Septic Thrombophlebitis of the Portal Vein: A Case Report
Megana Ballal, Eyong J Ly

TL;DR
This paper presents a case of a 53-year-old woman with septic portal vein thrombosis, emphasizing the challenges in diagnosing and treating this rare condition.
Contribution
The novelty lies in the detailed clinical presentation and management of a rare complication of intra-abdominal infection.
Findings
The patient presented with fever and abdominal pain, leading to the diagnosis of portal vein thrombosis.
Antibiotics and anticoagulation were used in treatment, reflecting standard approaches for pylephlebitis.
Abstract
Pylephlebitis, a septic thrombophlebitis of the portal vein, typically arises as a complication of intra-abdominal infection. We report the case of a 53-year-old woman whose presenting symptoms included fever and abdominal pain. Imaging revealed portal vein thrombosis. An evaluation was performed to identify a potential underlying infectious source. She was treated with antibiotics and anticoagulation. This case highlights the diagnostic and therapeutic complexities in the evaluation and management of pylephlebitis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
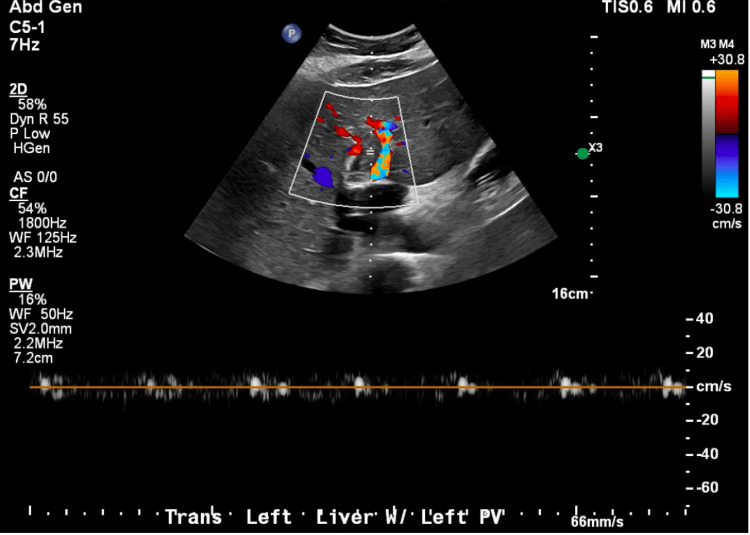 Figure 1
Figure 1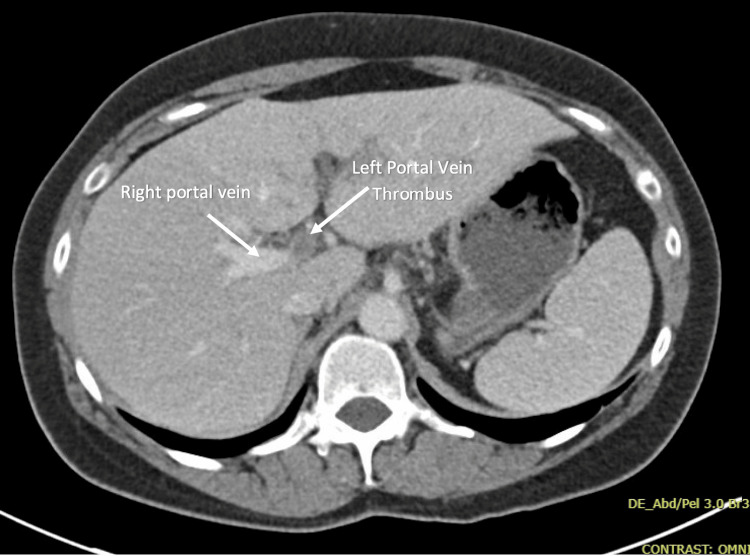 Figure 2
Figure 2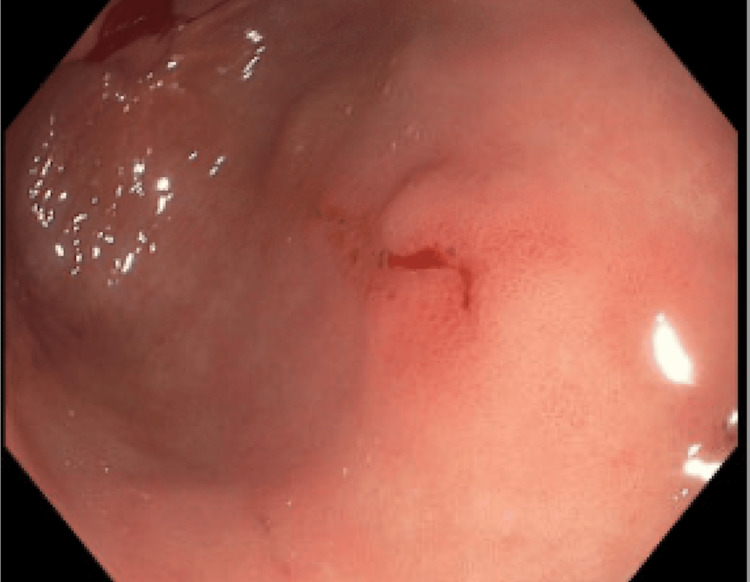 Figure 3
Figure 3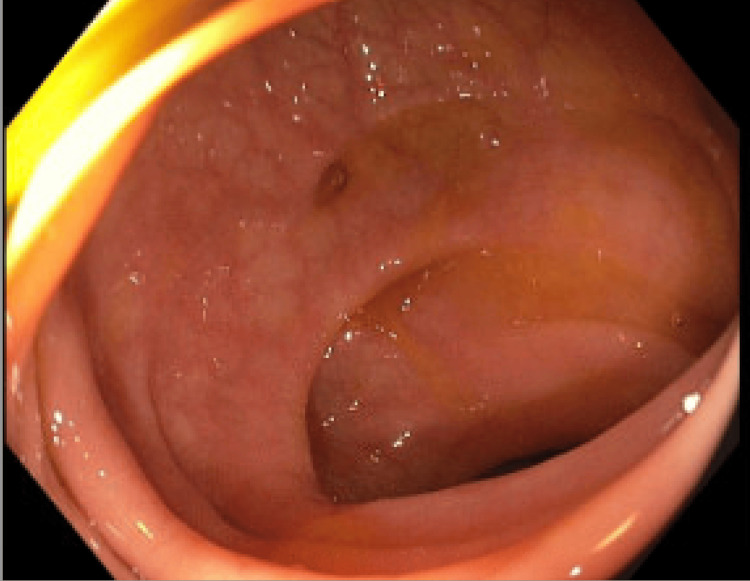 Figure 4
Figure 4| Lab | Patient's lab value | Reference range and unit |
| White blood cell count | 10.41 | 4.16-9.95 x 10E3/µL |
| Hemoglobin | 12.8 | 11.6-15.2 g/dL |
| AST | 134 | 13-62 U/L |
| ALT | 218 | 8-70 U/L |
| Conjugated bilirubin | 0.4 | <=0.3 mg/dL |
| Total bilirubin | 0.8 | 0.1-1.2 mg/dL |
| Total protein | 8.9 | 6.1-8.2 g/dL |
| INR | 1.3 | 0.8-1.2 |
| Albumin | 3.9 | 3.9-5.0 g/dL |
| C-reactive protein | 27.8 | <0.8 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Amoebic Infections and Treatments · Gallbladder and Bile Duct Disorders
