Advances in the prevention and prenatal treatment of spina bifida
Zachary B. Sluzala, Katrina E. Furth

TL;DR
This review discusses recent advances in preventing and treating spina bifida, focusing on prenatal interventions and improved outcomes for patients.
Contribution
The paper highlights innovative prenatal surgical techniques and emerging therapies like stem cells and 3D printing for spina bifida.
Findings
Folic acid supplementation has significantly reduced new spina bifida cases.
In-utero surgical techniques are evolving with hybrid open and minimally invasive methods.
Emerging technologies like stem cell therapy and 3D printing are redefining treatment goals.
Abstract
Spina bifida is a neural tube defect (NTD) that arises when the neural tube fails to close properly during early development. This review focuses on myelomeningocele (MMC), the most common severe form of spina bifida, which often leads to motor and sensory impairments, including lower limb weakness or paralysis, as well as renal, urological, orthopedic, developmental, and psychosocial challenges. We explore the etiology, pathogenesis, prevention, diagnosis, and management of spina bifida, with a special emphasis on in-utero surgical repair. Over the past several decades, researchers and clinicians have made remarkable strides across all stages of care from prevention to postnatal outcomes. Widespread use of folic acid supplementation has significantly reduced the number of new cases. Advances in prenatal imaging and diagnostics now allow for earlier and more accurate detection, enabling…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
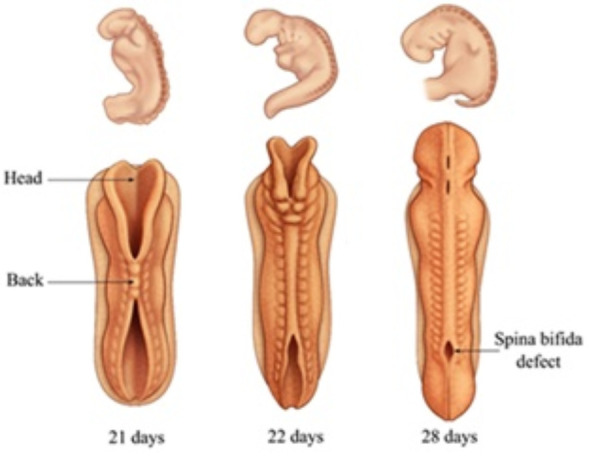 Figure 1
Figure 1| Clinical Trial | Outcomes | Year | Ref |
|---|---|---|---|
| Management of Myelomeningocele Study (MOMS) & Follow-up | Prenatal (open hysterotomy) repair is superior to postnatal repair in terms of shunt rate, reversal of hindbrain herniation, ambulation, and other metrics. | 2011-2022 |
|
| Cirurgia Endoscópica para Correção Antenatal da Meningomielocele (CECAM) | Minimally invasive fetoscopic repair is feasible, albeit with risks such as membrane rupture. | 2016 |
|
| Fetoscopic Meningomyelocele Repair Study (fMMC) & Follow-up | Hybrid laparotomy-assisted fetoscopic repair is feasible, with similar benefits to open repair and lowered risk of prematurity. | 2017-2025 |
|
| Fetoscopic NEOX Cord 1K® Spina Bifida Repair | Investigating feasibility of human umbilical cord patches for defect coverage. | Ongoing |
|
| Cellular Therapy for In Utero Repair of Myelomeningocele - The Cure Trial (CuRe) | Investigating application of stem cells to defect. Ongoing but thus far positive outcomes. | Ongoing |
|
| Approach | Key Benefits | Key Drawbacks |
|---|---|---|
| Postnatal Repair | • Non-invasive (post-birth)• Decreased risk of maternal morbidity• Decreased logistical complexity | • Worst postnatal outcomes• Little reversal of neurological defects |
| Open Hysterotomy | • Well-established• Improved postnatal outcomes | • Invasive• Necessitates c-section delivery• Risk of maternal morbidity |
| Percutaneous Fetoscopic | • Least invasive• Allows vaginal birth• Improved postnatal outcomes | • More time-consuming• Increased risk of prematurity• Limited data |
| Laparotomy-Assisted Fetoscopic | • Less invasive• Allows vaginal birth• Improved postnatal outcomes• Lowest risk of prematurity among prenatal techniques | • More time-consuming• Limited data |
| Percutaneous/Mini-Laparotomy | • Less invasive• Allows vaginal birth• Lowered risk of prematurity | • More time-consuming• Limited data |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Dysraphism and Malformations · Folate and B Vitamins Research · Fetal and Pediatric Neurological Disorders
SUMMARY
1. Introduction
2. Spina Bifida Prognosis
3. Spina Bifida Prevention: Folic Acid and NTDs
4. Spina Bifida Diagnosis
5. In-Utero Treatment for Spina Bifida
6. In-Utero Treatment for Spina Bifida: Recent Advancements of Note
7. Unresolved Challenges
8. Conclusions
1. Introduction
Spina bifida is a serious congenital condition caused by the incomplete closure of the neural tube during early embryonic development. Its prevalence varies widely across regions, with a global average ranging from 3.52 to 24.31 per 10,000 births.^1^ In the United States, spina bifida affects approximately 3.59 per 10,000 live births.^2^ Over the past three decades, early diagnosis and surgical innovation, especially prenatal intervention, have transformed the outlook for children with spina bifida. The landmark MOMS (Management of Myelomeningocele Study) trial and follow-up studies have demonstrated that fetal repair of myelomeningocele (MMC) can significantly improve motor outcomes and reduce the need for cerebrospinal fluid (CSF) shunting.^3,4^ Today, clinicians recognize the fetus as a patient in their own right, with a wide range of prenatal diagnostic tools and treatment options available. Advances in fetal medicine now allow healthcare teams not only to plan the timing, mode, and place of delivery—but in many cases, to treat the condition before birth. For families facing a spina bifida diagnosis, fetal surgery presents a hopeful alternative to termination and the potential to dramatically improve quality of life. This review synthesizes the current state of knowledge on open spina bifida, with a focus on prenatal surgery and outcome optimization.
