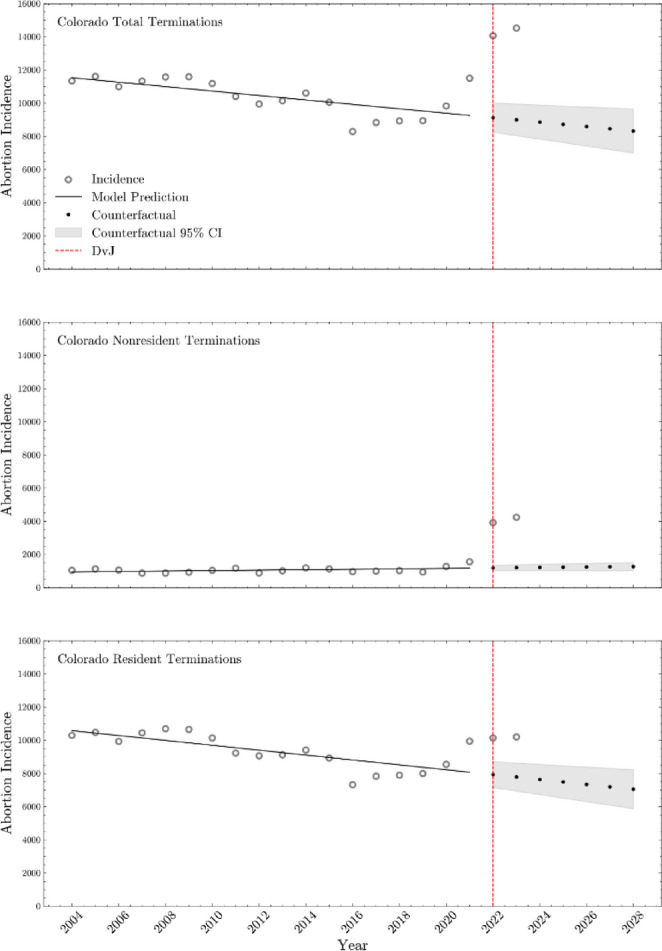 Figure 1
Figure 1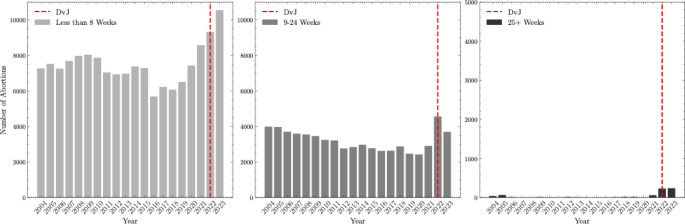 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Health and Contraception · Reproductive Health and Technologies · Legal Systems and Judicial Processes
Introduction
Dobbs v. Jackson (DvJ) was ratified on June 24, 2022, overturning Roe v Wade (RvW), which provided federal abortion protection in the United States from 1973 until 2022. The Dobbs decision returned the power to regulate abortion to individual states by ruling that the fourteenth amendment of the US constitution does not protect abortion as part of the constitutional right to privacy. Since the 1976 Hyde Amendment, federal funding of abortions has not been allowed; the three exceptions to this, life endangerment of the woman, rape, and incest, were approved in 1994 (Planned Parenthood Action Fund, n.d.). Based on the Dobbs decision, no federal funding of abortions can occur, regardless of the circumstances. Thus, states now have the power to determine public funding, regulate restrictions, or outright ban abortion care. At this time, 14 states have a total abortion ban and 27 have partial bans based on gestational duration. As the number of state-level abortion restrictions increase, it is estimated to cost those states without a ban more than 1.2 billion dedicated to Medicaid costs for unplanned births (Institute for Women’s Policy Research, 2021; Rodgers et al., 2021).
