Leptospirosis Incidence at Four Sites in Sub-Saharan Africa and South East Asia: An International Multi-Site Hybrid Surveillance Study
John A Crump, Mathieu Picardeau, Sara A Ajanovic, John Bradley, Justina M Bramugy, Mabvuto Chimenya, Edward W Green, Sham Lal, David C W Mabey, Mayfong Mayxay, Paul N Newton, Ioana D Olaru, Heidi Hopkins, Christian Bottomley, Benjamin Amos, Benjamin Amos, Elizabeth A Ashley

TL;DR
This study estimates leptospirosis incidence in four countries, showing high rates in Laos, Malawi, and Mozambique, highlighting the need for more data to improve global disease burden estimates.
Contribution
The study provides new leptospirosis incidence estimates from under-researched sites in Sub-Saharan Africa and South East Asia.
Findings
Leptospirosis incidence was highest in Laos and Malawi, with rates of 1302 and 1337 per 100,000 population per year.
Mozambique had a lower but still significant incidence rate of 187 per 100,000 population per year.
Incidence estimates from pre-COVID years were similar to the overall study period, indicating consistent trends.
Abstract
There are few leptospirosis incidence studies despite such estimates being central to accurate burden of disease estimation. We used data from the multicenter Febrile Illness Evaluation in a Broad Range of Endemicities (FIEBRE) study to make leptospirosis incidence estimates from new sites. Febrile patients aged ≥2 months in Laos, Malawi, Mozambique, and Zimbabwe were enrolled and underwent standardized clinical and exposure assessment. Acute and convalescent sera were tested by Leptospira microscopic agglutination test and acute plasma by lfb1 polymerase chain reaction (PCR). Participants with ≥4-fold rise in antibody titer between acute and convalescent sample, or Leptospira PCR positive for the lfb1, had confirmed leptospirosis. Leptospirosis incidence was estimated after adjusting for incomplete enrollment of febrile patients, availability of paired sera, and use of study…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
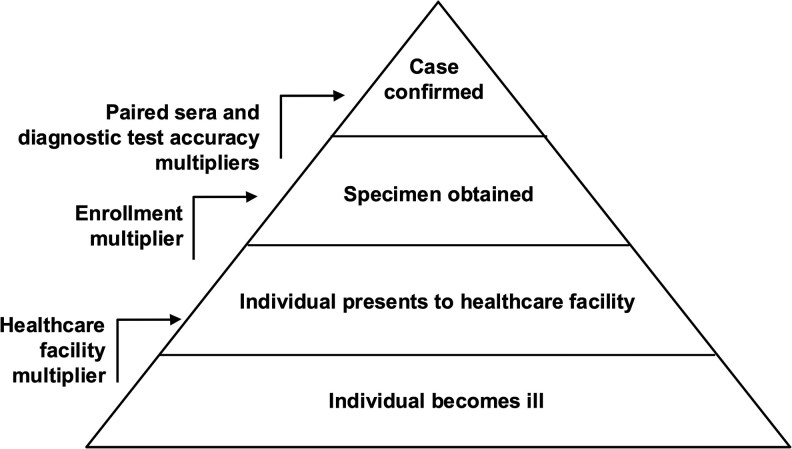 Figure 1
Figure 1| Laos, | Malawi, | Mozambique, | ||||
|---|---|---|---|---|---|---|
|
| (%) |
| (%) |
| (%) | |
| Age group, years | ||||||
| 0–4 | 54/485 | (11.1) | 218/906 | (24.1) | 186/568 | (32.7) |
| 5–14 | 131/485 | (27.0) | 179/906 | (19.8) | 116/568 | (20.4) |
| ≥ 15 | 300/485 | (61.9) | 509/906 | (56.2) | 266/568 | (46.8) |
| Sex | ||||||
| Female | 240/485 | (49.5) | 559/908 | (61.6) | 367/570 | (64.4) |
| Male | 245/485 | (50.5) | 349/908 | (38.4) | 203/570 | (35.6) |
| HIV-1/2 status | ||||||
| Uninfected | 0/0 | NAN | 628/710 | (88.5) | 486/566 | (85.9) |
| Infected | 0/0 | NAN | 82/710 | (11.5) | 80/566 | (14.1) |
| Malaria RDT result | ||||||
| Negative | 485/485 | (100) | 747/858 | (87.1) | 569/570 | (99.8) |
| Positive | 0/485 | (0) | 111/858 | (12.9) | 1/570 | (0.2) |
| Confirmed Leptospirosis | Tested | Enrolled | Fever | Seek Care | Study Population | Months | Person Years | Rate | (95% CI) | |
