An Unexpected Cause of Diabetic Foot Ulcer Infection: Pasteurella multocida
Jesse H Wu, Paul M Shaniuk

TL;DR
A rare case of diabetic foot ulcer infection caused by Pasteurella multocida is reported, highlighting the importance of considering atypical pathogens and exposure history.
Contribution
This paper presents a rare clinical case of Pasteurella multocida osteomyelitis in a diabetic patient, emphasizing its potential severity and diagnostic implications.
Findings
Pasteurella multocida can cause severe osteomyelitis in diabetic foot ulcers.
The infection likely originated from indirect exposure to a household dog.
Culture-guided therapy and amputation were necessary for effective treatment.
Abstract
Diabetic foot infection (DFI) is a common complication of diabetes mellitus and a major cause of preventable morbidity and mortality in individuals with diabetes. Superficial DFI can lead to contiguous spread to soft tissue and bone as well as hematogenous spread and sepsis. It frequently involves typical pathogens such as Staphylococcus aureus and Pseudomonas aeruginosa, or it may be polymicrobial, involving Gram-negative bacilli and anaerobes. Atypical organisms can also be responsible, especially when environmental exposures are present. We report a rare case of Pasteurella multocida osteomyelitis in a 75-year-old man with diabetes with a chronic foot ulcer. The infection likely developed from indirect exposure to his household dog after a piece of dog food became trapped in his shoe, which went undetected due to peripheral neuropathy. After failing outpatient management, he…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2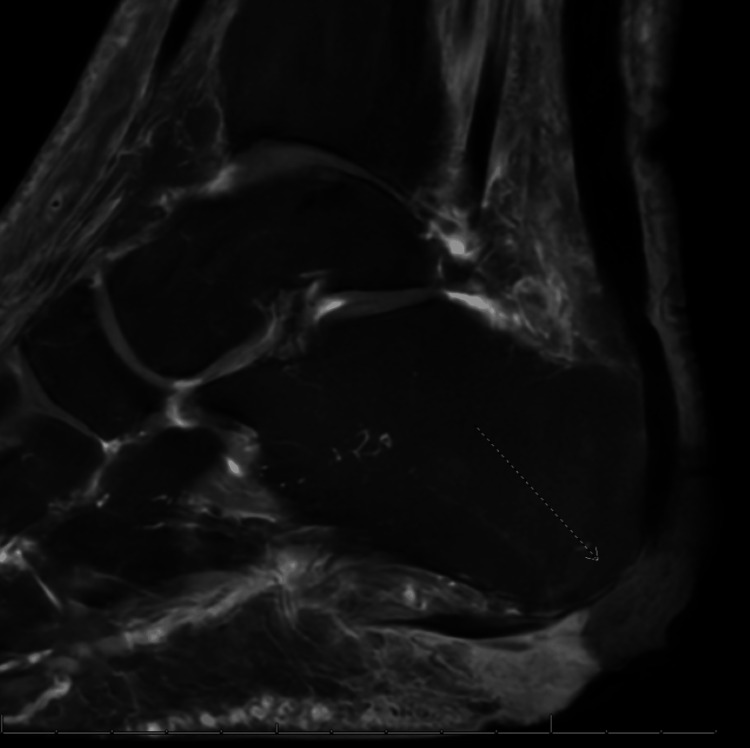 Figure 3
Figure 3| Lab study | Parameter | Patient’s value | Reference range |
| CBC | WBC | 11.5 k/cm2 | 4.5 - 11 k/cm2 |
| Hgb | 13.2 g/dL | 13.2 - 16.6 g/dL | |
| Hct | 39.8% | 38.3% - 48.6% | |
| Plt | 323 k/cm2 | 150 - 400 k/cm2 | |
| Automated differential | Neutrophils | 75.4% | 40 - 60% |
| Lymphocytes | 12.9% | 20 - 40% | |
| Monocytes | 8.1% | 4 - 8% | |
| Eosinophils | 2.5% | 1 - 3% | |
| Procalcitonin | Procalcitonin | 0.05 ng/mL | <0.1ng/mL |
| Serum chemistry | Na | 140 mmol/L | 135 - 145 mmol/L |
| K | 4.1 mmol/L | 3.5 - 5 mmol/L | |
| Cl | 106 mmol/L | 96 - 106 mmol/L | |
| CO2 | 23 mmol/L | 22 - 26 mmol/L | |
| BUN | 12 mg/dL | 7 - 20 mg/dL | |
| Cr | 0.8 mg/dL | 0.6 - 1.3mg/dL | |
| Glucose | 130 mg/dL | 70 - 100 mg/dL | |
| Albumin | 3.8 g/dL | 3.5 - 5.0 g/dL | |
| Total Protein | 8.0 g/dL | 6.0 - 8.3 g/dL | |
| ESR | ESR | 65 mm/hr | <20 mm/hr |
| CRP | CRP | 7.36 mg/dL | <1.0mg/dL |
| Wound culture | N/A |
| N/A |
| Antibiotic susceptibility testing | N/A | Does not produce beta-lactamase | N/A |