Spina Bifida, a Neural Tube Defect
Spina bifida is a neural tube defect (NTD) that arises when the neural tube fails to close properly at the caudal (lower) end during early embryonic development.^5^ The neural plate, which formed from ectoderm around 17 days after conception,^6^ undergoes primary and secondary neurulation to form the brain and spinal cord. Primary neurulation creates a hollow tube through folding and separation from the surface around day 22, while secondary neurulation forms the lower spinal cord through the hollowing of a solid cell cord around day 26.^5,7,8^ Neural tube closure occurs in a zipper-like fashion across multiple regions, guided by signals from the notochord and surrounding tissues^9^ (see Figure 1). Neural tube defects are classified as open or closed depending on whether neural tissue is exposed to the intrauterine environment. In closed defects, neural elements are sealed off from the intrauterine environment; in open defects, neural elements, or a cyst containing neural elements, remain exposed to the amniotic fluid.^8^
In MMC, the most common severe form of spina bifida, neural elements protrude through an opening in the spine. In closed MMC, the meninges and spinal cord remain sealed off from the intrauterine environment inside a cyst. In contrast, in open MMC, the neural elements are directly exposed to amniotic fluid, which causes further injury.^8^ The commonly accepted “two-hit hypothesis” explains MMC pathogenesis: first a failure of neurulation, followed by progressive in-utero injury to exposed neural tissue.^10^ In the most severe, but rare form of spina bifida, myeloschisis (MS), the spinal cord is completely open on the back, forming a flat plate of neural tissue, or a “placode”.^11,12^ In both MMC and MS the caudal end of the spinal cord may remain fixed or tethered to the vertebral column, pulling the hindbrain into the spinal cord, known as hindbrain herniation, and blocking the flow of CSF resulting in hydrocephalus.^10^
2. Spina Bifida Prognosis
Myelomeningocele involves a wide range of motor, sensory, and developmental challenges. Children with MMC may experience lower limb weakness or paralysis, loss of sensation, and orthopedic conditions such as clubfoot, scoliosis, kyphosis (outward curvature of the spine), or hip dislocations.^11–13^ Many also face complications involving the renal and urological systems, including infections, and incontinence.^11–13^ Neurologically, MMC is often associated with hindbrain herniation, also known as Chiari II malformation, and hydrocephalus, which frequently requires cerebrospinal fluid diversion through ventriculoperitoneal shunting or endoscopic third ventriculostomy.^11–13^Some individuals may also experience seizures, along with cognitive and psychosocial difficulties.^11–13^Despite these challenges, survival rates have steadily improved, with 20-year survival ranging from 50% to 87% depending on the presence of hydrocephalus.^14^ Clinicians can now manage MMC more effectively thanks to advances in both prenatal and postnatal surgical techniques. Once viewed primarily as a life-threatening condition, MMC is now increasingly treated as a quality-of-life issue. The advent of fetal surgery has shifted treatment goals toward maximizing independence and developmental potential for affected children.^15^As medicine and technology have improved outcomes for children with spina bifida, one of the most powerful advances has been preventing the condition in the first place through folic acid supplementation.
3. Spina Bifida Prevention: Folic Acid and NTDs
Folic acid deficiency is a major contributor to the development of NTDs. Because folates cannot be synthesized from scratch, they must be obtained in the diet.^16^ Folic acid plays a critical role in synthesizing thymidylates, purines, and other components essential to the creation of DNA and RNA.^16^ In this role, folate plays a key role in cell proliferation and neurulation, processes vital for neural tube closure.^8^ This makes adequate folic acid intake especially important during early pregnancy, when the neural tube is forming. Pregnant women require five to ten times more folate than their age-matched peers.^17^
Early studies in the 1980s suggested that folic acid supplementation reduced the risk of NTDs, though initial trials were limited by small sample sizes^18^ and methodological concerns.^19^ In response, the UK Medical Research Council conducted a large, randomized controlled trial in 1991, which confirmed that a daily 4,000 μg dose of folic acid significantly reduced NTD recurrence.^20^ More recently, a large meta-analysis found that folic acid supplementation reduces the risk of NTDs by approximately two-thirds, although it did not demonstrate a clear protective effect for other congenital anomalies.^21^ Furthermore, a multicenter randomized controlled trial showed that supplementation with 4 mg of folic acid per day, compared with 0.4 mg, significantly reduced the occurrence of multiple birth defects, including NTDs.^22^ Globally, a daily intake of at least 400 μg of folic acid is recommended periconceptionally.^23^
Because neural tube closure often occurs before pregnancy is recognized (see Figure 1), relying solely on prenatal vitamin use may fail to protect many pregnancies. This recognition prompted widespread public health interventions, including mandatory folic acid fortification of cereal grain products in the United States beginning in 1998.^8^ Researchers predict that about 1300 fewer babies are given NTD diagnoses in the United States every year because of this folic acid fortification.^24^ Similar reductions in NTDs have been observed in other countries including Chile, Canada, Brazil and South Africa upon the introduction of folic acid enrichment programs.^25,26,27,28^ Currently, countries with folic acid enrichment programs have fewer cases of spina bifida (35.2 vs. 52.3 per 100,000 live births), even after accounting for stillbirth and termination of pregnancy.^1^ Despite these successes, not all countries have adopted fortification policies, leaving continued opportunities for global prevention.^1,8,29^While broader access to folic acid could prevent many cases of spina bifida worldwide, accurate and timely diagnosis remains crucial for babies who are still affected.