|---|---|---|---|---|---|---|---|---|---|---|
| ( | ( | ( | ( | ( | (Y) | |||||
| Laos | ||||||||||
| ≥15 yrs | 68 | 730 | 1212 | 11 226 | 0.35 104/300 | 115 080 | 25 | 239 750.00 | 1246 | (947, 1640) |
| <15 yrs | 10 | 236 | 760 | 5741 | 0.23 43/185 | 53 336 | 25 | 111 116.67 | 952 | (491, 1845) |
| All | 78 | 966 | 1972 | 16 967 | 0.3 147/485 | 168 416 | 25 | 350 866.67 | 1302 | (1,011, 1677) |
| Malawi | ||||||||||
| ≥15 yrs | 17 | 629 | 821 | 37 492 | 0.93 473/509 | 23 649 | 27 | 53 210.25 | 2048 | (1,280, 3276) |
| <15 yrs | 4 | 640 | 952 | 40 142 | 0.93 373/399 | 19 116 | 29 | 46 197.00 | 584 | (220, 1552) |
| All | 21 | 1269 | 1773 | 77 634 | 0.93 846/908 | 42 765 | 29 | 103 348.75 | 1337 | (874, 2044) |
| Mozambique | ||||||||||
| ≥15 yrs | 5 | 642 | 1021 | 3503 | 0.12 32/266 | 128 379 | 24 | 256 758.00 | 89 | (35, 226) |
| <15 yrs | 2 | 549 | 1161 | 11 101 | 0.07 21/302 | 90 471 | 28 | 211 099.00 | 274 | (65, 1160) |
| All | 7 | 1191 | 2182 | 14 604 | 0.09 53/568 | 218 850 | 28 | 510 650.00 | 187 | (85, 409) |
| Confirmed Leptospirosis | Tested | Enrolled | Fever | Seek Care | Study Population | Months | Person Years | Rate | (95% CI) | |
|---|---|---|---|---|---|---|---|---|---|---|
| ( | ( | ( | ( | ( | (Y) | |||||
| Laos | ||||||||||
| ≥15 yrs | 50 | 520 | 890 | 7842 | 0.35 104/300 | 115 080 | 15 | 143850 | 1498 | (1103, 2035) |
| <15 yrs | 4 | 160 | 538 | 3141 | 0.23 43/185 | 53 336 | 15 | 66670 | 512 | (188, 1397) |
| All | 54 | 680 | 1428 | 10983 | 0.3 147/485 | 168 416 | 15 | 210520 | 1381 | (1033, 1846) |
| Malawi | ||||||||||
| ≥15 yrs | 16 | 580 | 715 | 24471 | 0.93 473/509 | 23 649 | 18 | 35473 | 2046 | (1261, 3320) |
| <15 yrs | 4 | 598 | 831 | 21078 | 0.93 373/399 | 19 116 | 18 | 28674 | 529 | (199, 1406) |
| All | 20 | 1178 | 1546 | 45549 | 0.93 846/908 | 42 765 | 18 | 64147 | 1296 | (839, 2002) |
| Mozambique | ||||||||||
| ≥15 yrs | 2 | 301 | 441 | 1576 | 0.12 32/266 | 128 379 | 10 | 106982 | 82 | (20, 339) |
| <15 yrs | 1 | 327 | 705 | 7642 | 0.07 21/302 | 90 471 | 14 | 105549 | 316 | (43, 2335) |
| All | 3 | 628 | 1146 | 9218 | 0.09 53/568 | 218 850 | 14 | 255325 | 192 | (60, 612) |
| Confirmed Leptospirosis | Tested | Enrolled | Fever | Seek Care | Population | Months | Person Years | Rate | (95% CI) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ( | ( | ( | ( | ( | ( | (Y) | |||||
| Laos | |||||||||||
| ≥15 yrs | 68 | 53 | 730 | 1212 | 11 226 | 0.35 104/300 | 115 080 | 25 | 239 750.00 | 971 | (681, 1384) |
| <15 yrs | 10 | 17 | 236 | 760 | 5741 | 0.23 43/185 | 53 336 | 25 | 111 116.67 | 1618 | (298, 8792) |
| All | 78 | 70 | 966 | 1972 | 16 967 | 0.3 147/485 | 168 416 | 25 | 350 866.67 | 1168 | (825, 1654) |
| Malawi | |||||||||||
| ≥15 yrs | 17 | 0 | 629 | 821 | 37 492 | 0.93 473/509 | 23 649 | 27 | 53 210.25 | 0 | (0, 361) |
| <15 yrs | 4 | 0 | 640 | 952 | 40 142 | 0.93 373/399 | 19 116 | 29 | 46 197.00 | 0 | (0, 438) |
| All | 21 | 0 | 1269 | 1773 | 77 634 | 0.93 846/908 | 42 765 | 29 | 103 348.75 | 0 | (0, 191) |
| Mozambique | |||||||||||
