Transfemoral Transcatheter Aortic Valve Implantation for Severe Aortic Stenosis in a Patient With Prior Tendyne Transcatheter Mitral Valve Replacement: Expanding the Boundaries of Transcatheter Valve Therapy
Rajan Rehan, Ben McDonough, Bernard Prendergast, Simon Redwood

TL;DR
This paper shows that aortic valve implantation can be safely done in patients who previously had a Tendyne mitral valve replacement.
Contribution
It introduces a safe approach for transcatheter aortic valve implantation after prior Tendyne mitral valve replacement.
Findings
Transfemoral transcatheter aortic valve implantation is feasible in patients with prior Tendyne mitral valve replacement.
Preprocedural CT planning helps assess risks of left ventricular outflow tract obstruction and device interaction.
Self-expanding aortic valves may reduce device interaction risks in complex anatomical cases.
Abstract
•Transfemoral transcatheter aortic valve implantation can be safely performed in patients with prior Tendyne transcatheter mitral valve replacement.•Careful preprocedural computed tomography planning allows assessment of left ventricular outflow tract obstruction risk and spatial interaction between the Tendyne frame and the aortic annulus.•Use of a self-expanding transcatheter aortic valve may minimize the risk of device interaction in this complex anatomical setting. Transfemoral transcatheter aortic valve implantation can be safely performed in patients with prior Tendyne transcatheter mitral valve replacement. Careful preprocedural computed tomography planning allows assessment of left ventricular outflow tract obstruction risk and spatial interaction between the Tendyne frame and the aortic annulus. Use of a self-expanding transcatheter aortic valve may minimize the risk of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
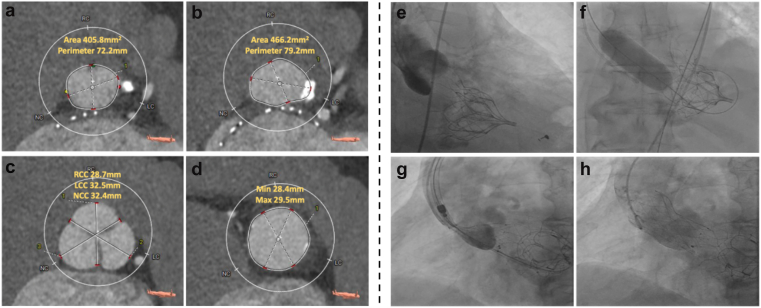 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Aortic Disease and Treatment Approaches · Diagnosis and Treatment of Venous Diseases
With the growing adoption of transcatheter mitral valve replacement (TMVR), the Tendyne system (Abbott, Santa Clara, CA) represents the largest cohort of patients, supported by the longest available follow-up data.1 The Tendyne bioprosthesis incorporates a self-expanding D-shaped nitinol frame designed to conform to the native mitral annulus. This design may alter the left ventricular geometry and narrow the left ventricular outflow tract (LVOT), making subsequent transcatheter procedures, particularly transcatheter aortic valve implantation (TAVI), anatomically and technically challenging.
We report the case of a 78-year-old man with a prior TMVR using a Tendyne bioprosthesis 3 years earlier for degenerative mitral regurgitation, who presented with progressive congestive cardiac failure (New York Heart Association class III–IV). Transthoracic echocardiography (TTE) demonstrated a dilated left ventricle with severe systolic dysfunction (biplane ejection fraction 27%) and a heavily calcified tricuspid aortic valve with severe low-flow, low-gradient aortic stenosis (aortic valve area 0.8 cm2; mean gradient 21 mmHg). The Tendyne prosthesis was well seated with a mean transmitral gradient of 3 mmHg and trace regurgitation. Multidetector computed tomography demonstrated an aortic annular area of 406 mm^2^, perimeter 72.2 mm, with left and right coronary heights of 13.8 and 15.3 mm, respectively. LVOT obstruction risk was assessed by qualitative evaluation of the aortomitral curtain through multiplanar computed tomography reconstructions, confirming preserved spatial clearance between the anterior Tendyne frame and aortic annulus suggesting a low risk. The iliofemoral vessels were of adequate caliber, without significant tortuosity or calcification, confirming suitability for transfemoral TAVI.
