Hydrogel Micro/Nanostructures for the Delivery of Oncolytic Viruses: Overcoming Limitations and Improving Efficacy
Chou-Yi Hsu, Saade Abdalkareem Jasim, Jasur Alimdjanovich Rizaev, Tina Saeed Basunduwah, Vikrant Abbot, Mamata Chahar, Mohammed Asiri, Abbas Fadhel Ali, Alexey Yumashev, Ahmed Hussein Zwamel

TL;DR
This review explores how hydrogel micro/nanostructures can improve the delivery and effectiveness of oncolytic viruses in cancer therapy.
Contribution
The paper provides a comprehensive review of hydrogel-based strategies to overcome limitations in oncolytic virotherapy.
Findings
Hydrogels offer controlled release and precise delivery of oncolytic viruses.
Hydrogels can enhance therapeutic efficacy by combining with other treatments.
Hydrogels help overcome challenges like immune clearance and non-specific localization.
Abstract
Oncolytic viruses (OVs) have attracted accumulating attention in cancer therapy owing to their ability to replicate in and kill tumor cells, resulting in the stimulation of immune responses for eradicating residual and distant malignant cells. Despite milestone achievements in the development of OVs, which led to the U.S. Food and Drug Administration (FDA) approval of talimogene laherparepvec (T-VEC) in 2015 against melanoma, there are some hurdles limiting their translation from the bench to the clinic, such as non-specific localization, host immune response against OVs and their clearance, and low efficiency as a monotherapy. Delivery of OVs with nano-biomaterials is a promising approach to address the drawback of oncolytic virotherapy. Hydrogels, with their tunable characteristics and versatile properties, offer a promising platform for the controlled release, precise delivery, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
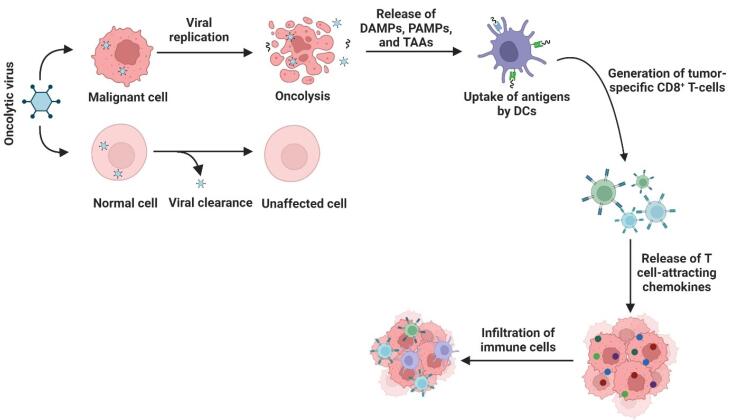 Figure 1
Figure 1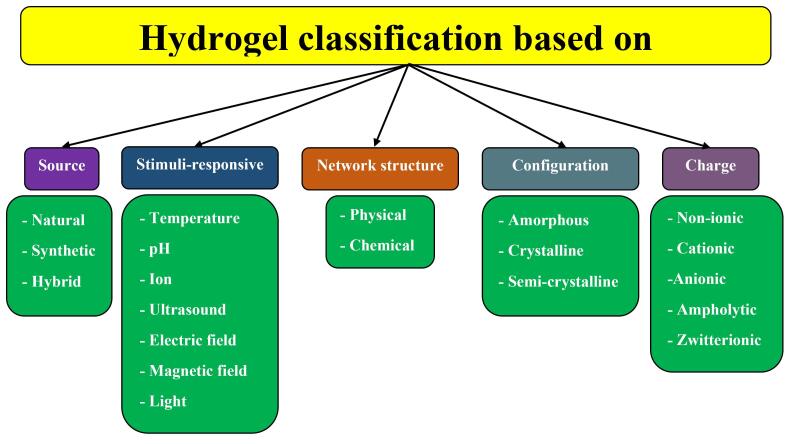 Figure 2
Figure 2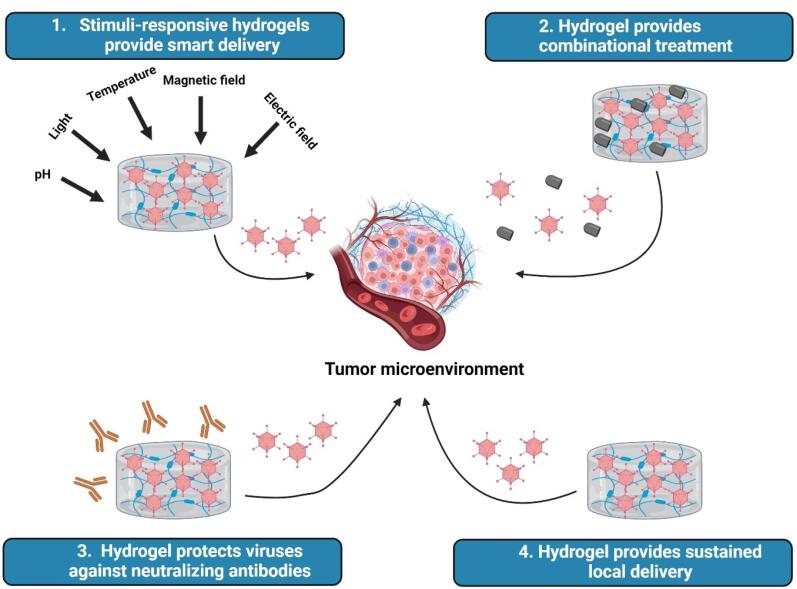 Figure 3
Figure 3|
|
|
|
|
|
|
|
| HSV | ||||||
| R130 | Solid tumors | IT/IP | - | Early 1 | Shanghai Yunying Medical Technology | |
| G207 | HGG | IT | Radiotherapy | II | Pediatric Brain Tumor Consortium | |
| T3011 | CRC | HAI | Toripalimab/Regorafenib | I | China Medical University, China | |
| OH2 | Melanoma | IT | - | III | Binhui Biopharmaceutical Co., Ltd. | |
| MVR-C5252 | Glioma | IT | - | I | Duke University | |
| RP2/RP3 | CRC | Direct or image-guided injection | Atezolizumab/ Bevacizumab | II | Replimune Inc. | |
| Adenovirus | ||||||
| H101 | Cervical | IT | Camrelizumab | II | Zhejiang Cancer Hospital | |
| TILT-123 | Ovarian | IT/IP | Pembrolizumab | I | TILT Biotherapeutics Ltd. | |
| H101 | ICC | IT | HAIC | IV | Beijing Tsinghua Chang Gung Hospital | |
| CG0070 | IR-NMIBC | N/A | TURBT | III | CG Oncology, Inc. | |
| KD01 | Cervical | IT | - | I | Tongji Hospital | |
| AdAPT-001 | Sarcoma/ Solid tumors | IT | - | II | EpicentRx, Inc. | |
| VACV | ||||||
| OVV-01 | Solid tumors | IT | Pembrolizumab/ Atezolizumab | I | North China Petroleum Bureau General Hospital | |
| TBio-6517 | Solid tumors | IT/IV | Pembrolizumab | I/II | Turnstone Biologics, Corp. | |
| hV01 | Pancreatic | IT | - | II | Hangzhou Converd Co., Ltd. | |
| Olvi-Vec | Ovarian | IP | Platinum-doublet/ Bevacizumab | III | Genelux Corporation | |
| IDOV-Immune | Solid tumors | IV | - | I | ViroMissile, Inc | |
| RGV004 | BCL | IT | - | I | Second Affiliated Hospital, School of Medicine, Zhejiang University | |
| MV | ||||||
| MV-s-NAP | Breast | IT | - | I | Mayo Clinic | |
| MV-NIS | Myeloma | IV | Cyclophosphamide | II | University of Arkansas | |
| Reovirus | ||||||
| Pelareorep | TNBC | IV | INCMGA00012 | II | Mridula George, MD | |
| Pelareorep | MM | IV | Bortezomib/ Pembrolizumab | I/II | University of Southern California |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVirus-based gene therapy research · Viral Infectious Diseases and Gene Expression in Insects · Viral gastroenteritis research and epidemiology
Introduction
Conventional cancer treatment strategies, such as chemotherapy and radiotherapy, are not optimally effective due to their mechanism of action, which is based on interrupting cell division, affecting normal cells along with tumor cells.^1^ Fortunately, as our understanding of cancer has improved, including the molecular and genetic basis of cancer as well as tumor microenvironment (TME) and its cellular components and interactions, cancer treatments have far surpassed these traditional strategies and their side effects.^2^ Over the past decade, there have been several advances that have improved survival rates for some common solid tumors. One of these advances comes from developing cancer immunotherapy strategies, aiming to activate the body’s immune responses against malignant cells.^3^ As a main branch of immunotherapy, oncolytic viruses (OVs) have attracted particular attention owing to their ability to preferentially replicate within tumor cells and lyse them without affecting non-malignant ones.