| ≥15 yrs | 5 | 0 | 642 | 1021 | 3503 | 0.12 32/266 | 128 379 | 24 | 256 758.00 | 0 | (0, 53) |
| <15 yrs | 2 | 0 | 549 | 1161 | 11 101 | 0.07 21/302 | 90 471 | 28 | 211 099.00 | 0 | (0, 411) |
| All | 7 | 0 | 1191 | 2182 | 14 604 | 0.09 53/568 | 218 850 | 28 | 510 650.00 | 0 | (0, 80) |
- —Febrile Illness Evaluation in a Broad Range of Endemicities
- —Wellcome Trust10.13039/100010269
- —London School of Hygiene & Tropical Medicine10.13039/100009660
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLeptospirosis research and findings · Zoonotic diseases and public health · Burkholderia infections and melioidosis
Leptospirosis was estimated to cause 1.03 million illnesses, 58 900 deaths, and to account for 2.90 disability adjusted life years in 2010 [1, 2]. High quality studies of leptospirosis incidence are needed to improve burden of disease estimates for leptospirosis that in turn inform resource allocation for diagnosis, treatment, and prevention. However, there are few studies of leptospirosis incidence worldwide [1] and data are particularly limited for African countries [3, 4]. Leptospirosis is difficult to distinguish from other causes of febrile illness clinically [5], and reference standard laboratory diagnosis relies on microscopic agglutination testing of paired sera, nucleic acid amplification tests, and bacterial isolation, techniques each with practical diagnostic limitations and that are not widely available in low-resource endemic areas [6].
Active, population-based surveillance studies have traditionally been used to measure infectious disease incidence, ideally achieved by visiting every household in a defined population regularly to identify those with the clinical syndrome of interest and to collect diagnostic specimens from those affected in the home or to actively refer individuals for testing. Such studies are complex and highly resource intensive. Hybrid surveillance methods, also known as multiplier studies, were developed more than 20 years ago to provide a less resource intensive means to estimate the incidence of acute infectious diseases [7]. Such studies adjust data from sentinel surveillance sites using multipliers to address under-ascertainment, including those derived from healthcare utilization surveys that account for illnesses not presenting to the sentinel sites [7, 8]. The Febrile Illness Evaluation in a Broad Range of Endemicities (FIEBRE) study sought to describe treatable and preventable causes of febrile illness using reference standard diagnostics among inpatients and outpatients at multiple sites with few or no data on causes of fever [9]. Thus, FIEBRE made reference standard leptospirosis diagnostics available and used a standardized diagnostic approach that allow for comparison between study sites. In addition, FIEBRE enrolled community controls that also provided data on healthcare utilization from the catchment populations of sentinel sites to estimate disease incidence using hybrid surveillance methods.