Preliminary evidence suggests unanticipated sequelae of Dobbs decision include increased maternal mortality, comorbidities associated with mortality, and adverse mental health effects (Kheyfets et al., 2023; Baden et al., 2024). It also disproportionately affects individuals with lower socioeconomic status. It is estimated that abortion bans across the country will result in an average increase of 21% in maternal mortality, with higher predicted mortality for racial and ethnic minorities (Kheyfets et al., 2023). Women denied abortion are more likely to experience gestational hypertension, which has the potential to lead to eclampsia (Foster, 2020). Gestational hypertension has also been found to be associated with higher likelihood of recurrence in subsequent pregnancies (Foster, 2020). In addition to bodily harm, women denied abortion are more likely to suffer from anxiety, depression, and low self-esteem in the short-term period after being denied care (Foster, 2020). Compared to women who are able to access abortion care, women who cannot access abortion have a 4 times greater odds of living below the Federal Poverty Level (Foster, 2020).
In addition to the health burdens on the individual, clinics that serve women and public health services have experienced higher abortion incidence for non-resident patients, longer appointment waiting times, extended hours, and more anti-abortion sentiment (Ungar, 2023; National Abortion Federation, 2023). The immediate effects of DvJ resulted in longer wait times (up to three weeks) in states that protect the right to abortion and are adjacent to states that have banned abortion (Sanger-Katz et al., 2022). Since the initial peak in the months following June 24, 2022, wait times for abortion have declined but still remain longer than when RvW was in place (Ungar, 2023). Abortion facilities are (1) at risk of being overwhelmed by appointment demand and unable to treat all patients, as well as (2) being subject to more frequent anti-abortion violence. Abortion clinics in 2022 saw increases in bomb threats by 133%, obstructions of clinic entrances by 538%, assault and batteries by 29%, and burglaries by 100% (National Abortion Federation, 2023). The delays experienced in abortion facilities have created an estimated demand for 4,300–16,500 late term abortions nationwide (Root et al., 2023).
In this study, we hypothesized that states that have protected the right to an abortion have experienced higher volumes of abortion incidence compared to average annual rates since DvJ , and that this influx was driven by non-resident patients. We used data from Colorado to support this claim, showing the observed changes in total and non-resident incidence in recent years. This work shows the immediate impact of health legislation and begins to address our limited understanding of the effects DvJ has on states with protective legislation.
Methods
Data Collection
We collected state level numbers of abortions performed at health care facilities for Colorado from 2004 to 2023 via the Colorado Department of Public Health and Environment (CDPHE). The CDPHE mandates abortion reporting to the state and collects counts at a yearly and monthly cadence. Abortion reports are inclusive of terminations occurring at physician clinics and hospitals. De-identified data were collected from the CDPHE via a data request form and the Lehigh University Human Subjects Committee determined that no Institutional Review Board approval was necessary for this study.
The following demographic data about women were available: race/ethnicity (collapsed into White non-Hispanic, White Hispanic, Black, other, and not stated), gestation week at time of termination (Less than or equal to 8 weeks, 9 to 24 weeks, 25 or more weeks), age (< 15, 15–19, 20–24, 25–29, 30–34, 35+), “Resident” or “Non-resident” status, marital status, and type of procedure (medical nonsurgical, suction curettage, dilation and evacuation, or other). We appended a binary indicator variable that takes the value 0 before the DvJ decision and the value 1 on and after DvJ. From 2020 to 2023, the CDPHE collected and reported the state of residence for each non-resident abortion patient in Colorado. The provided data did not include states with < 4 residents who traveled for abortion.
Data from 2004 to 2024 were provided and incorporated into analyses when available. In certain analyses, data beginning in 2004 were used to illustrate longitudinal trends in abortion incidence in Colorado.
Analysis
Continuous variables were summarized with means and standard deviations. Categorical variables were summarized with frequencies and percents. The estimated mean incident number of abortions before and after DvJ was assessed with a two-sample Student’s t-test. The chi-square test was used to test for an association between categorical variables. A p-value smaller than 0.05 was considered statistically significant.