^4^ Currently, different viruses have been investigated as oncolytic agents for the treatment of cancers, including herpes virus, adenovirus, Newcastle disease virus (NDV), reovirus, measles virus, vaccinia virus, and poliovirus.^5^ These investigations led to the approval of four OV-based drugs for the treatment of tumors: H101, T-vec, Rigvir, and G47Δ.^6,7^ Despite these advancements and approvals, the translation of in vitro and pre-clinical studies to the clinic and finally to the market faces obstacles, such as immune responses against OVs, passive targeting, spread and penetration, short duration of biological activity, rapid clearance, and poor persistence in the target tissue.^8-10^ Therefore, nano-sized tools and nanomaterials have been developed to circumvent the obstacles and join OVs and nanomaterials forces against cancer.^11^
Hydrogels are three-dimensional biomaterials with hydrophilic properties and cross-linked polymer chains, proposing them as promising structures for biomedical applications, including tissue engineering, drug screening, biosensors, bioimaging, drug delivery, and cancer immunotherapy.^12,13^ Regarding cancer immunotherapy, hydrogels not only serve as a delivery vehicle and a container of immune cells such as dendritic cells, macrophages, and chimeric antigen receptor (CAR) T-cell cells, immunomodulators, and cancer vaccines, but also provide a structure for a combination of immunotherapy and chemotherapy, called chemo-immunotherapy.^12,14^ To reach optimal therapeutic efficacy of OVs, they require escape from recognition by the host immune system as well as persistence and local delivery, for which hydrogel nano/microstructures can be considered suitable vehicles.^15^ Besides their ability to increase the concentration of the cargo at the target sites and provide controlled release, hydrogels reduce side effects and non-specific distribution of their cargo.^16^ Additionally, developing smart hydrogels that respond to external stimuli or internal ones allows them to specifically and under certain conditions release their cargo, leading to a high degree of targeting.^17^ Therefore, hydrogels with their tunable characteristics and versatile properties, offer a promising platform for the controlled release, precise delivery, and therapeutic enhancement of OVs in the treatment of cancer. Here, we will review different viruses with oncolytic activity, their mechanism of action, and their application in clinical trials. Also, we will discuss the characteristics of hydrogels as carriers of OVs and, finally, our focus will be on the state-of-the-art of hydrogel nanostructures applied in oncolytic virotherapy of cancers.
Oncolytic virotherapy in cancer
Viruses were once called “evil devils” for their role in disease, but with the rise of therapeutic viruses, especially OVs, they became “noble angels.” OVs exert their therapeutic effect through a dual mechanism (Figure 1). First, they selectively replicate in tumor cells, causing direct oncolysis. During the process of oncolysis, virus progeny will be released shortly thereafter to infect neighboring cancer cells and amplify the therapeutic response locally. Second, and importantly from an immunotherapy standpoint, destroyed tumor cells release tumor-associated antigens (TAAs), damage-associated molecular patterns (DAMPs) and pathogen-associated molecular patterns (PAMPs).^18^ This series of events initiates a strong anti-tumor immune response that can convert an overall immunologically “cold” tumors to “hot” tumors. As mentioned earlier, the immunogenicity of OVs prevents them from being neutralized, which means they can be neutralized by the host immune system before they induce a response, thereby limiting their persistence and efficacy in systemic situations. Hydrogel delivery systems are designed to circumvent this immunogenicity by protecting the virus from neutralizing antibodies and immune responses, resulting in localized delivery and prolonged release of OVs within the TME.^19^ Some OVs are naturally oncolytic in their native forms, called naturally occurring OVs (e.g., measles virus, NDV, and reovirus), whereas others require genetic modifications to exert their oncolytic functions, called genetically engineered OVs (e.g., vaccinia virus, herpesvirus, and adenovirus).^20^ Despite promising results in (pre)clinical studies, four OVs have been approved for the treatment of cancers: Rigvir (SND005) for the treatment of melanoma in Latvia (2004), Oncorine (H101) for the treatment of squamous cell cancer of the head and neck or esophagus in China (2005), Talimogene laherparepvec (T-VEC, Imlygic) for the treatment of melanoma by the U.S. FDA (2015), and Delytact (teserpaturev/G47Δ) for the treatment of malignant gliomas in Japan (2021).^21^ Table 1 summarizes some OVs in clinical trials for cancer therapy.