Folic acid makes major contributions to the development of the neural tubeNeural tube formation is often complete before a woman knows that she is pregnant because she first expects her period about 15 days after conception. Countries such as the United States started adding 140 µg of folic acid to every 100 grams of enriched grains in the 1990s, to ensure that women have enough folic acid during the critical first month of pregnancy. This reduced nationwide cases of spina bifida by up to 2/3.8 Image reproduced from reference13, with permission.
4. Spina Bifida Diagnosis
MMC is primarily diagnosed using prenatal ultrasound. Ultrasound interpretation is inherently subjective and dependent on fetal positioning; however, recent advancements have improved diagnostic accuracy. Computerized support software systems, such as those developed by Cengizler et al. allow for the algorithmic identification of the fetal spine, limiting subjectivity.^30,31^ Machine learning-based analyses have also been done to study the sonographer workflow, finding that each scan is a “non-ordered multistep process of anatomical structure acquisition” due in part to a need to take advantage of fetal position.^32^ These recent findings have helped standardize techniques while highlighting variables that can be improved upon. Ultrasound has also been shown to be a reliable diagnostic approach for MMC regardless of maternal body mass index (BMI),^33^ and cranial, spinal, ventricular, muscular, and post-surgical markers of MMC have been identified which further enhance diagnostic accuracy.^34-39^ In many cases, ultrasound is also often supplemented with molecular and biochemical testing, magnetic resonance imaging, and echocardiography ^39-47^ which help to confirm or clarify findings. Novel imaging and diagnostic techniques have also greatly advanced the capability of clinicians to identify these defects,^48^ including next-generation whole-exome sequencing technologies,^49^ which have led to the identification of several novel mutations associated with NTDs. ^50-57^ Advances in prenatal diagnosis made it possible not only to detect spina bifida earlier, but also to consider surgical repair before birth.
5. In-Utero Treatment for Spina Bifida
History
Historically, open spina bifida has been managed with postnatal surgical repair, which involves removing exposed tissue, dissecting a connective strand at the base of the spinal cord called the filum terminale, and surgically folding the spinal cord into a tube through a process known as tubularization. While this approach protects the spinal cord and prevents further damage, it does not reverse neurological deficits. Recognizing the limitations of postnatal repair, researchers began exploring the potential of earlier intervention, specifically in-utero surgery, to improve outcomes by halting or reducing neurological injury before birth.
Initial experiments in the 1980s and 1990s demonstrated the feasibility of fetal repair in animal models, including primates,^58^ rats,^59,60^ pigs,^60^ and lambs.^61,62^These promising results paved the way for human trials. In 1997, Meuli-Simmen and colleagues reported the first successful technical attempt at in-utero MMC repair in humans.^63,64^ Early cases faced challenges: the first two fetal surgeries used a maternal skin graft to cover the exposed neural tissue - one baby survived to one year, while the other died due to extreme prematurity.^65^ However, rapid progress followed. By 1998 and 1999, teams at the Children’s Hospital of Philadelphia (CHOP) and Vanderbilt University reported improved outcomes with refined surgical techniques.^66-69^ Later, in 2003, Dr. Harrison’s team at the University of California, San Francisco reported their attempt at fetoscopic MMC repair.^70^ Complete fetoscopic repair was only accomplished in one case, with two other fetuses undergoing partial fetoscopic repair. Dr. Harrison’s team then temporarily abandoned the fetoscopic approach for the remaining 10 fetuses, opting instead to utilize an open approach.^70^ Efforts to optimize fetal surgical techniques culminated in the landmark Management of Myelomeningocele Study (MOMS) trial, published in 2011,^3^ which confirmed that prenatal surgery significantly improves motor outcomes and reduces the need for CSF shunting, marking a turning point in the standard of care. Notable clinical trials advancing prenatal spina bifida repair can be found in Table 1.