Introduction
Pylephlebitis is considered a type of portal vein thrombosis (PVT). It is a rare but potentially life-threatening complication of an intra-abdominal infection in an area drained by the portal venous system. Diverticulitis and pancreatitis are two intra-abdominal conditions commonly associated with pylephlebitis [1]. Its clinical presentation can be nonspecific, including fever and abdominal pain. Contrast-enhanced imaging has become critical for prompt diagnosis. The cornerstones of treatment are broad-spectrum antibiotics, with the regimen tailored to the source of infection and culture results, in combination with anticoagulation. While historically more controversial, anticoagulation is now increasingly supported, given evidence of improved outcomes [1]. PVT is uncommon in patients without cirrhosis. In patients who develop PVT in the absence of cirrhosis or another provoking factor, evaluation for an underlying thrombophilic condition is recommended [2]. Although advances in recognition and treatment have reduced morbidity and mortality in recent decades, maintaining a high index of clinical suspicion remains crucial for timely diagnosis.
Case presentation
A 53-year-old woman with a history of eczema presented to the emergency department with fever, chills, epigastric pain, nausea, and vomiting. She had similar symptoms three weeks ago, which resolved after a week. Her symptoms recurred four days before presentation. Her temperature was up to 103 °F at home, for which she was taking Tylenol and ibuprofen one to two times a day. She tested negative for COVID, influenza, and respiratory syncytial virus one day earlier in the clinic. She had no prior surgeries and took no medications. She had a family history of Crohn’s disease. She had no history of tobacco, illicit drug, or significant alcohol use.