**
Herpes simplex virus
The only FDA-approved OV in cancer therapy is a herpes simplex virus (HSV-1)-derived agent, called T-VEC, in which viral infected cell protein (ICP) 34.5 and ICP47 genes were deleted and the human granulocyte-macrophage colony-stimulating factor (GM-CSF) gene was inserted into the genome of the virus. ICP34.5 deletion attenuates the neurovirulence capacity and improves tumor-selective replication of the virus, whereas ICP47 deletion declines virally mediated inhibition of tumor-associated peptides and improves antigen presentation. Moreover, the unique short 11 gene (US11) translocation enhances the tumor-lytic activity of the virus and GM-CSF insertion increases APC recruitment.^22^ In addition to T-VEC, other HSV-based OVs have been developed and translated into clinical trials, such as G207, HSV-1716, rQNestin34.5, G47Δ, OH2, ONCR-177, and RP1.^23,24^
Adenovirus
Two main approaches have been used to develop oncolytic adenoviruses (Ads): deletions in the E1A and E1B gene regions and replacement of the native E1 promoter with tumor-specific promoters.^25^ Oncorine, an Ad5-based virus with deletions in the E1B (55 kDa) and E3 gene fragment (78.3-85.8 mu), is the first approved OV for clinical use. Deletion of E1B-55KD leads to selective replication of the virus within tumor cells with dysfunction of the P53 pathway, whereas deletion of the E3 gene fragment enhances the safety of the virus.^26^ The promising results of Oncorine inspired the entry of other oncolytic Ads into clinical trials, such as LOAd703, CG0070, OBP-301 (Telomelysin), DNX-2401, TILT-123, VCN-01, etc.^27^
While OAds show great potential, their delivery is still a critical hurdle to overcome. When administered systemically, they are commonly sequestered rapidly by the liver and spleen and neutralized by pre-existing anti-Ad antibodies, even at high viral doses.^28^ To address this, simple non-viral delivery vectors have been investigated, including lipid nanoparticles (LNPs) and polymeric nanoparticles, which can protect OAds from neutralizing antibodies and can easily be surface functionalized for active targeting.^29^ However, nanoparticles tend to have a small loading capacity, are associated with the potential for complement activation and rapid clearance, and are unable to be localized. Instead, in our hands, hydrogels appear to be a much better platform for local or regional delivery. When therapeutic agents are encapsulated in a hydrogel, this results in the formation of a localized depot that allows for sustained release of the cargo over days or weeks, while keeping its concentration high directly within the TME.^10,30,31^ This localized delivery really helps to circumvent systemic toxicity and is most readily applied to surgically accessible tumors or in regard to adjuvant therapy/biologic after tumor resection.^32,33^
Vaccinia virus
Several advantages make vaccinia virus (VACV) a favorable agent for oncolytic virotherapy: replication within the cytoplasm that reduces its mutagenesis possibility, an extensive and long history in humans that guarantees its safety, such as the smallpox vaccine, the capacity to carry long segments of foreign DNA, the ability to infect a wide range of cells, a natural tropism toward cancer cells, and a rapid replication and lytic rate to induce inflammation and immune responses.^34,35^ Although unmodified VACVs could lyse cancer cells, their application in the clinic is limited because of reported side effects, including fatal neuroencephalitis and hepatitis; thus, genomic modifications have been made to improve clinical efficiency by reducing immunogenicity and toxicity as well as enhancing tumor selectivity and therapeutic outcomes.^36^ For example, the J2R gene deletion, which encodes thymidine kinase (TK), is the most common modification during the development of oncolytic VACVs, leading to tumor-selective replication of the virus and reduced pathogenicity.^37^ JX-594 (Pexa-Vec®) is an oncolytic VACV in which the TK gene was inactivated, whereas GM-CSF and β-galactosidase were inserted.^38^ In addition to JX-594, other developed oncolytic VACVs also were tested in clinical trials, such as GL-ONC1 (GLV-1h68), TroVax, TG4010, PROSTVAC, PANVAC, rV-B7.1, MVA-5T4, and IN rVV.^36^
Measles virus
Hemagglutinin (H) and fusion (F) proteins of the virus envelope are involved in its attachment to the target cell and fusion, while CD150/SLAM, CD46, and nectin-4 are considered the main receptors of measles virus (MV). Due to the upregulation of CD46 on the malignant cells, MV exhibits oncotropism and induces cell death by inducing fusion of cells and the formation of syncytia.^39^ Engineering MVs by mutating the receptor binding sites targeted them toward EGFRvIII-expressing glioblastoma,^40^ folate receptor (FR)-α-expressing ovarian cancer,^39^ and CD20-expressing B-cell malignancies,^41^ whereas fusing targeting moieties such as antibody single-chain variable fragments (scFv),^42^ cystine knot proteins,^43^ and integrin-binding peptides^44^ has also been developed to direct oncolytic MVs toward tumor cells. To monitor oncolytic MV in vivo, the virus is engineered to express sodium iodide symporter (NIS), allowing their tracking using radiotherapy with iodine-131 (^131^I), 99m-technetium uptake, and γ-camera imaging of ^123^I.^45^ Various types of oncolytic MVs have entered clinical trials owing to their promising results in in vitro and in vivo studies, such as MV-s-NAP for breast cancer, MV-NIS for malignant pleural mesothelioma and multiple myeloma, MV-CEA and MV-NIS for ovarian epithelial cancer or primary peritoneal cancer, and TMV-018 for tumors of the gastrointestinal tract. For instance, a phase I clinical trial using MV-CEA in 22 glioblastoma patients revealed that MV-CEA improves overall survival and has no dose-limiting toxicity. Intratumoral administration of MV-CEA was also associated with pro-inflammatory remodeling of the tumor milieu and increased infiltration of CD8^+^T-cells within the TME.^46^ A vaccine, named MV-s-NAP, against metastatic breast cancer is under investigation (NCT04521764), in which MV encodes Helicobacter pylori neutrophil activating protein (NAP) to increase innate immune recruitment into the TME.