The MOMS Trial & Open Hysterotomy Spina Bifida Repair
The MOMS Trial showed that prenatal surgery vastly improved the child’s mental and motor outcomes compared to postnatal surgery.^3^ In the study, clinicians utilized an open-hysterotomy prenatal closure approach, comparing outcomes to children treated postnatally. In this approach, a laparotomy incision is made to expose and exteriorize the uterus. A uterine incision is then made to expose the MMC, using ultrasound to guide the location of the hysterotomy. The neural placode is dissected and dropped into the spinal canal. The dura, skin, and uterus are then closed.^72^ During the MOMS Trial, participating centers coordinated with non-participating centers, who agreed not to perform
The MOMS Trial demonstrated remarkable results, and in fact was stopped early due to the efficacy of prenatal MMC repair over postnatal repair, particularly in terms of hindbrain herniation reversal and hydrocephalus. Prenatally repaired children required hydrocephalus management by CSF diversion via shunt placement at less than half the rate of postnatally repaired children (40% vs. 82%). Partial or total hindbrain herniation reversal was also markedly different, with 75% of prenatally repaired children showing no moderate or severe hindbrain herniation and 36% showing complete hindbrain herniation resolution, compared to 33% and 4% of postnatally repaired children, respectively. The incidence of brainstem kinking was also lower in prenatally repaired children (20% vs. 49%), as was abnormal 4^th^ ventricular location (46% vs. 72%) and rates of spinal cord cysts called syringomyelia (39% vs. 58%).^3^ An update was published outlining all 12-month outcome data and expanding upon the initially presented findings. The reduced need for CSF shunting was maintained (44% vs. 83.6%), and this follow-up data revealed that prenatally repaired children also needed fewer shunt revisions after placement (15.4% vs. 40.2%).^73^ Amazingly, even at the 5–10-year follow-up, prenatally repaired children required fewer shunts (49% vs. 85%) and fewer shunt revisions (23% vs. 60%), and the rate of total hindbrain herniation reversal had climbed and remained markedly improved (39% vs. 13%).^74^ Rates of syringomyelia also remained starkly different (59% vs. 81%). Most critically, neonatal death rates remained low and comparable between groups across this time range, with a 95% survival rate in the prenatal surgery group (5 total deaths of 91) and a 97% survival rate in the postnatal surgery group (3 total deaths of 92).^71,74^
As reduced lower body motor function and paralysis are particularly detrimental impacts of spina bifida, MOMS Trial investigators also longitudinally measured motor function improvements, and the results were similarly impressive. 44.8% of prenatally repaired children were walking independently at their 30-month follow-up exam, 27.6% were walking with the assistance of orthotics or devices, and only 27.6% were not walking. In marked contrast, the postnatally repaired group had rates of 23.9% (independent), 35.3% (assisted), and 40.9% (not walking).^75^ Prenatally repaired children also exhibited lower rates of leg-length discrepancy, and required fewer orthopedic treatments with casts or braces at both 12 and 30 months.^77^ In addition, prenatally repaired children demonstrated greater object manipulation, general locomotion and mobility, and stationary motor function than postnatally repaired children. In fact, these improvements in motor function were more often greater than expected and less often worse than expected based on anatomical measures, in comparison to postnatally repaired children.^3,75^ At the 5–10-year follow-up, these differences persisted, and prenatally repaired children were more likely to walk independently, less likely to require a wheelchair, and more likely to be capable of walking outdoors than their postnatally repaired counterparts.^71,74^ These physical improvements translated into greater self-care capabilities. Prenatally repaired children were more competent chewing and swallowing, using a fork, brushing their teeth, washing and drying their hands, removing their socks and shoes, and zipping, showcasing the real-world benefits to these children.^71^ Prenatally repaired children were even found to be taller than their postnatally repaired counterparts.^74^
Besides physical improvements, prenatally repaired children in the MOMS Trial exhibited several mental, developmental, and social improvements, particularly in comparison to the postnatally repaired children. Prenatally repaired children exhibited greater psychomotor development than those repaired postnatally,^3,75^ and greater verbal learning, nonverbal reasoning, and reading scores.^74^ In fact, on cognitive and neurological measures for which prenatally repaired children did not outperform postnatally repaired children, no robust differences were noted besides fine motor control.^74^ Socially and developmentally, prenatally repaired children experienced a higher quality of life with less negative impact on their families, with the differences being maintained through the 5–10-year follow-up.^74,76^