| Blood cultures | N/A | No growth after 5 days | N/A |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRabies epidemiology and control · Reconstructive Surgery and Microvascular Techniques · Nonmelanoma Skin Cancer Studies
Introduction
Diabetic foot infection (DFI) is a serious complication of diabetes mellitus, often leading to significant morbidity and, in severe cases, lower extremity amputation. Around 19% to 24% of people worldwide with diabetes will develop a diabetic foot ulcer in their lifetime [1]. These infections typically arise due to a combination of peripheral neuropathy, peripheral arterial disease, and impaired immune response, which predisposes patients to ulcers that become secondarily infected. Osteomyelitis occurs in 15% of DFIs, of which 15% require amputation [2]. In the largest and longest evaluation of the risk of death among those with diabetes and lower extremity amputation, individuals with diabetes who have had lower extremity amputation were three times more likely to die than those who did not receive lower extremity amputation [3]. In addition, in any given year, >5% of those with diabetes and lower extremity amputation will die [3]. The most common pathogens involved include aerobic Gram-positive cocci (Staphylococcus aureus, Streptococcus pyogenes, and coagulase-negative staphylococci) and Pseudomonas aeruginosa [4]. Deep infections are more likely to be polymicrobial, involving Gram-negative bacilli and anaerobes. There is less information about the management of this common condition when the causative organism is atypical. We describe an uncommon pathogen as the cause of osteomyelitis in a diabetic foot ulcer.
Case presentation
A 75-year-old male presented with a worsening left foot ulcer with redness, warmth, and swelling extending up the left calf. Past medical history was significant for type 2 diabetes mellitus (complicated by neuropathy), hypertension, benign prostatic hyperplasia, and dyslipidemia.
One week prior to admission, he presented to the podiatry outpatient clinic for a new left lateral heel wound along with a chronic plantar heel wound that was concerning for infection. He was started on amoxicillin-clavulanate. He reported using povidone-iodine-soaked dressings every day, which had resulted in soaking through to the bedsheets. One day prior to admission, he wrapped a plastic bag around his povidone-iodine-soaked dressing overnight, which caused the foot to become moist. He reported finding a flap of whitened, dead skin off the lateral heel in the morning, along with moist, swollen tissue on the foot. He trimmed the skin flap off and discarded it before going to his podiatry appointment on the day of admission.