Other OVs
Besides the mentioned viruses, other ones have also been used as OVs, including reoviruses, protoparvoviruses, polioviruses, and NDV. Reolysin (Pelareorep) is an unmodified reovirus that was investigated in clinical trials either as monotherapy or in combination with other therapeutic agents, such as chemotherapy and immune checkpoint inhibitors. For instance, Noonan et al studied the combination of reolysin with carboplatin and paclitaxel for the treatment of metastatic pancreatic adenocarcinoma in a randomized phase II trial. Although reolysin exhibited a safe profile, it did not improve the progression-free survival (PFS) compared with monotherapy with chemotherapeutic agents. They also found that a chemotherapy combination is critical to improve immunological outcomes of reolysin.^47^ Furthermore, reolysin could suppress both CTL and NK cell responses owing to the upregulation of immune checkpoint molecules.^47,48^ The smallest OV under clinical investigation is H-1PV (ParvOryx), belonging to the protoparvovirus (PV) genus, with a 25 nm diameter.^49^ Due to its small size, H-1PV could cross the blood-brain/tumor barrier in humans and concentrate in the brain/tumor. A phase I/IIa clinical trial using H-1PV revealed that the virus is safe and could trigger an immunogenic stimulus in glioblastoma patients, including CTL infiltrations.^50^ Intravenous administration of H-1PV to seven patients with pancreatic ductal adenocarcinoma and at least one liver metastasis also confirmed its safety. H-1PV was not only present in the tumor samples, but also enhanced the levels of pro-inflammatory interleukins (such as IFN-γ, IL-8, IL-9, and IL-12), pro-migratory cytokines (such as CXCL9), and T-cells.^51^ To date, various types of oncolytic polioviruses have been developed against cancers, such as PVSRIPO and PV-1. More than ten clinical trials tried to investigate the safety and efficacy of PVSRIPO in the treatment of glioblastoma, melanoma, and breast cancer either as monotherapy or in combination with other agents (NCT04479241, NCT04577807, and NCT03564782). A phase 1 trial with PVSRIPO, a recombinant type I poliovirus (Sabin) vaccine carrying an internal ribosomal entry site (IRES) of human rhinovirus type 2, which uses CD155 to target malignant cells, in melanoma patients showed no serious adverse events with encouraging antitumor responses.^52^ In addition to the higher expression in solid cancers, CD155 upregulation on APCs activates tumor-associated APCs in the TME and augments type I/III IFN production, leading to tumor growth suppression.^53,54^ A phase II study of PVSRIPO plus pembrolizumab for recurrent glioblastoma (NCT04479241) showed a median overall survival of 12.5 months, which is favorable when compared to historical controls and suggests synergistic effects with immune checkpoint blockade.^55^ Likewise, pelareorep (reovirus) has shown promise in combination therapies. According to a phase I/II study, patients with metastatic pancreatic adenocarcinoma received pelareorep plus atezolizumab plus chemotherapy and showed favorable modulation of immune response in the TME, as well as an encouraging objective response rate.^56^ Taken together, unmodified and genetically engineered viruses could act as oncolytic agents to selectively target tumor cells.
Hydrogels: structures and characteristics
According to the descriptions, hydrogels contain various properties, including hydrophilicity, polymeric networks, three-dimensional, water-swollen, and cross-linked structures.^57^ Therefore, hydrogels can be classified into varied groups based on their diverse characteristics (Figure 2): 1) Source: The source of hydrogels can be natural, synthetic, or hybrid (combining natural and synthetic polymers). Natural sources of hydrogels come from collagen, gelatin, dextran, alginate, lignin, cellulose, agar-agar, and chitosan, whereas synthetic hydrogels are made from polymers such as N-vinyl 2-pyrrolidone (NVP), ethylene glycol (EG), vinyl acetate (VAc), methacrylic acid, hydroxy methyl methacrylate (HEMA), and ethylene glycol dimethylacrylate (EGDMA).^58^ Although natural-based hydrogels are bioactive, biodegradable, and biocompatible, their allergenicity, immunological risks, and weak mechanical strength and stability are considered their limitations.^59^ On the other hand, hybrid hydrogels take more attention in biomedicine due to their well-defined structures and higher capacity of water absorption, strength, and durability.^60^ 2) Stimuli-responsive: Hydrogels, according to various applications, can respond to different stimuli, including temperature, pH, and ionic strength. These hydrogels are also called smart hydrogels. For instance, thermoresponsive hydrogels undergo a phase transition from a sol phase to a gel phase due to temperature increase and return back to the liquid phase by decreasing the temperature to a certain range.^61^ 3) Network structure: Another criterion for hydrogel classification is based on cross-linking networks: physically cross-linked hydrogels (reversible gels) and chemically cross-linked hydrogels (permanent gels). Due to not using cross-linking agents and ease of production, physically cross-linked hydrogels have gained significant attention.^57^ 4) Configuration: Hydrogels also can be classified into three groups according to their configuration or structure: amorphous, crystalline, and semi-crystalline. Crystalline hydrogels contain a strongly packed polymer network structure with the order of crystallization, whereas amorphous ones consist of a random network at the molecular level. Additionally, semi-crystalline hydrogels are a mixture of amorphous and crystalline structures.^59^ 5) Charge: Based on the electrical charge on the cross-linked network, hydrogels are categorized into four classes: nonionic (neutral), ionic (cationic and anionic), zwitterionic (polybetaines), and amphoteric electrolyte (ampholytic). Nonionic hydrogels contain no charge on the polymer backbone or side groups, whereas cationic hydrogels carry positively-charged functional groups, such as thiol and amines, and anionic hydrogels consist of negatively-charged functional groups in their structures, such as carboxyl and sulfonyl.^62^ Moreover, zwitterionic hydrogels contain both cationic and anionic groups, while amphoteric ones carry both acidic and basic groups.^60^
**
Hydrogel for delivery of oncolytic viruses
Advanced hydrogel platforms for delivery
Progressions in nanotechnology and polymer sciences led to the development of “smart” hydrogels for the delivery of therapeutic agents, in which hydrogels release their cargo in response to external stimuli, instead of conventional and “dumb” hydrogels. Traditional “dumb” gels can expand or contract due to osmotic pressure; however, their responsiveness tends to be inefficient, resulting in inaccurate drug release and restricted control over dosage timing, whereas “smart” gels, known as stimuli-responsive hydrogels, are designed to react to different stimuli including magnetic fields, electromagnetic radiation, pH levels, temperature, or the existence of particular biological elements.^63^ For example, the mechanism of action of thermosensitive hydrogels is based on phase transition (from sol to gel) at the critical solution temperature in response to temperature changes. The lower critical solution temperature (LCST) and upper critical solution temperature (UCST) are major properties of thermosensitive hydrogels as they describe the phase transition of these materials on temperature change. LCST is defined as the temperature below which a thermosensitive hydrogel is soluble (in a sol state), and above the temperature were hydrophobic interactions or the collapse of the polymer chains cause the formation of a gel (gelling state). The transition from so hydrated state to a gel state is a result of the balance between the properties of hydrophilic and hydrophobic segments chemically or physically incorporated in the polymer. UCST is above the temperature where a thermosensitive hydrogel is soluble (sol state), and below which a hydrogel forms a gel due to intermolecular interactions, such as hydrogen bonding or ionic interactions.