To estimate the incidence of leptospirosis at study sites in the FIEBRE study, we undertook a secondary analysis of the FIEBRE study using data from participants with confirmed lepospirosis and from community healthcare utilization surveys to adjust for under-ascertainment of confirmed leptospirosis at healthcare facilities. Our goal was to provide leptospirosis incidence estimates from locations without such estimates to strengthen evidence to inform resource allocation for disease diagnosis, treatment, and prevention.
METHODS
The overall design of the FIEBRE study and findings on leptospirosis prevalence and risk factors at FIEBRE sites have been described in detail elsewhere [9, 10]. A brief summary is provided below, including detailed methods for the present analysis.
Study Sites
The FIEBRE study was conducted at sites four countries selected for having little or no published data on causes of fever and substantial between-site variation in the prevalence of HIV-1/2 and malaria. The sites were Phonghong Vientiane Provincial Hospital, Lao People's Democratic Republic (Lao PDR); Chikwawa District Hospital, Malawi; Manhiça District Hospital, Mozambique; and Sally Mugabe Central Hospital, Parirenyatwa Hospital, Chitungwiza General Hospital, and three primary care clinics in Harare, Zimbabwe.
Enrollment, Data Collection, and Sample Collection for Febrile Participants
Febrile outpatients and inpatients aged ≥2 months were eligible for enrollment if they had a tympanic or axillary temperature of ≥37.5°C at presentation, and had not been hospitalized or undergone surgery in the previous month. Outpatients were eligible if they resided within the defined catchment area around the health facility at the time of enrollment [9]. For outpatients aged ≥15 years, those with symptoms of lower respiratory infection or of diarrheal disease were excluded. For outpatients aged ≥2 months to <15 years, those with symptoms of diarrheal diseases were excluded. Demographic information, a standardized clinical and exposure history and physical examination was performed on all consented participants and recorded on a case report form.
Whole and EDTA blood were collected on day 0, the day of enrollment, and participants were asked to return on day 28 (acceptable follow-up range: 26–48 days) for collection of convalescent whole blood. Serum and plasma were separated, aliquoted, and stored at −70°C. Samples were shipped on dry ice to the London School of Hygiene and Tropical Medicine, London, United Kingdom, for onward distribution to reference laboratories.
Laboratory Methods
Leptospira Serology
At the Unité Biologie des Spirochètes, French National Reference Center for Leptospirosis, WHO Collaborating Center for Reference and Research on Leptospirosis, Institut Pasteur, Paris, France, acute and convalescent serum was first screened by Leptospira fainei serovar Hurstbridge IgM ELISA [11, 12]. Serum from participants that screened positive by ELISA on the acute or convalescent sample proceeded for the Leptospira standard microscopic agglutination test (MAT). The MAT panels were based on the World Health Organization recommended list of globally representative reference Leptospira strains [13] adjusted to incorporate African and Asian regional isolates (Supplementary Appendix 1) [14].
Leptospira Nucleic Acid Amplification Testing and Speciation
Acute plasma from all participants was tested by polymerase chain reaction (PCR) to the lfb1 pathogenic Leptospira target [15]. Among samples positive by Leptospira lfb1 PCR, PCR products were sequenced for Leptospira speciation using established methods [16].
Case Definitions
We restricted this analysis to participants with rigorously defined confirmed leptospirosis who resided in the study catchment areas [17, 18]. We defined confirmed acute leptospirosis as a participant with paired sera with seroconversion or a ≥ 4-fold rise in MAT antibody titer between acute and convalescent sample, or a participant with paired serum and an acute plasma sample positive by Leptospira PCR for the lfb1 gene target.
