Epidemiological trends in enamel hypomineralisation and molar-incisor hypomineralisation: a systematic review and meta-analysis
Nour Ammar, Karl-Ferdinand Fresen, Falk Schwendicke, Jan Kühnisch

TL;DR
This paper updates a meta-analysis on enamel hypomineralisation, adding a previously missed North American study, but finds no major changes in global prevalence.
Contribution
The addition of a previously omitted North American study to a large meta-analysis on enamel hypomineralisation.
Findings
The global prevalence of MIH remains at 0.155 (95% CI: 0.144–0.166) after including the new study.
The North American MIH prevalence slightly decreased from 0.239 to 0.223 after adding the new study.
The new study did not alter the overall conclusions of the meta-analysis.
Abstract
Recently, the systematic review and meta-analysis “Epidemiological Trends in Enamel Hypomineralisation and Molar-Incisor Hypomineralisation: A Systematic Review and Meta-Analysis” was published in Clinical Oral Investigations. In 2025 a reader brought the omission of an epidemiological study from North America to the attention of the author group. After checking the eligibility for inclusion we aimed at updating the meta-analysis. After inclusion of this overlooked study the systematic review and meta-analysis covers 139 studies and data from a total of 199,999 participants. For North America, the MIH prevalence estimate decreased slightly from 0.239 (95% CI: 0.144–0.334) to 0.223 (95% CI: 0.140–0.306). Notably, the global prevalence estimate for MIH remained unchanged at 0.155 (95% CI: 0.144–0.166). The addition of the overlooked study influenced slightly the MIH outcome for North…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
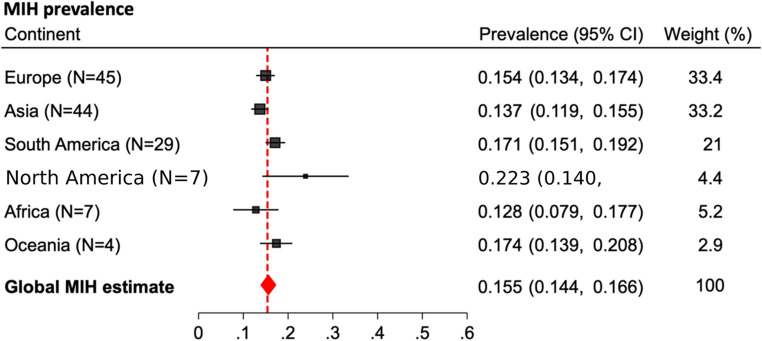 Figure 1
Figure 1- —Klinikum der Universität München (6933)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone and Dental Protein Studies · Forensic Anthropology and Bioarchaeology Studies · dental development and anomalies
Introduction
Recently, a reader [1] of the above mentioned systematic review and meta-analysis [2] draw attention to the omission of a key U.S. epidemiological study [3] that meets the review’s inclusion criteria and provides nationally relevant data. This study involved an American cohort and reported MIH prevalence and diagnostic criteria consistent with the methods applied by Ammar et al. [2]. Its inclusion could have strengthened the North American dataset, potentially altering the pooled estimates reported by the mentioned study. The study had a standardized clinical examination protocol, conducted by a single calibrated examiner using both the Modified Developmental Defects of Enamel (DDE) Index and the European Academy of Pediatric Dentistry (EAPD) criteria.
We thank Dr. Tagelsir Ahmed and the editors of Clinical Oral Investigations for bringing an overlooked study to our attention. The study by Tagelsir Ahmed et al. [3] was erroneously excluded during the duplicate removal step of the initial review. We have reviewed the study and deemed it eligible for inclusion. Therefore, we aimed at updating the corresponding data in the meta-analysis.
Results
The meta-analysis results have been updated in the attached table 1 and figure 1. The missing study presented data from a cohort of 337 children aged from 6 to 15 years old and influenced the calculations for North America (Table 1 and Figure 1). The meta-analysis now includes 139 studies and data from a total of 199,999 participants. For North America, the MIH prevalence estimate decreased slightly from 0.239 (95% CI: 0.144–0.334) to 0.223 (95% CI: 0.140–0.306). The forest plot for the presentation of global MIH prevalence was corrected accordingly (Figure). With an updated total number of seven studies from North America, it remains the continent with the highest reported MIH prevalence. Notably, the global prevalence estimate for MIH remained unchanged at 0.155 (95% CI: 0.144–0.166).
Conclusion
Consequently, the addition of the overlooked study influenced slightly the MIH outcome for North America but had no impact on the previously drawn conclusions.
Table 1. Corrected meta-analysis results for the MIH prevalence in North AmericaContinentCountryEH PrevalenceMIH PrevalenceM + IH PrevalenceNorth America (N = 7)United States of America (N = 2)0.109 (0.086–0.132)0.051 (0.033–0.078)Mexico (N = 5)0.268 (0.161–0.374) North America estimate
0.223 (0.140–0.306) 0.051 (0.033–0.078)Global estimate 0.253 (0.200–0.306)
0.155 (0.144–0.166)
0.069 (0.060–0.077)
Fig. 1. Corrected forest plot for the subgroup analyses of MIH prevalence per continent