^64,65^ LCST-based systems have become popular designs in the biomedical field because their transition temperatures can be designed to match ~32-37 °C (physiological temperature).^66^ Considering the source of their composition, thermosensitive hydrogels are divides as natural biodegradable polymers, including gelatin, cellulose, and chitosan, and synthetic polymers, such as polyethylene glycol (PEG) and poly(N-isopropyl acrylamides) (PNIPAM).^65^ Owing to its LCST ~32 °C, PNIPAM remains a suitable polymer for biomedical applications.^67^ Other stimuli-responsive hydrogels are enzyme-responsive hydrogels (ERHs) that change structure in response to enzyme activities, allowing existing properties of the materials to be altered based on specific biomolecular signals.^68^ For example, if an ERH were responsive specifically to matrix metalloproteinases (MMPs), which are often overexpressed in cancer, then by using the ERH, the release of the therapeutic agent and degradation of the biomaterial could be controlled where they are both released locally because of the local overexpression of MMPs, thus enhancing efficacy of the therapeutic agent and reduced off-target effects.^69^ Enzyme sensitive hydrogels proceed a bit differently, but the primary functionality will be through site-specific degradation or controlled release of different therapeutics by using specific linkers to therapeutically active and elastomeric materials. There are primary three different modes of enzyme mediated degradation used in ERHs: (1) Matrix degradation, in which enzymes begin degrading crosslinkers causing the hydrogel to disintegrate and release the encapsulated therapeutics; (2) Cleavage of covalently attached therapeutics, either tethered by enzyme cleavage linker or chemically; where therapeutic remains attached to the hydrogel until the enzymes activate the linkers, controlled release can then occur; (3) Conformational change by altering the “swelling” or “hydrophilicity” of the hydrogel and the rates of diffusions of the drug can be imparted by the enzymatic activity.^70,71^ Stimuli-responsive hydrogels can also be classified into two groups based on response to stimuli: single-stimulus responsive hydrogels and multi-stimuli responsive hydrogels. Compared with single-stimulus responsive hydrogels, multi-stimuli responsive hydrogels have some advantages because of their capability to respond to various external stimuli at the same time or in sequence, including improved reliability owing to their higher specificity, enhanced versatility, greater sensitivity, more stable, and synergistic effects.^72^ Design strategies focus on functionalizing stimuli-sensitive moieties into polymer networks for desirable properties. Stimuli-responsive polymer networks can be generated by covalent crosslinking, using supramolecular interactions (e.g., host-guest chemistry) or creating interpenetrating polymer networks (IPNs).^73^ This results in materials with tunable response characteristics. Biocompatible responses can also be enhanced by ‘borrowing’ functions from synthetic polymers built from stimuli-responsive monomers. Typically, a polymer would have a synthetic polymer, such as PNIPAm, which serves as a thermoresponsive component, along with groups that support responses at the pH level (for example, acrylic acid) or that respond to redox (for example, disulfide bonds).^74^ Natural polymers that also serve as conductive elements, such as chitosan or hyaluronic acid, are used as the basis of a hybrid construct with multi-stimuli capabilities (e.g., fibre aniline oligomers or nanoparticles, including magnetic Fe3O4).^74,75^ More advanced constructs can be developed that use complex supramolecular assemblies built from β-cyclodextrin (β-CD) containing azobenzene or ferrocene as guests, giving rise to materials with photo- and redox-responsiveness, allowing potentially reversible sol-gel behavior.^76^ Other advanced techniques, such as layer-by-layer (LbL) assembly, enable the production of multilayer films with the potential to control pH and temperature response mechanisms.^77^
Another promising alternative to conventional hydrogels is self-healing ones. In contrast to conventional hydrogels that have restricted mechanical stability and deforming characteristics due to mechanical forces, self-healing platforms have long-term stability and good reliability because they can restore their original function, structure, and shape.^78,79^ This self-repairing feature usually depends on restoring molecular interactions in a moisture-rich microenvironment once the hydrogel has encountered external forces or harm.^78^ These hydrogels can be linked through dynamic covalent bonds or noncovalent interactions, allowing them to heal and reform via the dynamic balance between the separation and reassociation of these interactions. Upon implantation or injection, self-healing hydrogels can endure in vivo structural changes without suffering damage. Self-healing hydrogels are usually water-dense polymers characterized by a porous framework. As a result, water-soluble bioactive agents dissolve effectively in hydrogels and adhere within porous structures and release in the target tissue.^78,80^ Recent developments have carefully explored new compositions to expand functions, including functionalized chitosan-based self-healing hydrogels, which take advantage of the natural polymer’s biocompatibility and contain dynamic imine linkages for rapid healing in wound dressings.^81^ Other innovative designs include photo-regulated self-healing hydrogels with hollow nanoparticles, which can increase the modulus of the material with light so that Young’s modulus can be up to synchronous growth in tissue repair applications.^82^ Recently cellulose based hydrogels have emerged as a sustainable and tunable swelling dynamics with molecular network architectures that respond to physicochemical stimuli with numerous potential uses in delivery applications and in regenerative medicine.^83^ Developments in additional directions should address challenges in mechanical durability and specificity and position self-healing hydrogels as versatile platforms for different biomedical applications for which they could be used for targeted therapy.