We fit an Interrupted Time Series (ITS) model to evaluate the change in abortion incidence due to DvJ, stratified by total, non-resident, and resident abortions. Our model assumes the expected number of abortions (E(Y)) depends on the elapsed number of years since 2004 (T), an indicator variable that equals 1 on and after DvJ and equals 0 before this event (D), and the elapsed number of months after the DvJ decision (P); E(Y) = (b0 + b2D) + (b1T + b3P), where bx are model parameters. We assume residuals are Normally distributed and fit this model using ordinary least squares regression.
To explore the difference in the number of abortions from patients outside Colorado, we generated choropleth maps. Evidence for an association between changes in the number of abortions from non-resident patients from 2020 to 2022 was tested via the chi-square test.
Results
Demographics
After Dobbs v. Jackson we observed an increase in non-resident abortions (before DvJ: 10.94%, after DvJ: 31.82%; p < 0.01), an increase in the proportion of medical non-surgical abortions (before: 42.83%; after: 69.15%; p = 0.10), and an increase in the proportion of abortions after gestation week 25 (before: 0.28%; after: 1.47%, p < 0.01). See Table 1. We observed a change in the frequencies of types of procedure performed with the biggest shift for Medical (Nonsurgical) abortions (before: 42.82%, after: 69.16%, p < 0.01).
Table 1. Summary of monthly incident abortions and associated demographic data for Colorado stratified by (left column) those months before the Dobbs vs. Jackson decision (Jan. 2004 to June 2022) and (right column) those months after the decision (July 2022 to Dec. 2023)Demographic variableColoradoJanuary 2004–June 2022ColoradoJuly 2022–December 2023Average Abortion Incidence Non-Resident10.94%31.82% Resident89.06%68.18%Age (yrs) < 150.38%0.32% 15–1912.99%9.90% 20–2432.03%31.81% 25–2925.57%27.77% 30–3416.04%17.7% 35+12.99%12.55%Race/Ethnicity White Non-Hispanic64.91%68.76% White Hispanic8.40%3.01% Black9.08%19.1% Other17.60%9.13%Marital Status Married18.33%15.88% Unmarried81.67%84.12%Gestation Week <= 869.63%69.15% 9–2430.09%29.93% 25+0.28%1.47%Type of Procedure Performed Suction Curettage48.09%25.8% Medical (Nonsurgical)42.83%69.15% Dilation and Evacuation5.97%3.6% Other3.11%2.1%
Increase in Non-resident Abortion Incidence After Dobbs v. Jackson Decision
The total number of monthly incident abortions in Colorado increased after DvJ (before 878; after 1180; p < 0.01). This number, however, does not provide the full picture. We observed a 2.89 times increase in the number of non-resident abortions after DvJ (monthly mean incident cases = 366) compared to before DvJ (monthly mean incident cases = 94); p < 0.01; Table 2), while the number of incident abortions among residents increased only 1.04 times or 5.6% (p = 0.19) from a mean of 782 to 818 abortions.
Table 2. The mean total, non-resident, and resident monthly incident abortions before (January 2004–June 2022) and after (July 2022–December 2023) the Dobbs vs. Jackson decision, the relative difference, and Pvalue to test if there was a significant differencePopulationColorado before DvJ (January 2004–June 2022)Colorado after DvJ (July 2022–December 2023Relative differenceTwo-sample pvalueTotal abortion incidence878119035.5%< 0.01Non-resident abortion incidence94366289.3%< 0.01Resident abortion incidence7828185.6%0.19
Marked Increase in Incident Abortions Near the Dobbs v. Jackson Decision in Time
We found an estimated 2,449 (95CI = [1,728, 3,171]; p < 0.01) increase in the number of non-resident abortions and 4,391 increase in total (resident plus non-resident) number of abortions (95CI = [491, 8,292]; p = 0.03) in the six months, and year after, the DvJ ruling (See Table 3 for Interrupted Time Series analysis estimates and Fig. 1). There was an approximate increase of 2,014 resident abortions (95CI = [−1447, 5475]) during this time period (p = 0.24). An increase in the rate of incident abortions after the DvJ was not statistically significant, but the maximum likelihood estimate suggested a positive increase.