Outside of the MOMS Trial, comparisons of outcomes between postnatal and prenatal repair are still relatively limited.^85^ However, several non-MOMS studies have validated these findings, demonstrating similarly improved neonatal outcomes including a reduced need for a shunt or shunt revision, higher rates of hindbrain herniation resolution, improved neonatal functional level, and shorter length of stay in neonatal intensive care units than postnatal repair.^86-88^ Another study showed that fetal spina bifida repair may also help normalize cerebral blood flow.^89^ Similar benefits to ambulation have been shown in non-MOMS studies as well,^80,90,91^ with one study even showing prenatally repaired children participating in sports activities at later time points.^91^ Non-MOMS studies have found prenatally repaired children exhibit adaptive behavior, executive functioning abilities, neurocognitive outcomes, psychoeducational achievement, and memory scores within the age-matched population norms, albeit with delays or deficits, particularly for children with shunts.^91-93^
Open hysterotomy-based prenatal spina bifida surgery is not without its drawbacks, however (see Table 2). As with many other prenatal surgeries, open MMC repair is more strongly associated with preterm delivery, low birth weight, and other obstetric issues such as uterine rupture, membrane separation or rupture (including preterm premature rupture of membranes or PPROM), maternal pulmonary edema, placental abruption, and oligohydramnios (reduced amniotic fluid) than postnatal repair.^3,67,80,86,88,94,95^However, the risk of some of these complications is notably similar to the risk following classical c-section.^94,96,97^ Prenatal surgery has also been more strongly associated with certain perinatal complications, such as respiratory distress syndrome and bradycardia.^3,80^ Other findings, particularly on urological function post-repair, are mixed. Both MOMS and non-MOMS studies have shown positive findings, such as prenatally repaired children being more likely to void volitionally and have lower rates of urinary tract infection, but there are also negative findings such as a higher prevalence of bladder muscle overactivity compared to postnatally repaired children.^98,99^ As the field of fetal surgery continues to evolve, advancements will likely improve the outlook for mothers and children following open prenatal MMC repair.^100^
Advances in Open Hysterotomy-Based Prenatal MMC Repair
Following the MOMS Trial, inclusion criteria for open prenatal MMC repair have expanded. Although high BMI was initially an exclusion factor, later studies have shown comparable perioperative outcomes in women with higher BMI.^101^ Access has also expanded to include women with gestational diabetes, certain fetal abnormalities, maternal infections and Rh alloimmunization,^4,102^ and discussion continues to be had about further loosening eligibility criteria.^103^ CHOP has also developed a new closure technique, which uses a needlepoint monopolar cautery to raise myofascial flaps, that has been shown to result in reduced rates of CSF diversion, more significant closure, reductions in hindbrain herniation and shunting, and overall improved results.^4,104^ Due to these technical modifications and increased experience, outcomes reported post-MOMS by CHOP have improved. As of 2017, PPROM rates had dropped from the 46% observed in MOMS to 32%, repair site dehiscence (rupture) rates had dropped from 13% to 3.6%, and pulmonary edema, the need for maternal blood transfusion, and severe preterm birth rates all dropped substantially as well.^4,88^
Even postnatal repair continues to improve. Intraoperative neurophysiological monitoring, which has been used extensively in spinal surgery already, has been recently shown to be useful in postnatal neonatal spina bifida repair as well.^105^
Several other approaches in addition to the open hysterotomy-based repair technique have also developed, which offer unique benefits over postnatal and open prenatal repair. These include percutaneous fetoscopic repair, laparotomy-assisted fetoscopic repair, and a percutaneous/mini-laparotomy fetoscopic technique.^78,81,106-111^ Anesthetics and analgesics are administered to both the mother and the fetus during all these procedures.^78,108,112^
Percutaneous Fetoscopic Repair
Percutaneous fetoscopic repair of MMC is a minimally invasive alternative to open fetal surgery that has evolved significantly over time. The procedure involves inserting instruments through small punctures in the maternal abdomen and uterus, dissecting the neural placode, covering it with a patch, and closing the defect, all without a large uterine incision. Unlike open hysterotomy, which requires cesarean section, percutaneous fetoscopic repair allows for vaginal delivery, and has been associated with a lower risk of maternal complications such as uterine thinning, rupture, and pulmonary edema (see Table 2).^113-116^ However, percutaneous fetoscopy carries higher rates of placental abruption, PPROM, and earlier gestational age at delivery, contributing to complications like respiratory distress syndrome, site dehiscence, sepsis, and increased need for CSF diversion.^107,115-118^Despite these risks, some studies have reported better neurological outcomes, including higher rates of hindbrain herniation reversal, urinaryc ontinence, and independent walking compared to open repair.^115,118^
Technological refinements have improved outcomes over time. The technique has been adapted to close larger spinal defects with comparable success, and the gestational age window for surgery has been extended slightly later (to 27+6 weeks) without compromising outcomes, which helps reduce the risk of extreme prematurity.^119,120^ Most recently, hybrid surgical approaches have emerged, aiming to leverage the benefits of both open and fetoscopic techniques while limiting the drawbacks, reflecting the continued drive to optimize safety and effectiveness for both mother and child.