Under general anesthesia, balloon aortic valvuloplasty was performed using a 22 mm True balloon (Video 1). Subsequently, a 27-mm Navitor (Abbott, London, UK) TAVI was advanced via the transfemoral approach and deployed under rapid ventricular pacing (120/min) (Video 2). A self-expanding Navitor platform was selected to allow controlled, gradual deployment and minimize the risk of interaction between a balloon-expandable system and the adjacent Tendyne frame. The valve expanded symmetrically with optimal positioning and satisfactory hemodynamic performance, with a postimplant mean transvalvular gradient of 6 mmHg and mild anterior paravalvular regurgitation on TTE. The Tendyne mitral prosthesis remained well seated with stable transmitral gradients and no evidence of LVOT obstruction. The patient had an excellent recovery and was discharged 24 hours postprocedure. At 30 days, the patient remained clinically well, with stable valve hemodynamics, preserved Tendyne function, and no LVOT obstruction on TTE.
To our knowledge, this represents the first reported case of TAVI for native aortic stenosis in a patient with a pre-existing TMVR (Figure 1). Previous publications have described the reverse sequence (TAVI followed by TMVR),2 as well as valve-in-Tendyne procedures3; however, the TAVI performed after prior Tendyne implantation has not been previously reported. This case highlights the importance of preprocedural planning to define the spatial relationship between the Tendyne frame and aortic annulus ensuring safe device interaction with an altered left ventricular geometry. The procedure demonstrates the technical feasibility and favorable hemodynamic performance of TAVI following prior Tendyne TMVR, thereby extending the therapeutic possibilities for high-risk patients with complex multivalvular disease.Figure 1Preprocedural CT assessment and procedural fluoroscopy during TAVI. (a–d) Preprocedural multidetector computed tomography (CT) analysis: (a) aortic annulus measurements (area = 405.8 mm^2^; perimeter = 72.2 mm); (b) left ventricular outflow tract (LVOT) measurements (area = 466.2 mm^2^; perimeter = 79.2 mm); (c) sinus of Valsalva dimensions (right coronary cusp [RCC] = 28.7 mm, left coronary cusp [LCC] = 32.5 mm, noncoronary cusp [NCC] = 32.4 mm); and (d) sinotubular junction measurements (minimum diameter = 28.4 mm, maximum diameter = 29.5 mm). Multiplanar reconstructions were additionally reviewed to demonstrate preserved clearance between the Tendyne frame and aortic annulus, supporting a low risk of LVOT obstruction. (e–h) Fluoroscopic images during transcatheter aortic valve replacement (TAVR): (e) baseline aortogram; (f) balloon aortic valvuloplasty with a 22 mm True balloon; (g) partial deployment of a 27 mm Navitor valve; and (h) final fully deployed Navitor 27 mm valve in optimal position.Abbreviation: TAVI, transcatheter aortic valve implantation.
Consent Statement
Written informed consent was obtained from the patient. All reasonable efforts were made to ensure anonymity and that no identifying information would be disclosed.
Funding
This work was supported by the British Heart Foundation [grant number FS/CRTF/25/24841]
Disclosure Statement
Rajan Rehan is supported by an RACP Research Establishment Fellowship.
The other authors had no conflicts to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Duncan A.Sorajja P.Dahle G.3-Year outcome of tendyne transcatheter mitral valve replacement to treat severe symptomatic mitral valve regurgitation JACC Cardiovasc Interv 1720241625162710.1016/j.jcin.2024.05.02038986665 · doi ↗ · pubmed ↗
- 2Shah M.A.Almahrous N.Alreshidan M.Alshehri H.Z.Transcatheter mitral valve implantation using the Tendyne valve in a patient with prior transcatheter aortic valve implantation: a case report Eur Heart J Case Rep 72023 ytad 47610.1093/ehjcr/ytad 476PMC 1058353937860683 · doi ↗ · pubmed ↗
- 3Duncan A.Quarto C.Denti P.Smith R.Heng E.L.Structural degeneration of a 9-Year-Old tendyne: treatment by transfemoral transseptal SAPIEN in tendyne JACC Case Rep 29202410244710.1016/j.jaccas.2024.102447 PMC 1132874739157557 · doi ↗ · pubmed ↗