He reported his wound started about six months ago when a piece of dog food got stuck in his shoe, and he could not feel it due to his neuropathy. It started as a blister and had worsened over time to approximately 1.5 cm x 3 cm, and he had been seeing a podiatrist for it. He had been adherent to amoxicillin-clavulanate for the week prior to admission, but he reported increasing fatigue. He reported left lower extremity redness and swelling, as well as loss of sensation in the bilateral feet and intermittent shock-like sensations running up his left leg. He denied fever, chills, weakness, or pain elsewhere. He was started on intravenous vancomycin and piperacillin-tazobactam in the emergency department and admitted to the hospital. A1C measured at the beginning of admission was 6.7%. Considering the lack of response to initial antibiotics and the history of a moist wound, empiric antibiotics aimed to target Gram-positive organisms, including methicillin-resistant S. aureus, as well as P. aeruginosa and anaerobes.
Vital signs at admission were 100.8°F, a heart rate of 90 beats per minute, a respiratory rate of 18 breaths per minute, and 98% oxygen saturation on room air. A skin exam demonstrated a 1.5 cm x 3 cm tense black necrotic ulcer on the lateral aspect of the left heel and a 2 cm x 2 cm ulcer on the plantar aspect of the left heel (Figure 1). A neurologic exam revealed loss of proprioception in the left hallux, with proprioception maintained in the right. There was a loss of crude touch near the toes bilaterally on the plantar surface. There was a palpable 2+ posterior tibial pulse on the right, but no palpable posterior tibial pulse on the left. There was a markedly dependent rubor in the left calf with warmth and pitting edema. A biphasic Doppler signal was found on the right, but it was not found on the left.
Necrotic plantar heel wound.
Labs demonstrated leukocytosis with neutrophilic predominance, elevated erythrocyte sedimentation rate (ESR), and elevated C-reactive protein (CRP), likely reflecting active infection. The remaining studies were otherwise unremarkable, including a blood culture that showed no growth after five days (Table 1).
An X-ray of the foot demonstrated sclerotic changes to the plantar calcaneus without signs of osteomyelitis (Figure 2). Pulse volume recordings were obtained and were normal. MRI demonstrated osteomyelitis of the calcaneus (Figure 3).
Plain film radiograph of the foot.This patient's X-ray image demonstrated sclerotic changes to the plantar calcaneus without signs of osteomyelitis.
MRI of the calcaneus.This patient's MRI demonstrated osteomyelitis of the calcaneus (represented by the dotted arrow).
His fatigue improved throughout the first day of admission on intravenous vancomycin and piperacillin-tazobactam. On the second day of admission, his wound was debrided by the Inpatient Podiatry service, yielding purulent fluid that was cultured. The bone probe at this time was positive, and the foot was deemed unsalvageable.
Wound cultures grew Pasteurella multocida and diphtheroids. Antibiotic susceptibility testing revealed that the P. multocida did not produce beta-lactamase. The history of the dog sniffing the wound and the dog food particle in his shoe was confirmed at this time, although he denied any history of the dog licking him or any other direct contact with the wound. His antibiotics were switched to intravenous ampicillin-sulbactam, as P. multocida grown was susceptible to beta-lactams, and the beta-lactamase inhibitor was added to cover the potential pathogenic role of the diphtheroids. Labs and clinical status remained stable throughout the hospital stay, and he received a below-the-knee amputation. He was transitioned to oral amoxicillin-clavulanate the day of amputation to complete a course of five days post-operation.
Discussion
Foot infections are the most common cause of hospitalization in patients with diabetes, and they are a major cause of lower extremity amputations in the United States [5]. Risk factors for foot infection include sustaining a foot wound, recurrent or prolonged wounds (greater than 30 days), and peripheral artery disease [5]. Acute hematogenous osteomyelitis may be treated with antibiotics alone, but chronic osteomyelitis usually requires surgical management [6].
First discovered in 1878 by Edoardo Perroncito and isolated by Louis Pasteur in 1881 as the cause of fowl cholera, Pasteurella multocida is a Gram-negative coccobacillus that causes a variety of clinical syndromes. Multocida means “many killing,” referring to the fact that this bacterium is pathogenic for many species of animals [7]. It is a commensal bacterium in the oropharynx and upper respiratory tract of mammals and fowl [8]. Transmission to humans usually comes from cats and dogs, with reported carrier rates of 70% to 90% and 20% to 50%, respectively [9]. Based on our review of the literature, only a few cases exist in the past 15 years of Pasteurella multocida being a cause of diabetic skin and soft tissue infection or osteomyelitis of the foot [10-13].