Nanogels, nanoparticle-based hydrogels, are another innovative and promising advanced platform. They consist of interconnected hydrophilic polymers and water, with an average diameter of approximately 100 nm. They possess a significant water content, an extensive specific surface area, and robust stability. Nanogel-centered systems are engineered to ensure the cargo maintains an extended circulation half-life within the body and can effectively deliver it to intended sites in biomedical applications. Additionally, nanogels can be designed to respond to environmental factors; these are referred to as stimulus-responsive or environmentally responsive nanogels.^84,85^ The characteristics of the nanomaterials within the hydrogel influence the type and functionality of stimuli-responsive hydrogels. Moreover, the incorporation of nanomaterials into hydrogels enhances their injectability and shear-thinning characteristics. The porous microstructure of hydrogels and the diverse interactions between nanomaterials and hydrophobic polymer chains allow nanomaterials to influence the rheological behavior of hydrogels through distinct interactions, leading to enhanced viscoelastic properties. A proper distribution of nanomaterials within hydrogels leads to enhanced biocompatibility and improved functionality of nano-crosslinked dynamic hydrogels.^86^ Molecular architectures of nanogels can utilize dynamic crosslinking approaches to achieve tunable properties, chemical crosslinking via click chemistries (thiol-maleimide Michael additions or strain-promoted azide-alkyne cycloadditions) to form redox-degradable networks, or physical self-assembly with electrostatic interactions and hydrogen bonding via reversible structures.^87^ Many fabrications of stimuli-responsive designs have also progressed, including pH-sensitive nanogels, which use ionizable groups (carboxylic acids or amines) to induce swelling and drug release within acidic TMEs, redox-responsive nanogels utilizing disulfide bonds, which are destructed intracellularly in glutathione-rich environments, and thermo-responsive polymers, with examples using PNIPAM, which transition around body temperature to allow controlled release.^88^ As shown in the multi-stimuli designs, there are also byproducts that offer combinations of mechanisms such as pH/redox dual-responsive nanogels from hyaluronic acid crosslinked by cystamine, which execute targeted delivery of cargo while promoting on-target delivery and reducing off-target effects.^89^ New compositional innovations expand the versatility of nanogels, including natural polymers, such as hyaluronic acid, alginate, and chitosan with the intent of allowing for some biocompatibility, synthetic polymers, such as PNIPAM and PEG leading to tunable hydrophilicity, and hybrid nanogels utilizing nanomaterials, such as gold-silver-cuprous oxide nanoparticles (Au-Ag-Cu2O NPs) with potential photothermal effects.^87^ For example, nucleic acid-based nanogels, made by DNA hybridization or creating DNA origami structures, are extremely versatile, are very good at loading drugs such as siRNA and mRNA, have potential for a high cargo and their programmed structures protect against nucleases, static charge, and enable size-targeted nanoparticle methods of gene therapy.^89^ It is worth noting that using microfluidics in nanogel synthesis is one of the recent advancements in this area. Microfluidics provides a precise and powerful tool for real-time monitoring and efficient polymerization that circumvents scalability challenges and guarantees uniform particle production.^90^
Hydrogels deliver oncolytic viruses to the tumor microenvironment
Despite great attention to OVs, they need to circumvent some limitations to revolutionize the cancer treatment market. For example, OAds require high doses and repeated administration to show promising anti-cancer effects due to poor persistence of the virus in a target tissue, short duration of gene expression with therapeutic goals, and virus-specific immune responses within the host.^91,92^ As shown in Figure 3, hydrogel-based micro/nanomaterials can overcome these challenges because they protect their cargo from the host’s harsh environments and retain their cargo over an extended time in the target tissue with high concentration.^93,94^ Moreover, hydrogels provide sustained local delivery of OVs into the TME to improve therapeutic outcomes.^10,95^ Owing to its responsiveness to the TME, including matrix metalloproteinase-2 (MMP-2), MMP-9, and collagenase, Jung et al designed a gelatin-based hydrogel for sustained delivery of tumor necrosis factor-related apoptosis-inducing ligand (TRAIL)-expressing OAd (OAd-TRAIL) into the TME. They found that the stiffness of hydrogel affects the kinetics of the release of OAds, proposing that 3380-Pa gel provides a more tightly regulated (enzyme-dependent) release profile compared with 50-Pa gel. Surprisingly and in contrast to in vitro experiments, they reported that the 50-Pa gel-mediated delivery system leads to more effective release of OAd and exhibits anti-tumor activities in Syrian hamsters compared with the 3380-Pa gel. Encapsulation of OAd-TRAIL into the hydrogel system also prolongs virus persistence and enhances viral localization and accumulation into the TME due to the time-dependent degradation of the hydrogel. Moreover, the OAd-TRAIL/gel system displayed lower liver accumulation (15.4-fold), indicating lower hepatotoxicity, and reduced innate immune responses (IL-6 and TNF-α) as well as adaptive immune responses (neutralizing antibodies) against OAd.^19^ The potential reason for the inconsistency between the in vitro and in vivo results could be explained as follows: 1) Due to better accessibility of enzymes to cleavage sites and looser polymer network, MMPs may degrade softer hydrogels faster than stiff ones in vivo, which leads to burst release of OVs and potent anti-tumor immune responses in softer gels may stem from better infiltration of immune cells into the TME.^96,97^ In addition to collagenase, which was used in the in vitro conditions of this study, the TME has a complex environment with esterases, glycosidases, and proteases activities,^98^ all of which can affect the kinetics of cargo release and hydrogel degradation. This difference in heterogeneity of enzymatic activity between the TME and in vitro conditions can lead to different results. Furthermore, infiltration of immune cells occurs better in softer hydrogels,^99,100^ which degrade faster, subsequently, resulting in release of antigens, PAMPS, and DAMPs from lysed malignant cells, priming the “cold” TME to “hot” one. This rapid activation of immune responses might lead to potent anti-tumor activities in vivo. In another study, Le et al developed a dual temperature- and pH-responsive physically cross-linked hydrogel-based structure for long-term and efficient delivery of OAd. This system rapidly formed a gel at the TME or body condition, whereas it was in sol form at room temperature and pH = 9. The sol/gel transition of the polyurethanes (PUSMA)-based hydrogel can allow it to be injectable for delivery purposes. The physically cross-linked hydrogel protected OAds from the environment and retained their anti-tumor therapeutic effects for a long time compared to naked OAds, leading to robust cytotoxicity against malignant cells even for 11 days.^101^ In addition to the temperature- and pH-responsive hydrogels, redox-responsive hydrogels have also been designed for OV delivery in which crosslinking based on disulfide bonds could be cleaved by high concentrations of glutathione (GSH), a reduction agent, at the intracellular or tumor region. In this regard, Deng et aldesigned a nano-dimensional redox-responsive hydrogel, 300-400 nm in diameter and -13 mV zeta potential, for the encapsulation and delivery of two model OVs, echovirus Rigvir® ECHO-7 (RNA virus) and Ad [I/PPT-E1A] (DNA virus), and to protect them against circulatory antibodies. The redox-responsive OVs/nanohydrogel systems not only maintained stability in normal physiologic conditions, but also provided the controlled release of OVs and induced cell lysis of malignant cells.^102^