Estimating the Population of Febrile Patients Presenting to Study Facilities
The number of patients presenting with fever to each of the FIEBRE study healthcare facilities was recorded throughout the study period, or estimated from a random sample of calendar days during the study period. This population of febrile patients allowed estimation for each study site of the proportion of eligible patients enrolled into the study.
Healthcare Utilization Survey
At each site we sought to enroll ≥600 control participants. Control participants were community members in the study site health facilities’ catchment areas, frequency matched one control to two cases to participating outpatients by month of enrollment, age, gender, and geographical location of residence to the outpatients. Potential control participants were approached at their place of residence by study staff with assistance from established community health workers, and enrolled if they or their parent or guardian provided informed consent.
In addition to collection of basic demographic data from control participants, study staff administered questionnaires to capture representative data about healthcare and treatment seeking (Supplementary Appendix 2). Consistent with convention for hybrid surveillance studies [19–21], the control participant, or healthcare decision-maker if the participant was a child, was asked about current and recent fever and care seeking practices for each household member in the event of fever of three or more days duration. The healthcare utilization survey provided an estimate of the proportion of individuals in the community who would present to the study enrollment sites for care in the event of fever of three or more days duration. The fraction of people with fever presenting to a study site was used to estimate the population-based incidence of fever overall, and the incidence of specific causes of fever, in the catchment area of study healthcare facilities.
Derivation of Multipliers
Enrollment Multiplier
The enrollment multiplier was calculated by dividing the number of febrile patients presenting to the study site by the number of participants enrolled .
Paired Sera Multiplier
The paired sera multiplier was calculated by dividing the number of participants enrolled in the study by the number with paired sera tested by Leptospira MAT and acute plasma PCR .
Diagnostic Test Accuracy
In the primary analysis we assumed 100% test sensitivity and specificity as Leptospira MAT on paired sera is considered to be the reference standard serologic test for leptospirosis. In a sensitivity analysis, we assumed instead a sensitivity of 93.8% and specificity of 97.3% based on published data on Leptospira MAT diagnostic test accuracy [22].
Health Facility Multiplier
The health facility multiplier was calculated using responses to healthcare utilization survey questions relating to health-care seeking behavior of the control participant in the event of febrile illness by site healthcare facility. The question was “If you [the control] had a fever that lasted three or more days, where would you usually seek care?’ and “For a fever lasting more than three days, where would you usually go?” We recorded the first, second, third, fourth, and fifth options reported for each queston. Each multiplier was calculated as the reciprocal of the proportion of survey participants who responded that they would attend a particular healthcare facility as their first or second choice healthcare provider .
Population Denominators
Population totals of health facility catchment areas were obtained from the most recent national census or most relevant demographic surveillance period. Population denominators were stratified into age <15 years and age ≥15 years to calculate age-group specific incidence.
Statistical Analysis
Incidence was estimated by age group, age <15 years, ≥ 15 years, and overall, and by site with the use of the multipliers described above to account for leptospirosis cases that were potentially missed in the stages of reporting (Figure 1).
Specifically, the incidence rate per person year, , was calculated using the formula:
where was the number of confirmed acute leptospirosis cases and Y was the number of person-years. The other terms correspond to the multipliers.
This simplifies to:
where and . Thus, can be viewed as the product of three estimates: (1) the proportion positive for leptospirosis among those tested; (2) the incidence of fever cases presenting at a health facility; and (3) the inverse of the proportion of those with fever who seek care. We calculated a 95% confidence interval for by incorporating uncertainty from each of these three estimates via the delta method (Supplementary Appendix 3) [23].