Hybrid Approaches
The hybrid laparotomy-assisted fetoscopic approach, developed in part by Texas Children’s Fetal Center,^79^ combines elements of open and fetoscopic MMC repair. Surgeons begin with a maternal abdominal incision to partially exteriorize the uterus. The membranes are secured to the uterine wall, amniotic fluid is replaced with carbon dioxide, and a fetoscope is inserted. The neural placode is dissected and closed fetoscopically.^81,112^This hybrid repair offers several benefits over earlier techniques. Unlike open surgery, it allows for vaginal delivery and achieves higher gestational age at birth than both open and percutaneous repairs.^80,87,107,116,121-123^ Vaginal delivery following laparotomy-assisted fetoscopic repair has also been associated with shorter length of stay in neonatal intensive care units.^122^ While maternal complication rates (e.g., PPROM, edema, preeclampsia) are generally similar to open repair, laparotomy-assisted fetoscopic is associated with lower rates of uterine thinning or dehiscence.^80^ Neonatal complication rates are similarly very comparable.^80,121^ Though laparotomy-assisted fetoscopic repair takes longer than open repair and initially raised concerns about carbon dioxide use, studies have shown no adverse impact on fetal growth or long-term development.^124^ Importantly, when factors such as gestational age at delivery, age at time of outcome measurement, and presence of hydrocephalus treatment are controlled for, long term motor and neurodevelopmental outcomes are also comparable to open repair.^80,121,125,126^
Over time, technical refinements in the laparotomy-assisted fetoscopic approach have improved results. A multilayered closure technique reduced CSF leakage, skin dehiscence, and tethered cord, while improving rates of hindbrain herniation reversal.^80^ More recently, a California team introduced a “percutaneous/mini-laparotomy” hybrid approach, which uses a small incision and camera port for fetoscopic closure. Early results suggest a lower risk of prematurity than percutaneous repair and the possibility of vaginal delivery, though PPROM remains a challenge.^108^ Together, these innovations reflect the ongoing evolution of fetal surgery, balancing safety and precision while expanding treatment options for spina bifida.
As of 2017, ACOG and NAFTNet recommend providing women with a fetal MMC diagnosis the option to receive open fetal repair. They do not yet recommend fetoscopic fetal repair due to limited data.^127^ Although open fetal surgery is currently recommended by ACOG, emerging bioengineering strategies are introducing new tools and techniques that could further improve outcomes. Several surgical approaches are shown in Table 2.
6. In-Utero Treatment for Spina Bifida: Recent Advancements of Note
Additional improvements to open and fetoscopic approaches, as well as to postnatal repair procedures not outlined above have improved the outcomes and processes further. Modified closure techniques have also been tested since the MOMS trial. Two-layer closure (myofascial and skin) has been shown to improve watertightness and outcomes,^128^ and another more recently developed 3-port, 3-layer fetoscopic repair technique may further improve outcomes and lead to higher rates of watertight closure.^129,130^ MOMS3, a follow-up of MOMS participants in teen and young adult years, is also currently planned and enrolling study participants.^131^There are also numerous groundbreaking advancements being developed that make use of stem cells and bioengineered tissues, and which leverage other technological modalities such as robotics, 3D printing, and plastic surgery.
Stem Cell and Biomaterials Based Approaches
Stem cells, tissue engineering, and biomaterials-based advances have continued to drive fetal spina bifida repair forward.^132-134^ In 2008, the concept of applying neural stem cells to spina bifida defects to aid in repair was validated in an animal model. Authors showed that application of stem cells to induced MMC defects in a lamb model led to the local production of neurotrophic factors.^135^ This approach has since been built upon with the use of early gestational placental mesenchymal stromal cells (PMSCs) in prenatal MMC repair. These PMSCs are isolated from placental chorionic villus tissue and can be subsequently expanded and banked.^136^ The cells can then be seeded into an extracellular matrix delivery vehicle which is applied to the defect. In mouse^137^ and sheep^138-143^ models, this approach has shown promising results. Now, a clinical trial is currently underway at UC Davis Health called the “CuRe Trial: Cellular Therapy for In Utero Repair of Myelomeningocele”, which uses the approach outlined above to complement fetal surgery for spina bifida treatment. Robbie, the first baby who received this treatment, moved her legs and wiggled her toes after birth, and is thus far in very great health. Robbie is now crawling and kicking, and other babies have undergone the same treatment as the trial continues.^83,84^ See Supplemental video 1 (https://discoveriesjournals.org/art/Suppl/Supplemental%20Video1-CuReTrial.mp4) for an animation of the procedure used in the CuRe Trial.^144^
Another stem cell-based advancement in development is the use of transamniotic stem cell therapy (TRASCET)^145^as an alternative to open fetal MMC repair. TRASCET involves harnessing and augmenting biological roles of specific fetal stem cells – in the context of spina bifida, placental-, amniotic fluid-, or bone marrow-derived stem cells – to exert therapeutic benefits. Rat and rabbit models utilizing this approach have shown promising results, with higher rates of partial or complete defect coverage and reductions in hindbrain herniation rates.^146-151^Other stem cell-based advancements under investigation include differentiation of human induced pluripotent stem cells into neural crest stem cells for implantation into MMC defects, which has also been shown to be feasible in a lamb model;^152^ differentiation of amniotic fluid-derived stem cells into keratinocytes;^153^ and use of fibroblasts and keratinocytes to bioengineer lab-grown fetal skin, which has been demonstrated in lamb models as well.^154^
Other advancements in patch development and defect coverage are also being investigated. One such approach involves the use of basic fibroblast growth factors, delivered via an extracellular gelatin matrix for coverage of the spina bifida defect. In 2010, researchers at CHOP demonstrated preliminary success in adhering their growth factor-crosslinked hydrogel sponge scaffold to the MMC defect in a rat model, with evidence of tissue ingrowth and angiogenesis.^155^ They then went on to show equivalent effectiveness between this gelatin sponge and gelatin microspheres.^156^ More recently, in 2016, these researchers reported feasibility of this approach in a sheep model,^157^ complementing their previous work in rats. Another group at Yale is also investigating growth factor-based defect coverage and has shown success in rat models.^158^The feasibility of covering the defect using collagen-, small intestinal submucosa-, silicone, polypropylene or high-density polyethylene-, amniotic membrane-, biosynthetic cellulose-, and nanofiber-based scaffolds/patches, has also been shown in experimental animal models, and in some cases human patients.^110,159-171^Defect coverage using umbilical cord-derived patches has also been shown to be successful in both rat^172^ and sheep^173-177^ models and in human fetal spina bifida repair.^178^ There is currently an active clinical trial attempting to show feasibility of coverage of spina bifida defects with these patches as well.^82^