Although Pasteurella multocida infection is most commonly associated with an exposure history, cases without an exposure history were more associated with bacteremia and increased hospital admissions. Exposure to household pets has been implicated in disease. However, infections not associated with an animal bite were also associated with increased severity of illness, with higher intensive care utilization and increased mortality [9]. The absence of bite or scratch in history may be associated with preexisting pulmonary disease, open wounds, or immunocompromise. Therefore, Pasteurella multocida in the absence of bite or scratch history should be considered an opportunistic infection [14].
In this patient, the foot wound began six months prior to presentation, but systemic symptoms (i.e., fatigue) were only present for the week prior to presentation. There is a possibility that this is a case of chronic calcaneal osteomyelitis, as it is impossible to truly know when the infection spread to the bone, but the time course is more consistent with acute osteomyelitis. Treatment failure with amoxicillin-clavulanate, which was started only one week prior to presentation, can likely be attributed to the onset of osteomyelitis necessitating surgical intervention prior to the start of antibiotic therapy.
Isolating a causative organism in osteomyelitis in a DFI can be challenging. Wound cultures are helpful in determining a causative organism regardless of bone involvement and are recommended by the Infectious Diseases Society of America (IDSA) guidelines on DFI [15]. The first step in the workup of suspected osteomyelitis is obtaining a plain film X-ray radiograph. Changes seen on X-ray may include periosteal reaction, regional osteopenia, cortical loss, or endosteal scalloping. Unfortunately, changes may take five to seven days in children and 10 to 14 days in adults to appear on a radiograph, making this a less sensitive test for osteomyelitis [16].
MRI is the mainstay in the diagnosis of osteomyelitis as the most sensitive and specific test [17]. Probe to bone test, which is where the provider probes the injury with a metal rod, scratching the innermost surface to feel for bone, has also shown a high diagnostic accuracy with a pooled sensitivity/specificity of 0.87 (95% confidence interval, 0.75-0.93) and 0.83 (95% CI, 0.65-0.93), respectively [18]. While the gold standard confirmatory test is the bone biopsy, this test may be a low-yield procedure, playing a minor role in diagnosis [19]. Often, results are concordant with clinical and radiologic impressions and rarely change management. A bone biopsy was not performed in this patient due to the likely low yield with an invasive procedure, considering antibiotic therapy had already been initiated a week prior to presentation. This does weaken the causative connection between P. multocida and osteomyelitis. But the pus obtained from wound debridement (which was cultured) was contiguous with the calcaneus, and along with the exposure history, a diagnosis of P. multocida osteomyelitis was made.
The pathogenic vs colonizing role of diphtheroids (i.e., non-diphtheriae Corynebacterium species, normal components of flora) is controversial, as reflected by the 2023 IDSA/International Working Group on the Diabetic Foot (IWGDF) Guidelines on the Diagnosis and Treatment of Diabetes-related Foot Infections [20]. The guidelines recommend having a careful sterile wound culture during debridement in order to avoid the growth of diphtheroids and other colonizers in the culture. In this case, the addition of a beta-lactamase inhibitor in the narrowed antibiotic regimen was to cover for the potential pathogenic role of diphtheroids in the osteomyelitis.
Prompt diagnosis of P. multocida infection or a new ulcer may improve outcomes in DFI, especially since many in this population lack sensation in the lower extremity due to neuropathy. Additional challenges in diabetes mellitus and osteomyelitis include poor wound healing and recurrence of infection. In this case, the patient could not feel the piece of dog food that was stuck in his shoe and only visually noticed it several days after a new wound had developed. The patient self-managed the wound at home prior to presenting for management, and foot wound debridement with culture of the drained purulent fluid occurred after hospitalization. The antibiotics were able to be narrowed to ampicillin-sulbactam and transitioned to oral amoxicillin-clavulanate after adequate source control with amputation. Amoxicillin-clavulanate was continued for five days post-operatively, as the most recent IDSA/IWGDF guidelines recommend a two to five-day course after surgical intervention [20].