We conducted two sensitivity analyses. In the first we accounted for the possible surveillance artifact associated with COVID-19 lockdowns and other disruptions from 2020, by restricting to the pre-2020 period. In the second, we adjusted for the sensitivity of 93.8% and specificity of 97.3% of Leptospira MAT serology by replacing in the simplified equation with an adjusted value, , based on the Rogen-Gladen correction [24]:
where and denote the sensitivity and specificity estimates.
Sample Size
The sample size for this analysis was driven by that of the parent FIEBRE study and is described in detail elsewhere [9].
Research Ethics
Ethics approval was obtained from the National Ethics Committee for Health Research Committee and the Oxford Tropical Research Ethics Committee for the Laos; the University of Malawi College of Medicine Research and Ethics Committee and the Liverpool School of Tropical Medicine Research Ethics Committee for Malawi; Comité Institucional de Medical Research Bioética para a Saúde do Centro de Investigação em Saúde de Manhiça, and the Comité Nacional de Bioética em Saúde de Moçambique for Mozambique; and the Medical Research Council of Zimbabwe for Zimbabawe. The study was also approved by the research and ethics committee of the London School of Hygiene and Tropical Medicine. Written informed consent is obtained from all participants or their parents or guardians.
RESULTS
Leptospirosis Cases
A total of 7851 patients with fever were enrolled in the FIEBRE study, including 1972 (25.1%) in Lao PDR, 1773 (22.6%) in Malawi, 2182 (27.8%) in Mozambique and 1924 (24.5%) in Zimbabwe. The characteristics of the overall FIEBRE cohort and the participants with leptospirosis have been described in detail elsewhere [10]. Of those enrolled, 4503 had paired sera tested by Leptospira MAT and acute plasma by Leptospira lfb1 PCR, including 966 (49.0%) in Lao PDR, 1269 (71.6%) in Malawi, 1191 (54.6%) in Mozambique and 1077 (56.0%) in Zimbabwe. Of those tested, 38 (0.8%) had confirmed leptospirosis based on a positive Leptospira lfb1 PCR, 96 (2.1%) had confirmed leptospirosis based on paired Leptospira MAT serology, and 128 (2.8%) met the confirmed leptospirosis case definition based on either MAT or PCR, including 78 (8.1%) in Lao PDR, 21 (1.7%) in Malawi, 7 (0.6%) in Mozambique, and 22 (2.0%) in Zimbabwe.
Healthcare Utilization
In the health care utilization survey, 2401 matched control participant households were enrolled, including 485 (20.2%) in Laos, 908 (37.8%) in Malawi, 572 (23.8%) in Mozambique, and 436 (18.2%) in Zimbabwe. Four controls with missing age in Mozambique were excluded from the current analysis. Table 1 show the demographic and co-infection status of FIEBRE controls by site.
Multiplier Derivation
Enrollment Multiplier
The number of participants enrolled by site and the number of febrile participants presenting by site was 1972 and 16 967 in Laos, 1773 and 77 634 in Malawi, and 2182 and 14 604 in Mozambique, yielding enrollment multipliers of 8.6, 43.8, and 6.7, respectively. Accurate counts of the number of patients presenting with fever to Zimbabwe FIEBRE study healthcare facilities were not available due to COVID-19 disruptions and healthcare worker strikes.
Paired Sera Multiplier
The number of participants with paired sera was 966 in Laos, 1269 in Malawi, and 1191 in Mozambique, yielding paired sera multipliers of 2.0, 1.4, 1.8, respectively.
Diagnostic Test Accuracy Multiplier
While the primary analysis assumed 100% sensitivity and specificity of Leptospira MAT on paired sera, in a sensitivity analysis we assumed a sensitivity of 93.8% and specificity of 97.3% [22].
Health Facility Multiplier
The proportion of control participants identifying a FIEBRE study healthcare facility as the first or second choice location that they would seek healthcare in the event of a fever for ≥3 days was 147 (30%) of 485 in Laos, 846 (93%) of 908 in Malawi, and 53 (9%) of 568 in Mozambique, yielding health facility multipliers of 3.3, 1.1, and 10.7, respectively.