**
Hydrogel micro/nanostructures also facilitate combinational therapy using OVs and other therapeutic agents. During the treatment profile, high-dose repeated administration of both OVs and therapeutic agents is applied to compensate for their inactivation, proposing the development of co-delivery systems, such as hydrogel, to conquer these limitations. To prolong and enhance the therapeutic ability of OAd armed with IL-12 and IL1-5 (CRAd-IL12-IL15) and cytokine-induced killer (CIK) cells in a single local injection, Du et al encapsulated both therapeutic agents into a gelatin-based hydrogel. The CRAd-IL12-IL15 + CIKs/gelatin structure not only reduced the spreading of high-dose OAds and CIK cells from the vaccination site to the non-target tissues, such as the liver, but also attenuated immune responses against Ad and maintained sustained release of both therapeutic agents.^103^ Another study combined IL-12 and GM-CSF-expressing OAd with DCs using a biodegradable hydrogel to ameliorate immunosuppressive TME and impede their rapid inactivation and dissemination. Compared with OAd + DCs or a single treatment, the OAd + DC/gel system (1 × 10^10^ VP and 1 × 10^6^ DC cells) activated both exogenous and endogenous DCs and enhanced their infiltration into draining lymph nodes. Additionally, the OAd + DC/gel system increased the number of tumor-specific IFN-γ-secreting immune cells and presented considerably greater tumor growth inhibition than the OAd + DC-vaccinated group. These beneficial results of the OAd + DC/gel system returns to higher population of OAds and DCs within the TME owing to release kinetics which prolonged intratumoral retention of both therapeutic agents. Retention of OAds and DCs by the hydrogel system in the tumor tissue augments the level of cytokines and finally increases infiltration of immune cells and augments DCs maturation.^104^ In hydrogel-based delivery platforms, especially in co-delivery systems, determining a release profile for achieving an ideal therapeutic advantage is a major challenge. The development of mathematical models, such as ordinary differential equations (ODEs), could be helpful in predicting and optimizing treatment protocols as well as determining optimal doses and schedules.^105-107^ ODE models simulate the multifaceted interactions of therapeutic agents with tissues and cells to determine the effects of treatment on cells, tumor growth, personalized medicine, immune cell responses, immune evasion, resistance management, and treatment schedule.^108,109^ Indeed, ODE models use temporal dynamics of cell population and response to treatment for representing the rate of change over time.^110^ In this regard, Jenner et al used a mathematical model (ODEs) to optimize the release profile in combinational therapy (OAd and immature DCs) loaded onto a hydrogel system in interaction with immune cells and tumor cells. Their modeling revealed that (1) different immune and virus characteristics are tumor cell-specific, (2) the division of resources between anti-viral and anti-tumor immune responses potentiates fighting against tumors in combinational treatments, (3) the significantly reduced tumor volume stems from an initial burst release of OAd from the hydrogel delivery system, which infects and stimulates an immune response, followed by a sustained constant release of DCs, and (4) additional complexity in the hydrogel-release profile is not vital for any improvement in the treatment outcome. In this model, they included the release of both OVs and immature DCs as well as the roles of uninfected malignant cells in stimulating immune cells. The final ODE system is as follows:
-
𝑑𝑈/𝑑𝑡 = 𝑟 log (𝐿/𝑈)𝑈 – 𝛽𝑈𝑉/𝑇−𝜅𝐾𝑈/𝑇,
-
𝑑𝐼/𝑑𝑡 = 𝛽𝑈𝑉/𝑇 − 𝑑_𝐼_𝐼 – 𝜅𝐾𝐼/𝑇,
-
𝑑𝑉/𝑑𝑡 = 𝑢_𝑉_(𝑡) − 𝑑_𝑉_𝑉 + 𝛼𝑑_𝐼_𝐼,
-
𝑑𝐷_𝑆_/𝑑𝑡 = (1−𝑓)𝑢_𝐷𝐶_ (𝑡) – 𝑠_𝐴𝑈_𝐷_𝑆_𝑈 − 𝑠_𝐴𝐼_𝐷_𝑆_𝐼 − 𝑑_𝑆_𝐷_𝑆_,
-
𝑑𝐷_𝐿_/𝑑𝑡 = 𝑓𝑢_𝐷𝐶_ (𝑡) −𝑠_𝐴𝑈_𝐷_𝐿_𝑈 − 𝑠_𝐴𝐼_𝐷_𝐿_𝐼 − 𝑑_𝐿_𝐷_𝐿_,
-
𝑑𝐴_𝐼_/𝑑𝑡 = 𝑟_𝐴𝐼_𝐼 − 𝑠_𝐴𝑈_𝐴_𝐼_𝑈 − 𝑠_𝐴𝐼_𝐴_𝐼_𝐼 – 𝑑_𝐴𝐼_𝐴_𝐼_,
-
𝑑𝐴_𝑀_𝑑𝑡 = 𝑠_𝐴𝑈_𝑈 (𝐴_𝐼_ + 𝐷_𝐿_ + 𝐷_𝑆_) + 𝑠_𝐴𝐼_𝐼 (𝐴_𝐼_ + 𝐷_𝐿_ + 𝐷_𝑆_) − 𝑑_𝐴_𝐴_𝑀_,
-
𝑑𝐻/𝑑𝑡 = 𝑠_𝐻_𝐴_𝑀_ − 𝑑_𝐻_𝐻,
-
𝑑𝐾/𝑑𝑡 = 𝑠_𝐾𝐻_𝐻 + 𝑠_𝐾𝐴_𝐴_𝑀_ − 𝑑_𝐾_𝐾.
where t is time (days); U and I are the uninfected and infected tumor cells, respectively; V is free virus particles; DS and DL are short-lived and long-lived immature DCs, respectively; AI and AM are immature and mature APCs, respectively; K is killer T-cell, and H is helper T-cell. Furthermore, they presented the 𝑇 = 𝑈 + 𝐼 + 𝐷_𝐿_ + 𝐷_𝑆_ + 𝐴_𝐼_ + 𝐴_𝑀_ + 𝐻 + 𝐾 equation for the total cell [population within the TME.^111^
To overcome immunosuppressive TME, Zhuang et al co-loaded an oncolytic HSV-1 (1 × 10^7^ pfu) and Navoximod (120 μg), an indoleamine 2, 3-dioxygenase 1 (IDO1) inhibitor, into 2% silk-hydrogels (V-Navo@gel). In the V-Navo@gel system, the intratumoral injection of hydrogel reduces the toxicity of the oncolytic HSV-1 by restricting the virus dissemination. Furthermore, the upregulation of IDO1 is inhibited by the release of Navoximod from the V-Navo@gel, leading to the reshaping and reversal of immunosuppressive TME and inhibition of tumor growth.^112^ While the clinical translation of such a system holds enormous promise, its challenges include the scale-up production of the GMP-grade silk hydrogels and the variability of the TME composition and expression of IDO1 from one patient to another. Future research could enhance specificity by functionalizing the silk fibroin polymer with targeting ligands such as RGD (arginine-glycine-aspartic acid) peptides. In addition to providing scaffolds for OVs and cancer immunotherapy approaches, hydrogels facilitate the co-encapsulation and delivery of OVs with other tumoricidal agents. For instance, Qiao et al assessed the anti-tumor effects of injectable pH-degradable polyvinyl alcohol (PVA) microgels co-encapsulated with OAd and bromodomain and extra-terminal (BET), JQ1, using microfluidics. The cargos of the PVA microgel were released due to cleavage of vinyl ether acrylate (VEA)-functionalized PVA in a mildly acidic environment and the co-loaded microgel exhibited significant cytotoxicity against A549 lung cancer cells. Furthermore, the addition of JQ1 treatment to OAd in microgels enhanced the Ad replication in vivo and reversed the immune suppression by inhibiting PD-L1 expression, leading to tumor inhibition.^15^ It is worth noting that OV-loading hydrogel beads and its combination with transcatheter arterial embolization (TAE) is a sufficient approach for targeting malignant cells. In this combinational approach, OV-loading hydrogel beads act as an effective embolic system for transcatheter arterial viroembolization (TAVE) in the treatment of hepatocellular carcinoma. Also, it provides sustained release of OVs for an extended period and prevents virus accumulation within normal tissues.^113^
Conclusion
OVs, as preferentially lysing tumor cell agents, have gained accumulating attention due to promising therapeutic potential in (pre)clinical studies. Nevertheless, their anti-tumor activity is hindered by various factors, including non-specific targeting in systematic delivery, neutralization by pre-existing antibodies, immunosuppressive TME, and physical barriers. To address these limitations, different delivery systems have been developed. Among them, hydrogels have unique advantages that make them more appealing, such as biodegradability, biocompatibility, the ability to respond to multiple stimuli, high loading capacities, and low toxicity. Compared with other delivery platforms, such as nanoparticles and liposomes, OV delivery using hydrogels presents several advantages. In contrast to nanoparticles and liposomes that are suitable for systemic delivery, hydrogels represent another class of effective local (intratumoral) or sustained delivery approaches, mainly because they have the potential for depot formation that underpins sustained, high-concentration local delivery for long periods of time with minimal systemic exposure and systemic toxicities. This is especially beneficial for unresectable solid tumors or for local treatment in the resection cavity to minimize recurrence. However, some serious considerations must be resolved before the translation of these studies to clinical practices.