Plastic Surgery, Robotic Surgery, and 3D Printed Materials
Outside of biomaterials, technological and engineering innovations have steadily enhanced prenatal MMC repair. In Zurich, researchers successfully demonstrated the first in-utero use of pedicled random pattern transposition flaps - which have been commonly used in adult and pediatric surgeries - for closing spinal defects, with minimal complications.^179^ Robotic-assisted fetal surgery is another promising frontier.^15,180^ Although not yet standard, multiple animal studies have shown the feasibility of robot-assisted endoscopic repair,^181-184^ including novel methods using customized magnetic catheters to improve precision.^184^ A major milestone came with the 2025 “Fetoscopic Robotic Open Spina Bifida Treatment” (FROST) study, which showcased the integration of robotics and 3D printing. Researchers created lifelike, 3D-printed uterine models, including a silicone fetus and placenta, to train surgeons in robot-assisted MMC repair. After 15–21 simulations, the surgeons could competently perform mock procedures.^185^ Possible use of 3D printed materials in training contexts such as these was discussed at a teaching session at the 2018 EuroCMR/SCMR joint congress, at which clinicians agreed that there were potential applications for these materials.^186^ But use cases have expanded beyond training, and 3D printing is now being used to assess patch requirements and build patient-specific models for surgical planning.^187,188^ These advancements highlight how technology is driving safer, more effective, and increasingly personalized approaches to fetal spina bifida repair. The fruits of this can be seen not only in the United States, but internationally as well.
International Adoption
International adoption of prenatal spina bifida repair has also progressed, though variability exists in terms of inclusion and diagnostic criteria, surgical techniques, perioperative management strategies, and neonatal resuscitation practices.^189-192^ Despite this variability, there has also been increasing collaboration between prenatal MMC repair centers in different countries, and the development of more multidisciplinary approaches and teams.^193^ Several non-U.S. countries are continuing to expand access to prenatal MMC repair and have seen improvements in outcomes over time, including (but certainly not limited to) Germany,^194-198^ Brazil,^78,111^ Taiwan,^199^ Canada,^200,201^ France,^202,203^ and Israel.^204^As prenatal repair of MMC expands to more countries and healthcare systems, it also raises important ethical questions about risk, access, and responsibility.
7. Unresolved Challenges
Limitations of Recent Advances
The advances outlined above have resulted in remarkable progress. However, they are not without limitations. Some, but not all the new techniques and technologies have been validated in humans, raising questions about translatability. For those which have shown applicability in human patients, limited data and small sample sizes of existing trials and studies must also be considered. As additional data are collected demonstrating safety and efficacy, it is likely that these novel interventions will need to roll out in waves. Eligibility criteria will start relatively narrow and expand over time, as has been the case for prenatal surgical approaches outlined above. Regulatory hurdles should also be considered and foreseen. These approaches not only utilize biomaterials but also involve treatment of the most vulnerable group of people, unborn children, and therefore will understandably be met with scrutiny by regulatory agencies. While this scrutiny is crucial in ensuring that pregnant women and their children are protected, it will likely slow progress towards therapeutic advancements. Unresolved challenges exist not only pertaining to recent advances, but also to existing treatments and their availability.
Limited Domestic Access to Prenatal MMC Repair
Although adoption of in-utero MMC repair has grown in the United States, access remains limited. A 2024 national survey found that only 31% of U.S. hospitals offered both prenatal and postnatal MMC repair, while the majority provided postnatal repair only.^205^One way by which access could be increased would be expansion of insurance coverage to support maternal travel to specialized centers offering prenatal MMC repair. Given the compelling evidence that prenatal repair significantly improves neurodevelopmental outcomes and mobility while reducing the long-term need for interventions such as shunting and catheterization, these benefits would translate not only to enhanced quality of life for affected children and their families but also to substantial healthcare cost savings over a lifetime.
Maternal Complications vs. Fetal Benefit
The main drawback of in-utero spina bifida repair is the incidence of negative maternal outcomes, as outlined above. The ethics of fetal surgery have been discussed at greater length elsewhere,^206,207^ but frequently discussed considerations include the weighing of risks to the mother against the benefits to the fetus. As with many other fetal surgical interventions, fetal MMC repair comes with risks of preterm birth, ruptured membranes, dehiscence, and other obstetric complications. Though as noted, the risk of some of these complications such as rupture are similar to typical c-section rates.^94,96,97^ Each of the approaches outlined above come with benefits and drawbacks, with some (such as the percutaneous/mini-laparotomy approach) having much lower risks of uterine dehiscence, and others (such as the laparotomy-assisted fetoscopic approach) having lower risks of premature birth. As these techniques continue to develop further, it is possible that new, hybrid approaches will be able to further limit drawbacks while continuing to draw on the strengths of different techniques. However, these obstetric complications must also be viewed considering the reality that during a pregnancy, doctors and surgeons are treating two patients – the mother and her unborn child.^208-210^ In the words of the “Father of Fetal Surgery” himself, “The fetus is no longer a medical recluse hidden inside an opaque womb. The fetus is a patient with problems that cannot only be examined by an array of prenatal tests, but also can be actively managed by arranging the timing, mode, and place of delivery. In a few cases, the fetal problem can even be treated before birth”.^210^ For this second patient, prenatal surgery offers an option besides termination and a markedly improved quality of life.