Incidence Calculations
Leptospirosis incidence (95%CI) per 100 000 population per year was 1302 (1,011, 1677) in Laos, 1337 (874, 2044) in Malawi and 187 (85, 409) in Mozambique. We did not calculate incidence for Zimbabwe as accurate counts of the number of patients presenting with fever to Zimbabwe FIEBRE study healthcare facilities were not available. Incidence estimates by age group <15 years, ≥ 15 years and site are shown in Table 2. A sensitivity analysis restricted to pre-COVID years of 2018 and 2019 produced similar estimates of incidence to that of the whole study period (Table 3). A sensitivity analysis adjusted for diagnostic sensitivity and specificity yielded similar estimates in Laos but suggested that apparent incidence in Malawi and Mozambique could be largely attributable to false positives (Table 4).
DISCUSSION
We provide, to the best of our knowledge, the first estimates of leptospirosis incidence from sites in Lao PDR, Malawi, and Mozambique, adding considerably to the limited number of available estimates of leptospirosis incidence from low-resource settings. We show that leptospirosis incidence exceeded 100 per 100 000 population per year at sites in three countries, highlighting considerable illness in these previously unstudied locations.
We estimated that incidence of leptospirosis was significantly higher in the Lao PDR and Malawi sites than the Mozambique site during the study period. While leptospirosis incidence in Laos and Malawi may be stably higher than in Mozambique, it is also possible that differences represent fluctuations in incidence over time, as has been observed elsewhere [19]. We have shown that work in rice fields was substantially more common at the Lao PDR site than in the African sites [10]. Additionally, the Malawi study site of Chikwawa is located in a rural, low-lying area adjacent to and including the flood plain of the Shire River, a major tributary to the Zambezi River. It could therefore be speculated that both the Laos and Malawi study catchment areas provide substantial risk for exposure to moist soil potentially contaminated with Leptospira [10]. Notably, the FIEBRE leptospirosis incidence estimates were at the high end of the range of those identified by a systematic review of the World Health Organization Leptospirosis Burden Epidemiology Reference Group (LERG) [1]. Among studies identified in the LERG review from Africa incidence per 100 000 per year was 69 in Cameroon 1975–1976 [25], 101 in the Seychelles in 1995–1996 [26], and 160 in Wonji, Ethiopia 2003 [27]. Among studies from countries neighboring Lao PDR, incidence per 100 000 per year was 5 from a study from Takeo Province, Cambodia 2003 [28], 15 from Mahasarakam Province, Thailand 1996 [29], 7 from Nakornratchasrima, Thailand 1998 [30], 2 from Kamphaeng Phet, Thailand 1998–2003 [31], and 10 from Thailand national data 1994–2003 [32]. However, the LERG review included studies that measured crude incidence, often from passive surveillance, and as such likely represent underestimates of actual leptospirosis incidence [7, 8]. More data from active population-based or hybrid surveillance studies would be useful to understand the true incidence of leptospirosis.
We did not observe significant differences in leptospirosis incidence among those aged ≥15 years compared with those aged <15 years at any study site. There were statistically non-significant trends toward higher incidence in the older age groups in Laos and Malawi, and younger age groups in Mozambique. Review of global leptospirosis data indicates that risk for disease tends to be higher in adults than in children [1], likely associated with occupational exposures involving direct contact with infected animals and indirect contract with contaminated environments [6].