*1) Absence of clinical trials for OV-hydrogel systems: *We affirm that there are no clinical trials reported, to the best of our knowledge, for a combination of OV-hydrogel as a reliable therapeutic strategy of cancer. The reason is that this field is relatively new and both modifying the biological (virus) and making changes to the delivery system (hydrogel) have regulatory challenges. To strengthen our claims regarding the hydrogel delivery system overcoming limitations of OVs, clinical trials are the critical next step required to validate these preclinical findings in humans. It is worth noting that hydrogel applications in other therapeutic contexts, including drug delivery systems, tissue engineering and regenerative medicine, vaccine adjuvants, and immunotherapy, depicts the established clinical safety and utility of hydrogels in clinical trials, contextualizing the potential of OV-hydrogel system to translate into clinical practices. 2) Safety and biocompatibility concerns: Since most studies evaluated the pharmacokinetics of hydrogels and OV-carrying hydrogels in experimental environments and animal models, more careful analyses and precise characterizations are required for transferring these applications to human studies. The lack of clinical trials may lead to safety and biocompatibility considerations in the future. For instance, the byproducts of hydrogel degradation or the hydrogel materials themselves could elicit host immune responses, local inflammation, fibrosis, and toxicity, leading to reduced therapeutic efficacy. Controlling the degradation rate of hydrogels is also another important factor in eliciting immune responses. Too fast degradation can result in insufficient delivery of cargo, while too slow a degradation rate can augment inflammatory responses and fibrous encapsulation. These issues highlight the necessity of selecting biocompatible materials to minimize side effects and immune responses during long-term use. In this regard, using generally recognized as safe (GRAS) materials or materials such as gelatin, chitosan, and hyaluronic acid, whose biocompatibility is well established, could reduce side effects. Although the bioactivity and biodegradability of natural polymers give them an advantage over synthetic polymers, control over purity with stringent quality control during manufacturing and chemical modification can reduce their immunogenicity and allergenicity. 3) Manufacturing, scalability, and translational hurdles: Other challenges in the OV-hydrogel system are manufacturing as well as translational hurdles. Maintaining batch-to-batch consistency under Good Manufacturing Practice (GMP) conditions and difficulties in scaling up hydrogels and OV-loading hydrogels, in addition to challenges of the sterilization process of biomaterials without affecting their structure and functions, are required to be addressed in future research to facilitate the translation of the OV-hydrogel system to clinical trials. During industrialization, large-scale production is a complex process that requires confirming the consistency of material properties and incorporating bioactive agents into the hydrogel system. 4) Cost and regulatory complexity: The complex synthesis process and potentially high cost of raw biomaterials, besides the multifaceted processes of combining two distinct tools, hydrogel as a synthetic material and OV as a biological agent, require complex regulatory landscapes and safety testing. The future considerations should aim to eliminate cost through scalable, inexpensive alternatives such as alginate or scaled automated production platforms such as 3D bioprinting, that lessen labor and material costs. Regulatory simplification could take the form of creating standardized testing methods for hybrid systems, or providing similar use regulatory fast-track programs to orphan indications, assuring hydrogel-OV treats have a high economic viability and attain clinically navigable approval. 5) Hydrogel design optimization: The determination of the hydrogel degradation rate and the factors that affect this parameter, such as hydrogel stiffness and cross-linking mode, will help to design more controllable micro/nanostructures to deliver OVs to tumor sites. Furthermore, modeling their release profile and targeting moieties could be helpful in achieving an ideal and personalized nano-delivery system for OVs using hydrogels. In this regard, machine learning (ML) and artificial intelligence (AI) models can analyze and predict the dynamics of both anti-tumor (e.g., CTLs) and anti-viral (e.g., neutralizing antibodies and NK cells) immune responses, the rate of tumor cell infection and lysis, the OV release kinetics and the hydrogel degradation rate. Analyzing both in vitro and in vivo results and predicting both OV and hydrogel behavior in the body using ML and AI models could accelerate the design of optimized OV-hydrogel formulations for personalized cancer therapy. Additionally, ML and AI could deal with the issues related to scalability and reproducibility by optimizing fabrication processes and material formulations. Taken together, interdisciplinary collaboration among genetic engineering, bioengineering, material science, computational modeling, and chemistry as well as long-term behavior of hydrogels could bridge the gaps and introduce the hydrogel system as an encouraging candidate for delivery of OVs and circumvent their limitations.
Competing Interests
The authors declare no conflict of interest.
Data Availability Statement
No data was used for the research described in the article.
Ethical Approval
Not applicable.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hill C Carlisle R Achieving systemic delivery of oncolytic viruses Expert Opin Drug Deliv 20191666072010.1080/17425247.2019.161726931144549 · doi ↗ · pubmed ↗
- 2Najafi M Hashemi Goradel N Farhood B Salehi E Solhjoo S Toolee H Tumor microenvironment: interactions and therapy J Cell Physiol 2019234557002110.1002/jcp.2742530378106 · doi ↗ · pubmed ↗
- 3Chen DS Mellman I Elements of cancer immunity and the cancer-immune set point Nature 201754176373213010.1038/nature 2134928102259 · doi ↗ · pubmed ↗
- 4Ghanaat M Hashemi Goradel N Arashkia A Ebrahimi N Ghorghanlu S Veisi Malekshahi Z Virus against virus: strategies for using adenovirus vectors in the treatment of HPV-induced cervical cancer Acta Pharmacol Sin 2021421219819010.1038/s 41401-021-00616-533633364 PMC 8633276 · doi ↗ · pubmed ↗
- 5Chen L Ma Z Xu C Xie Y Ouyang D Song S Progress in oncolytic viruses modified with nanomaterials for intravenous application Cancer Biol Med 202320118305510.20892/j.issn.2095-3941.2023.027538009779 PMC 10690878 · doi ↗ · pubmed ↗
- 6Hemminki O Dos Santos JM Hemminki A Oncolytic viruses for cancer immunotherapy J Hematol Oncol 20201318410.1186/s 13045-020-00922-132600470 PMC 7325106 · doi ↗ · pubmed ↗
- 7Frampton JE Teserpaturev/G 47Δ: first Approval Bio Drugs 20223656677210.1007/s 40259-022-00553-736098872 · doi ↗ · pubmed ↗
- 8Hashemi Goradel N Baker AT Arashkia A Ebrahimi N Ghorghanlu S Negahdari B Oncolytic virotherapy: challenges and solutions Curr Probl Cancer 202145110063910.1016/j.currproblcancer.2020.10063932828575 · doi ↗ · pubmed ↗