On presentation, the patient was afebrile, and vitals were unremarkable with the exception of an elevated heart rate at 117 beats per minute. Mild epigastric tenderness to palpation was noted on physical exam. Initial labs are shown in Table 1.
An abdominal ultrasound showed an isolated left PVT (Figure 1).
Abdominal ultrasound of the left portal vein.Ultrasound demonstrated a patent right portal vein with normal flow direction, as well as thrombosis of the left portal vein without an associated mass lesion.
Blood cultures were drawn on admission, which were ultimately negative. On hospital day 2, repeat blood cultures were ordered given fever and malaise, and she was empirically started on ceftriaxone and metronidazole. An infectious disease specialist was consulted, and the patient was continued on these antibiotics based on the suspicion of an initial gastrointestinal infection with bacteremia that progressed to pylephlebitis. She was also started on a therapeutic dose of enoxaparin. A computed tomography (CT) scan of the abdomen and pelvis with contrast showed complete thrombosis of the left portal venous system with no specific findings of hepatic or enteric inflammation or malignancy (Figure 2).
CT abdomen and pelvis with contrast showing a portal vein thrombus.An axial (transverse) CT image shows a filling defect in the left portal vein, consistent with complete thrombosis of the left portal venous system.
One of the blood cultures was positive for Bacteroides fragilis. Urine culture was negative. She underwent endoscopy and colonoscopy on hospital day 5 as the source of bacteremia remained unclear. The endoscopy showed two clean-based antral ulcers, with a biopsy negative for Helicobacter pylori or intestinal metaplasia (Figure 3).
Antral ulcer.
The colonoscopy demonstrated diverticulosis (Figure 4).
Colonoscopy demonstrating diverticulosis.
Evaluation for infectious or autoimmune causes of hepatitis was unremarkable.
Given the resolution of fevers with clinical improvement and no sign of active infection on colonoscopy, ceftriaxone was discontinued after five days. Blood culture susceptibility testing demonstrated sensitivity to metronidazole. The patient was discharged on metronidazole with a plan to complete four weeks of treatment. She was transitioned to apixaban on discharge and also provided with pantoprazole twice daily, given the endoscopy findings. The patient was evaluated by hematology as an inpatient and had an outpatient follow-up. A hypercoagulable workup was performed and was negative for antiphospholipid syndrome, paroxysmal nocturnal hemoglobinuria, myeloproliferative neoplasms, inherited thrombophilias, and protein C or S deficiency. Therefore, her presentation was suspected to be due to pylephlebitis. The source of bacteremia remained unclear, although there was a suspicion of diverticulitis despite negative imaging based on her initial presentation and that diverticulosis was found on colonoscopy. She was advised to continue anticoagulation for six months.
Discussion
Pylephlebitis is defined as septic thrombophlebitis of the portal vein. It was described by Waller as early as 1846 [1]. According to the American Association for the Study of Liver Disease, PVT is considered a heterogeneous condition in terms of cause, presentation, prognosis, and management [2]. PVT is less commonly seen in patients without cirrhosis [3]. Pylephlebitis is considered a type of PVT. It is an infrequent complication of intra-abdominal infections [4]. Although this condition is rare, it is associated with significant morbidity and mortality. Prompt diagnosis and treatment are crucial to prevent long-term complications.
While the prevalence of PVT increases with the severity of cirrhosis, PVT remains uncommon among the general population [5]. The reported cases of pylephlebitis have increased over time, but the incidence remains low with an estimated 0.37-2.7 cases per 100,000 person-years [6]. A systematic review of 220 cases of pylephlebitis between 1971 and 2022 demonstrated that 70.5% of patients were male, with a median age of 50 years [6]. Pylephlebitis can occur as a complication of infection in an area drained by the portal system, with diverticulitis, pancreatitis, and appendicitis among the most common causes [1]. The diagnostic criteria for pylephlebitis are not clearly established. Choudhry et al. defined pylephlebitis as PVT within 30 days of an intra-abdominal inflammatory process with or without bacteremia [1]. Other review articles have defined this condition as PVT in patients with fever and bacteremia, although it was acknowledged that negative blood cultures shouldn’t rule out the diagnosis [6].
The clinical presentation of pylephlebitis can be nonspecific, with possible symptoms including fever, malaise, abdominal pain, and nausea [1]. Physical exam may or may not include right upper quadrant tenderness. Leukocytosis as well as elevated serum transaminases, C-reactive protein, and erythrocyte sedimentation rate occurred in the majority of patients [6]. Escherichia coli, Bacteroides spp., and Streptococcus spp. were the most commonly isolated pathogens, although no bacteria were identified in 30% of cases [6]. Ultrasound can be used for screening when there is suspicion for portal vein pathology, however it is operator dependent. Therefore, contrast-enhanced CT or magnetic resonance imaging (MRI) is useful to confirm the diagnosis and evaluate the clot burden [7].