Fig. 1. Interrupted time series analysis for Colorado total terminations, non-resident terminations, and resident terminations from 2004 to 2023, including long-term trend projections
Table 3. The point estimate, 95% confidence interval, and p-value from interrupted time series analysis of annual abortion incidence in Colorado, stratified by total, non-resident, and resident abortions, before (2004–2022) and after (2022–2023) the Dobbs v. Jackson decisionPopulationPoint estimate95% CIp-valueAnnual Total Abortion Incidence 2004–2023 Change in rate of incident abortions after DvJ (P)49.65[−162.01, 261.30]0.63 Shift in abortion incidence at time of DvJ (D)4391.56[491.12, 8292.00]0.03Annual Non-resident Abortion Incidence 2004–2023 Change in rate of incident abortions after DvJ (P)25.45[−13.70, 64.60]0.19 Shift in abortion incidence at time of DvJ (D)2449.66[1728.19, 3171.13]< 0.01Annual Resident Abortion Incidence 2004–2023 Change in rate of incident abortions after DvJ (P)17.61[−170.23, 205.45]0.85 Shift in abortion incidence at time of DvJ (D)2014.32[−1447.19, 5475.82]0.24
Evidence suggests an increase in incident abortion numbers near the DvJ decision impacted the ability for health centers to care for the increase of abortion care patients in a timely manner. Planned Parenthood of the Rocky Mountains reported wait times of 28 days immediately after DvJ. Longer wait times lead to implications for women, as elaborated in the Discussion.
Surrounding States that Experienced Changes in the Rate of Non-resident Abortions to Colorado
The proportion of non-resident abortions from surrounding states grew significantly from the years 2020 (n = 1242.0) to 2023 (n = 4142.0), a change of 233.45%. Of all states, residents from Texas and Oklahoma showed the biggest shift in receiving abortive care in Colorado, relative to other surrounding states. Texas had a 277.78% increase in the proportion of residents receiving abortion care in Colorado from 2020 (0.18%) to 2023 (0.68%). In Colorado, the mean incident cases of Texas residents grew from 316.5 in the years leading up to DvJ (2020–2021) to 2632.0 after DvJ (2022–2023), a 731.6% increase. Colorado also experienced a significant change in the proportion of Oklahoma state residents from 0.01% to 0.04% of the total non-resident abortions, an increase of 300%. Total Oklahoma abortions changed from a mean incidence of 13.5 (2020–2021) to a mean incidence of 189.5 (2022–2023), an increase of 1303.7%.
Average Gestation Week During Termination is Later After DvJ Decision
After the DvJ decision, the average number of monthly abortions increased for women with later gestation weeks (see Fig. 2): (1) Less than 8 weeks increased from 7,205 on average in 2004–2021 to 9,927 on average in 2022–2023 or a 27.8% increase; (2) 9 to 24 weeks increased from 3,112 on average in 2004–2021 to 4,130 on average in 2022–2023 or a 32.7% increase; and, most notably, (3) 25–28 or more weeks increased from 14 on average in 2004–2021 to 235 average in 2022–2023 or a 1578.6% increase (Please find a table of results in the Supplement).
Fig. 2. Prevalence of abortion procedures stratified by gestation week in Colorado from 2004 to 2023
Discussion
Data collected from Colorado on incident abortions from 2004 to the present suggest that the Dobbs decision has resulted in an increase in total terminations driven by non-residents from the states surrounding Colorado. There is evidence that the uptick in non-resident abortions has likely led to longer wait times, a higher burden on facilities, and later gestation times for the woman.