Our study had a number of limitations. While hybrid surveillance is a widely accepted and used method for estimating the incidence of acute infectious diseases [7, 8], factors such as differential healthcare seeking among risk groups mean that it is unlikely to yield incidence estimates that are as accurate as active, population-based surveillance. The FIEBRE study took place during the COVID-19 pandemic, resulting in disruptions to health systems that may have influenced our sentinel surveillance for leptospirosis and the healthcare utilization survey among controls. Indeed, in Zimbabwe the COVID-19 disruptions and healthcare worker strikes meant that it was not possible to estimate leptospirosis incidence there. However, for the remaining sites we explored the impact of the COVID-19 pandemic through a sensitivity analysis comparing incidence estimates from the pre-pandemic with those of the post-pandemic period and found no significant differences. Our diagnostic strategy was also a source of limitations. If the L. fainei serovar Hurstbridge IgM ELISA screening test used prior to Leptospira MAT had sensitivity <100%, we may have failed to detect some participants with leptospirosis resulting in under-estimation of disease incidence. Furthermore, incidence estimates are also sensitive to assumptions about the diagnostic accuracy of MAT, particularly its specificity. Because the prevalence of true cases is low, even a small number of false positives can substantially influence the estimates. Leptospirosis is a zoonosis with a complex ecology and incidence varies in both time and place. Therefore, our incidence estimates may not be generalizable to other locations in Asia or Africa, nor even to the same locations in different time periods.
We show that leptospirosis incidence was high in Lao PDR, Malawi, and Mozambique, countries that hitherto lack leptospirosis incidence estimates. The very high incidence observed in Laos and Malawi may relate to rice field exposure and exposure to moist flood plain environments, respectively. Our incidence estimates are at the high end of reported data and exceed those identified by the LERG systematic review of incidence studies, perhaps in part due to our use of the hybrid surveillance design to approximate incidence observed in active, population-based incidence studies. We recommend that leptospirosis be included and regularly updated in global burden of disease estimates to draw the attention of policy makers and those willing to invest in its diagnosis, management, and control.
Supplementary Material
ofag021_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Costa F, Hagan JE, Calcagno J, et al Global morbidity and mortality of leptospirosis: a systematic review. P Lo S Negl Trop Dis 2015; 9:e 0003898.26379143 10.1371/journal.pntd.0003898 PMC 4574773 · doi ↗ · pubmed ↗
- 2Torgerson PR, Hagan JE, Costa F, et al Global burden of leptospirosis: estimated in terms of disability adjusted life years. P Lo S Negl Trop Dis 2015; 9:e 0004122.26431366 10.1371/journal.pntd.0004122 PMC 4591975 · doi ↗ · pubmed ↗
- 3Allan KJ, Biggs HM, Halliday JE, et al Epidemiology of leptospirosis in Africa: a systematic review of a neglected zoonosis and a paradigm for ‘one health’ in Africa. P Lo S Negl Trop Dis 2015; 9:e 0003899.26368568 10.1371/journal.pntd.0003899 PMC 4569256 · doi ↗ · pubmed ↗
- 4de Vries SG, Visser BJ, Nagel IM, Goris MG, Hartskeerl RA, Grobusch MP. Leptospirosis in sub-saharan Africa: a systematic review. Int J Infect Dis 2014; 28:47–64.25197035 10.1016/j.ijid.2014.06.013 · doi ↗ · pubmed ↗
- 5Biggs HM, Bui DM, Galloway RL, et al Leptospirosis among hospitalized febrile patients in northern Tanzania. Am J Trop Med Hyg 2011; 85:275–81.21813847 10.4269/ajtmh.2011.11-0176 PMC 3144825 · doi ↗ · pubmed ↗
- 6Levett PN . Leptospirosis. Clin Microbiol Rev 2001; 14:296–326.11292640 10.1128/CMR.14.2.296-326.2001 PMC 88975 · doi ↗ · pubmed ↗
- 7Crump JA, Youssef FG, Luby SP, et al Estimating the incidence of typhoid fever and other febrile illnesses in developing countries. Emerg Infect Dis 2003; 9:539–44.12737736 10.3201/eid 0905.020428 PMC 2972755 · doi ↗ · pubmed ↗
- 8Andrews JR, Barkume C, Yu AT, et al Integrating facility-based surveillance with healthcare utilization surveys to estimate enteric fever incidence: methods and challenges. J Infect Dis 2018; 218:S 268–76.30184162 10.1093/infdis/jiy 494PMC 6226762 · doi ↗ · pubmed ↗