Myelodysplastic Syndrome (MDS) With KMT2A::CBL Rapidly Progressed to Acute Myeloid Leukaemia (AML)
Ke Xu, Temenuzhka Boneva, Elisabeth Nacheva

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
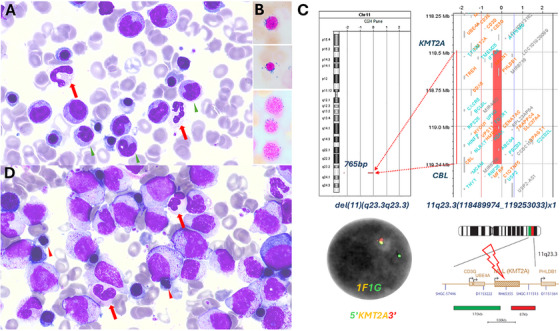 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Blood disorders and treatments · Myeloproliferative Neoplasms: Diagnosis and Treatment
1
A 73‐year‐old female presented with progressive isolated normocytic anaemia. The blood work showed haemoglobin 95 g/L, white blood cells 4.7 × 10^9^/L (neutrophil 2.6 × 10^9^/L, monocytes 0.4 × 10^9^/L) and platelets 172 × 10^9^/L. The bone marrow aspirate showed dysplastic neutrophils (> 10%) and erythroblasts (> 10%), 22% monocytes and 2% of blasts (Figure 1A). Flow cytometry showed 0.1% blasts and 57% CD14+CD56+ monocytes. Iron stain showed 15% ring sideroblasts (Figure 1A). Targeted fluorescence in situ hybridisation (FISH) analysis (Cytocell) and chromosomal microarray analysis (CMA) using 8 × 60 K oligonucleotide arrays (Agilent) showed loss of the 7q22.1 region (housing CUX1 gene among others) and a 765 bp deletion within 11q23.3, suggestive of KMT2A::CBL fusion gene formation (Figure 1B). RNA sequencing (Archer Fusion Plex Pan‐Heme panel) showed KMT2A::CBL fusion transcript. Pan‐Heme VariantPlex NGS (157 gene panel) showed TET2 p.Leu500Ile (VAF 81%), DIS3 p.Tyr867Ter (VAF 51%) and SRSF2 p.Pro95Arg (VAF 47%) variants. The patient was diagnosed with MDS, multiple lineage dysplasia, IPSS‐R intermediate risk and IPSS‐M moderate high risk. MDS with ring sideroblast usually has a better outcome, but the presence of KMT2A::CBL puts this patient at high risk of progression to AML. She was monitored closely. Two and a half months later, she developed worsening anaemia, mild neutropenia and monocytosis. Hb 80 g/L, WBC 4.1 × 10^9^/L (neutrophils 1.3 × 10^9^/L, monocytes 1.5 × 10^9^/L) and platelets 157 × 10^9^/L. The repeat bone marrow aspirate showed 50% monocytoid blasts on the background of MDS (Figure 1C). By flow cytometry, the blasts were positive for CD33, HLADR, CD15, CD56, CD11b, cMPO and negative for CD34, CD117, CD19, CD22, cCD79a and cCD3. Myeloid NGS showed SRSF2 p.Pro95Arg (VAF 48%), TET2 p.Leu500IlefsTer4 (VAF 83%) and TET2 p.Gly1815GlufsTer7 (VAF 4%) variants. Targeted FISH and CMA again showed loss of the CUX1 gene, 12q24 loss and a cryptic deletion within 11q23.3. RNAseq showed persistence of KMT2A::CBL fusion. She was diagnosed with AML with KMT2A rearrangement (KMT2Ar).
(A) Bone marrow aspirate (May‐Grünwald–Giemsa stain, ×100 objective) at diagnosis showed > 10% dysplastic hypogranulated neutrophils (red arrow), monocytosis (green arrow head) and no excess of blasts; (B) Iron stain (×100 objective) showed ring sideroblasts. (C) At diagnosis, FISH (DAPI staining, ×100 objective) using KMT2A break‐apart probe showed 1F1G signal, suggestive of del(11). CMA showed a cryptic deletion within 11q23.3, suggestive of KMT2A::CBL fusion. (D) Bone marrow aspirate (May‐Grünwald–Giemsa stain, ×100 objective) at disease progression showed large monocytoid blasts with open chromatin, prominent nucleoli, no auer rods and dysplastic erythroblasts (red arrow head showing irregular nuclear contour) and dysplastic neutrophils (red arrows showing Pseudo‐Pelger–Huët forms).
Here, we report a rare case of MDS with KMT2A::CBL and low blast count that rapidly progressed to KMT2Ar AML. KMT2A rearrangement is considered to be AML‐defining by WHO5 [1] and ICC classification [2]. WHO5 requires an excess of myeloblasts in the bone marrow (≥ 5%) or peripheral blood. ICC requires myeloblast *≥ *10%. KMT2A rearrangement is rare in MDS. Arber DA et al. reported 31 KMT2Ar MDS/chronic myelomonocytic leukaemia (CMML) cases with similar median overall survival compared to the 100 cases of KMT2Ar AML (12 months vs. 14.4 months, *p *= 0.62), raising the hypothesis that KMT2Ar MDS/CMML and AML likely represent the same biologic entity [3]. Given the grey zone for MDS with KMT2A rearrangement without blast excess, a multidisciplinary team approach is recommended for optimal management on a case‐by‐case basis.
Author Contributions
K.X. wrote up the manuscript. K.X., T.B. and E.N. critically revised the final version of the manuscript.
Funding
The authors have nothing to report.
Ethics Statement
The authors have nothing to report.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO , “Haematolymphoid Tumours Part A,” in WHO Classification of Tumours, 5th ed. (IARC Press, 2024).
- 2D. A. Arber , A. Orazi , R. P. Hasserjian , et al., “International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: Integrating Morphologic, Clinical, and Genomic Data,” Blood 140, no. 11 (2022): 1200–1228, 10.1182/blood.2022015850.35767897 PMC 9479031 · doi ↗ · pubmed ↗
- 3M. Siddiqui , S. Konoplev , G. Issa , et al., “Biologic Features and Clinical Outcomes in Newly Diagnosed Myelodysplastic Syndrome With KMT 2A Rearrangements,” American Journal of Hematology 98 (2023): E 91–E 94, 10.1002/ajh.26858.36661399 · doi ↗ · pubmed ↗