Restrictive abortion legislation enacted in individual states following DvJ has led to residents traveling to states with less restrictive laws for care. The ruling of DvJ resulted in 13 states’ trigger laws severely restricting or banning abortion almost immediately. Currently there are 14 total state bans and 27 partial bans as of June 2024. Of these states, Texas and Oklahoma have banned abortion with very limited exceptions (Guttmacher Institute, 2024). Colorado has since experienced tremendous increases in non-resident abortions from surrounding states like Texas and Oklahoma. Prior to 2022, Texas reported an average of approximately 50,000 in-state abortions annually, but only 62 in 2023 after DvJ (Texas Health and Human Services, 2024). In 2023 Oklahoma reported a total of 0 in-state abortions compared to an average of approximately 5,200 in the years prior DvJ (Oklahoma State Department of Health, 2024; Charlotte Lozier Institute, 2023). A comprehensive analysis of Texas and Oklahoma vital statistics was not performed as part of this study. However, based on our Colorado state data, we infer that restrictive states like Texas and Oklahoma are displacing residents seeking abortion onto states with less restrictive laws, such as Colorado. Additional examination of incident cases in other states with greater protections for those seeking abortions is warranted to better understand what is happening at a national level.
The immediate increase in the number of out-of-state residents seeking care after DvJ has resulted in longer wait times for patients. Colorado’s reported 28 day wait time immediately after DvJ, was 11 days longer than the typical wait time of 17 days in the months prior to the decision (Ungar, 2023). The 17-day wait times in Colorado likely were a result of the enacting of the Texas Heartbeat Act and the creation of Texas’s trigger law in 2021. Otherwise in the years leading up to DvJ, many states had average wait times of only 5 days (Ungar, 2023).
Use of telehealth for non-surgical abortions in Colorado and similar states has been important in improving appointment wait times for patients living in restrictive states (Upadhyay et al., 2024). Telehealth appointments that can prescribe medical abortions using medications such as Mifepristone and Misoprostol for women with a gestation time of less than 10 weeks have increased in response to excess burden at healthcare facilities. In Colorado, before DvJ, the proportion of medical terminations was 42.82% and after, 69.16%. Though telehealth may be a way for some individuals to receive abortion care in a timely fashion, it is only useful for early abortions and, thus, does not take the place of surgical care for many women.
Appointment delays in Colorado may be a driving factor behind the 1578.6% increase in abortions after gestation week 25 that was observed in 2022–2023. Colorado has reported experiencing higher volumes of patients seeking abortion in later stages of pregnancy due to the several weeks delay in appointments. Colorado is also one of only 8 states with abortion legislation that does not restrict termination at any gestation week (Guttmacher Institute, 2024; Ungar, 2023). Unfortunately for patients, as appointment delays push them later into pregnancy, the cost for an abortion increases from an average 1,500-$2,000 in the second trimester (Planned Parenthood, 2022). Maternal health concerns also increase as abortion is pushed further into the later stages of pregnancy. Being denied abortion is associated with higher risk of eclampsia, postpartum hemorrhage, gestational hypertension, and a four times greater odds of living below the federal poverty line (Foster, 2020).
The shift in gestational age at time of termination to later in pregnancy complicates the impact of the Dobbs decision. Many states enacted restrictions on abortions, not complete bans. These restrictions were based primarily on gestation time. The influx of patients seeking care from states with bans on abortions has caused greater waiting periods, likely including in states that have gestational restrictions. Thus, people seeking abortions in these states may miss the time period that is legal in their state, sending them to states like Colorado without limitations. As a result, Colorado and other states with similar laws will likely face even more increases in late-term abortions with higher cost and greater health concerns.
In addition to financial costs changing at an individual level, the high costs of abortions impact health care spending at the state and national levels. National reproductive organizations have had to increase their spending to assist patients in restrictive states. Since DvJ, Planned Parenthood has increased its patient assistance funding from 9 million in the year after (Daley, 2023). Between 2021 and 2022, the Baltimore Abortion Fund has distributed three times the amount of funds to those who need assistance and has experienced 33% more calls to their hotline after DvJ (Forouzan et al., 2023). The National Network of Abortion Funds has also estimated their disbursements to callers seeking support has more than tripled within one year after DvJ (Forouzan et al., 2023).