The lack of a bone biopsy confirming the presence of* Pasteurella multocida* within the calcaneus is a limitation of this case report, as it weakens our conclusion of the causative link between P. multocida and the osteomyelitis diagnosed by MRI. However, due to the low likelihood of a result changing management of this patient and the costs associated, the bone biopsy was not performed, and the amputated foot was not sent for pathology. Post-operative recovery course was not complicated by any recurrence of infection, representing a response to the treatments given.
Conclusions
Although P. multocida is an uncommon cause of osteomyelitis, it should be considered in patients at risk for opportunistic infections. Careful social history should include asking about a history of household pets or recent animal scratches or bites in a patient with a non-healing wound or deep-seated infection. Treatment depends on early clinical recognition and targeted antibiotic therapy, as well as surgical management for source control. While plain film radiography and MRI have substantial roles in diagnosis, antimicrobial therapy should also be guided by clinical impression and history. In this case, the 75-year-old male with an environmental history significant for dog food in the shoe and potential contact with dog saliva prompted clinical suspicion for P. multocida infection. Plain film radiography did not demonstrate evidence of osteomyelitis, but MRI did, demonstrating the value of MRI as a confirmatory test in cases of suspected osteomyelitis. There was a lack of specific animal bite or lick in his history, prompting a search for more disseminated infection within the bloodstream and further thought about the potential opportunistic nature of the infection. He received a below-the-knee amputation for definitive treatment and had no recurrence of infection after finishing a course of amoxicillin-clavulanate. Further research is needed to outline risk factors for localized versus disseminated infection as well as superficial versus deep tissue infection. The results of such studies may further guide the diagnosis and treatment of atypical pathogens in DFIs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diabetic foot ulcers and their recurrence N Engl J Med Armstrong DG Boulton AJ Bus SA 2367237537620172861467810.1056/NEJ Mra 1615439 · doi ↗ · pubmed ↗
- 2Incidence, outcomes, and cost of foot ulcers in patients with diabetes Diabetes Care Ramsey SD Newton K Blough D Mc Culloch DK Sandhu N Reiber GE Wagner EH 3823872219991009791410.2337/diacare.22.3.382 · doi ↗ · pubmed ↗
- 3Diabetes, lower-extremity amputation, and death Diabetes Care Hoffstad O Mitra N Walsh J Margolis DJ 185218573820152620306310.2337/dc 15-0536 · doi ↗ · pubmed ↗
- 4Diabetic foot infections Am Fam Physician Gemechu FW Seemant F Curley CA 177184882013 https://pubmed.ncbi.nlm.nih.gov/23939696/23939696 · pubmed ↗
- 5Risk factors for foot infections in individuals with diabetes Diabetes Care Lavery LA Armstrong DG Wunderlich RP Mohler MJ Wendel CS Lipsky BA 128812932920061673201010.2337/dc 05-2425 · doi ↗ · pubmed ↗
- 6Treating osteomyelitis: antibiotics and surgery Plast Reconstr Surg Rao N Ziran BH Lipsky BA 177187127 Suppl 1201110.1097/PRS.0b 013e 3182001 f 0f 21200289 · doi ↗ · pubmed ↗
- 7Species Pasteurella multocida 6 2025 2025 http://lpsn.dsmz.de/species/pasteurella-multocida
- 8Pasteurella multocida infection in humans Pathogens Piorunek M Brajer-Luftmann B Walkowiak J 12101220233788772610.3390/pathogens 12101210 PMC 10610061 · doi ↗ · pubmed ↗