8. Conclusions
Our understanding of spina bifida has greatly improved over the past several decades, with advances being made from prevention to diagnosis and management. A better grasp on the preventative roles of folic acid has allowed fewer cases of spina bifida to manifest in the first place. This highlights that clinicians worldwide should encourage folic acid supplementation prior to and during pregnancy. Improved imaging and diagnostics have allowed for more rapid and accurate identification of those cases which do manifest. Clinicians are now equipped with a multitude of techniques to repair the defect in utero, as new, hybrid approaches continue to develop to harness the benefits and limit the drawbacks of each. In practice, the findings of this review and the broader literature will inform the selection of surgical techniques by clinicians based upon each woman’s circumstances and risk profile. As the field moves forward, improvements will continue to be made. Stem cells and other biomaterials, robotic surgeries, 3D printing, improved imaging and diagnostic markers, and other refinements in technology and technique have consistently pushed the limits of what is possible. Further work is needed to expand treatment availability so that more expecting mothers and their unborn children can access the fruits of this advancing field and pursue positive outcomes for both patients.
Key Points
Clinicians now recognize the fetus as a patient in their own right.
Folic acid supplementation plays an important role in spina bifida prevention worldwide.
Prenatal surgical approaches for myelomeningocele (MMC) have evolved and continue to evolve, expanding treatment options and improving outcomes for both mother and child.
Author Contributions
Conceptualization, Z.B.S.; writing - original draft preparation Z.B.S.; writing - review and editing, Z.B.S. and K.E.F.; figure preparation, K.E.F.; project administration, Z.B.S. All authors have read and agreed to the published version of the manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Birth Prevalence of Spina Bifida by Folic Acid Fortification Status: A Systematic Review and Meta-Analysis.1e 2434 Atta Callie A M Fiest Kirsten M Frolkis Alexandra D Jette Nathalie Pringsheim Tamara St Germaine-Smith Christine Rajapakse Thilinie Kaplan Gilaad G Metcalfe Amy American journal of public health 10620162656212710.2105/AJPH.2015.302902 PMC 4695937 · doi ↗ · pubmed ↗
- 2National population-based estimates for major birth defects, 2016-2020.1e 2301 Stallings Erin B Isenburg Jennifer L Rutkowski Rachel E Kirby Russell S Nembhard Wendy N Sandidge Theresa Villavicencio Stephan Nguyen Hoang H Mc Mahon Daria M Nestoridi Eirini Pabst Laura J Birth defects research 11620243827740810.1002/bdr 2.2301 PMC 10898112 · doi ↗ · pubmed ↗
- 3A randomized trial of prenatal versus postnatal repair of myelomeningocele.119931004 Adzick N Scott Thom Elizabeth A Spong Catherine Y Brock John W Burrows Pamela K Johnson Mark P Howell Lori J Farrell Jody A Dabrowiak Mary E Sutton Leslie N Gupta Nalin Tulipan Noel B D'Alton Mary E Farmer Diana L The New England journal of medicine 36420112130627710.1056/NEJ Moa 1014379 PMC 3770179 · doi ↗ · pubmed ↗
- 4Fetal surgery for myelomeningocele: After the Management of Myelomeningocele Study (MOMS).6360366 Moldenhauer Julie S Adzick N Scott Seminars in fetal & neonatal medicine 2220172903153910.1016/j.siny.2017.08.004 · doi ↗ · pubmed ↗
- 5Embryology, Neural Tube Singh Ranbir Munakomi Sunil Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 542285/
- 6The Developing Human: Clinically Oriented Embryology. 12th edition. Torchia Persaud Elsevier 2024
- 7Critical appraisal on neural tube defects and their complexities.6515521 Shaikh Fouziya Sanadhya Mallica Kaleem Safa Verma Tiya Jayaraj Richard L Ahmad Faizan Pediatrics and neonatology 6620254027446910.1016/j.pedneo.2024.07.015 · doi ↗ · pubmed ↗
- 8Spina Bifida Prevention: A Narrative Review of Folic Acid Supplements for Childbearing Age Women.1e 53008 Ledet Iii Lloyd F Plaisance Connor J Daniel Charles P Wagner Maxwell J Alvarez Ivan Burroughs Caroline R Rieger Ross Siddaiah Harish Ahmadzadeh Shahab Shekoohi Sahar Kaye Alan D Varrassi Giustino Cureus 1620243840608210.7759/cureus.53008 PMC 10894015 · doi ↗ · pubmed ↗