It is not yet fully known the extent of the effects that DvJ has on patients, the healthcare system, or organizations like Planned Parenthood. To better understand the severity of DvJ on abortion-protecitve states like Colorado, there needs to be more frequent reporting in abortion incidence. Some states publish publicly-available, annual data on induced terminations; however, not all states do so. Advocating for nationwide or state policies surrounding the reporting and public dissemination of abortion incidence, at least bi-annually, would allow researchers to study the impacts of DvJ across the country more effectively.
Limitations
The data reported by the CDPHE included state level demographic information for terminations occurring within the state from 2004 to 2023. The data and analysis were limited because the information was not linked to the patient, which made it difficult to draw conclusions about how factors like socioeconomic status are involved in the changes in abortion incidence in Colorado. Future work should collect case-specific data to estimate the association between state residence, race, and gestation week at time of abortion.
Though extensive, the CDPHE data reporting was inconsistent in reporting metrics. Demographic characteristics such as marital status, age, and race were reported monthly from 2004 to 2023. Data on state of residence was reported annually from 2004 to 2023. Inconsistencies in the frequency of reporting affected our analysis, resulting in the use of multiple different data subsets. Reported demographic data was also not inclusive of all races/ethnicities, but rather only reported (1) White non-Hispanic, (2) White Hispanic, (3) Black, and (4) Other. Our research team interpreted the Other category to include all excluded racial and ethnic groups. Lastly, DvJ remains a current event; there is limited data since June 2022 to study the extent of the impact on healthcare facilities or individuals.
Our study begins to understand how DvJ has resulted in changes in abortion incidence in abortion-protective states. In studying the state of Colorado, we observed a significant increase in the incidence of total terminations and attributed the change to an influx of non-resident patients from states with severely restrictive abortion legislation. Our findings suggest that as individual states across the country restrict abortion access, protective states like Colorado will continue to experience higher volumes of total terminations, and late-gestation terminations, driven by non-residents, likely impacting appointment wait times and abortion access.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baden, K., Dreweke, J., & Gibson, C. (2024). Clear and growing evidence that Dobbs is harming reproductive health and freedom. Guttmacher Institute. https://www.guttmacher.org/2024/05/clear-and-growing-evidence-dobbs-harming-reproductive-health-and-freedom
- 2Charlotte Lozier Institute. (2023). Abortion reporting: Oklahoma (2023). Charlotte Lozier Institute. https://lozierinstitute.org/abortion-reporting-oklahoma-2023
- 3Daley, J. (2023). Abortion numbers rise sharply in Colorado, driven by out-of-state patients. Colorado Public Radio. https://www.cpr.org/2023/09/11/abortion-numbers-rise-sharply-in-colorado-driven-by-out-of-state-patients/
- 4Forouzan, K., Friedrich-Karnik, A., & Maddow-Zimet, I. (2023). The high toll of US abortion bans: Nearly one in five patients now traveling out of state for abortion care. Guttmacher Institute. https://www.guttmacher.org/2023/12/high-toll-us-abortion-bans-nearly-one-five-patients-now-traveling-out-state-abortion-care
- 5Guttmacher Institute. (2024). Interactive map: US abortion policies and access after Roe. Guttmacher Institute. https://states.guttmacher.org/policies/
- 6Institute for Women’s Policy Research. (2021). Costs of reproductive health restrictions. IWPR. https://iwpr.org/costs-of-reproductive-health-restrictions/
- 7National Abortion Federation. (2023). Violence against abortion providers continues to rise following Roe reversal, new report finds. https://prochoice.org/violence-against-abortion-providers-continues-to-rise-following-roe-reversal-new-report-finds/
- 8Oklahoma State Department of Health. (2024). Abortion surveillance in Oklahoma summary report. https://oklahoma.gov/content/dam/ok/en/health/health 2/aem-documents/data-and-statistics/center-for-health-statistics/induces-termination-of-pregnancy/2023%20Abortion Report.pdf