Treatment of pylephlebitis starts with broad-spectrum antibiotics, with the specific medication depending on the suspected source of infection. Options for initial antibiotics include Ceftriaxone 2 g daily plus Metronidazole 500 mg every 8 hours, as well as monotherapy with Piperacillin-tazobactam 4.5 g every 8 hours. The duration of treatment is typically at least four to six weeks after symptom onset [6]. The role of anticoagulation has not been as clear; the use of anticoagulants has increased in recent years to include the majority of patients, especially when there is thrombus progression on repeat imaging or ongoing fever on appropriate antibiotic therapy [6]. Anticoagulation can increase the rate of thrombus resolution and decrease the rate of complications associated with chronic portal hypertension [8]. There is also no set recommendation on the exact duration of anticoagulation, with some data suggesting three to six months if there is no other cause of thrombophilia [1]. Invasive therapeutic approaches such as thrombectomy are not routinely used, as they are not the first-line treatment.
Mortality from pylephlebitis has decreased to less than 10% since 2010, suggesting that diagnosis and treatment of this condition may have improved over time [6]. Complications associated with pylephlebitis include cavernous portal vein transformation or persistent portal vein thrombosis causing portal hypertension, dissemination of infection, including liver abscesses, and intestinal ischemia [6]. A study of 67 patients found that there was a 58% rate of portal vein thrombosis resolution among those who took anticoagulation, compared to 21% among those who did not [8]. Pylephlebitis is a rare but serious condition. The prognosis can vary depending on the timing of diagnosis and initiation of treatment, as well as identification of complications.
Conclusions
Pylephlebitis is an uncommon but potentially life-threatening condition that can occur as a complication of an intra-abdominal infection. As illustrated by this case, its variable and nonspecific presentation underscores the need for a high index of suspicion, given its associated morbidity and mortality. Prompt imaging is essential to identify PVT and guide management, with antibiotics and anticoagulation serving as the mainstays of treatment. Ongoing research aims to clarify guidelines on anticoagulation and develop strategies to improve early recognition and intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pylephlebitis: a review of 95 cases J Gastrointest Surg Choudhry AJ Baghdadi YM Amr MA Alzghari MJ Jenkins DH Zielinski MD 6566612020162616032010.1007/s 11605-015-2875-3PMC 4882085 · doi ↗ · pubmed ↗
- 2Vascular liver disorders, portal vein thrombosis, and procedural bleeding in patients with liver disease: 2020 practice guidance by the American Association for the Study of Liver Diseases Hepatology Northup PG Garcia-Pagan JC Garcia-Tsao G 3664137320213321952910.1002/hep.31646 · doi ↗ · pubmed ↗
- 3Diagnosis, development, and treatment of portal vein thrombosis in patients with and without cirrhosis Gastroenterology Intagliata NM Caldwell SH Tripodi A 1582159915620193077135510.1053/j.gastro.2019.01.265 · doi ↗ · pubmed ↗
- 4Pylephlebitis: an uncommon complication of intra-abdominal infection West J Emerg Med Hagopian T Zuniga F Surani SR 5755761220112222416510.5811/westjem.2011.1.2197 PMC 3236157 · doi ↗ · pubmed ↗
- 5Current knowledge and management of portal vein thrombosis in cirrhosis J Hepatol Senzolo M Garcia-Tsao G García-Pagán JC 4424537520213393047410.1016/j.jhep.2021.04.029 · doi ↗ · pubmed ↗
- 6Pylephlebitis: a systematic review on etiology, diagnosis, and treatment of infective portal vein thrombosis Diagnostics (Basel) Fusaro L Di Bella S Martingano P CrocèLS GiuffrèM 13202310.3390/diagnostics 13030429 PMC 991478536766534 · doi ↗ · pubmed ↗
- 7Portal vein thrombosis: diagnosis and endovascular management Rofo Ju C Li X Gadani S Kapoor B Partovi S 16918019420223464928910.1055/a-1642-0990 · doi ↗ · pubmed ↗
- 8The role of anticoagulation in pylephlebitis: a retrospective examination of characteristics and outcomes J Thromb Thrombolysis Naymagon L Tremblay D Schiano T Mascarenhas J 3253314920203149329010.1007/s 11239-019-01949-z · doi ↗ · pubmed ↗