Analysis of factors influencing weight regain after bariatric-metabolic surgery in obesity hypoventilation syndrome patients based on gastrointestinal peptide hormones
Jingjing Zhang, Shadike Apaer, Shuo Zhang, Guanyou Liang, Tao Li, Xinling Cao

TL;DR
This study examines how gastrointestinal hormones and lifestyle factors affect weight regain in patients with obesity hypoventilation syndrome after bariatric surgery.
Contribution
The study identifies specific gastrointestinal peptide hormones and lifestyle factors as predictors of weight regain after bariatric surgery in OHS patients.
Findings
Levels of INS, Lep, and GLP-1 increased while ghrelin decreased after surgery.
Unfavorable diet, lack of exercise, trace element deficiencies, and negative emotions were independent risk factors for weight regain.
Gastrointestinal peptide hormones showed strong predictive value for postoperative weight regain.
Abstract
Obesity is becoming increasingly prevalent in modern society, leading to a rise in the incidence of obesity hypoventilation syndrome (OHS). This study analyzes the factors influencing weight regain in OHS patients following laparoscopic sleeve gastrectomy (LSG), based on gastrointestinal peptide hormones. A total of 134 OHS patients who underwent LSG at our hospital between January 2023 and January 2024 were enrolled. The alterations in gastrointestinal peptide hormones, including insulin (INS), leptin (Lep), glucagonlike peptide-1 (GLP-1), and ghrelin (GHR), before and after surgery were measured. Subsequently, a 6-month followup was conducted. Patients with weight regain were identified, and the predictive value of gastrointestinal peptide hormones for weight regain was analyzed. Logistic regression was then employed to analyze the related factors affecting weight regain. Following…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
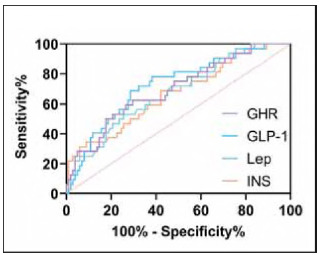 Figure 1
Figure 1| Before treatment (n = 134) | After treatment (n = 134) | t |
| |
|---|---|---|---|---|
| INS (pg/mL) | 262.18±21.57 | 317.56±37.33 | 14.873 | <0.001 |
| Lep (pg/mL) | 5.84±0.90 | 7.48±1.36 | 11.727 | <0.001 |
| GLP-1 (pg/mL) | 87.12±10.59 | 100.56±10.36 | 10.501 | <0.001 |
| Not regaining weight (n = 102) | Weight regains (n=32) | t |
| |
|---|---|---|---|---|
| INS (pg/mL) | 323.31±36.08 | 299.25±35.80 | 3.297 | 0.001 |
| Lep (pg/mL) | 7.70±1.33 | 6.81±1.24 | 3.351 | 0.001 |
| GLP-1 (pg/mL) | 102.40±10.30 | 94.71±8.25 | 3.847 | <0.001 |
| GHR (pg/mL) | 223.75±19.42 | 237.84±17.86 | 3.647 | <0.001 |
| Cut-off | Sensitivity (%) | Specificity (%) | AUC |
| |
|---|---|---|---|---|---|
| INS (pg/mL) | <315.60 | 68.75 | 57.84 | 0.665 | 0.005 |
| Lep (pg/mL) | <6.93 | 53.13 | 74.51 | 0.676 | 0.003 |
| GLP-1 (pg/mL) | <96.99 | 68.75 | 71.57 | 0.724 | <0.001 |
| GHR (pg/mL) | >233.80 | 62.50 | 70.59 | 0.696 | <0.001 |
| Not regaining weight (n=102) | Weight regains (n=32) | χ2/t |
| |
|---|---|---|---|---|
| Sex (male/female) | 59/43 | 16/16 | 0.608 | 0.436 |
| Ape | 48.47±8.14 | 48.38±5.77 | 0.062 | 0.951 |
| TWL (%) | 25.03±7.84 | 26.29±7.96 | 0.786 | 0.433 |
| BMI before surgery (kg/m2) | 35.71±3.00 | 36.17±2.66 | 0.785 | 0.434 |
| Neck circumference (cm) | 46.02±4.92 | 45.94±6.03 | 0.078 | 0.938 |
| Chest circumference (cm) | 119.67±8.84 | 122.47±16.42 | 1.247 | 0.215 |
| Waist circumference (cm) | 119.58±7.95 | 123.03±12.44 | 1.852 | 0.066 |
| Hip circumference (cm) | 122.78±12.26 | 124.78±12.41 | 0.802 | 0.424 |
| SBP (mmHp) | 138.66±12.38 | 137.66±17.13 | 0.362 | 0.718 |
| DBP (mmHp) | 85.75±8.72 | 87.94±10.78 | 1.170 | 0.244 |
| Unhealthy eating habits (often/occasionally/rarely) | ||||
| Irregular eating | 24/36/42 | 15/9/8 | 6.642 | 0.036 |
| Binge eating | 20/39/43 | 12/15/5 | 8.5.03 | 0.014 |
| Nocturnal eating | 19/31/52 | 10/14/8 | 6.759 | 0.034 |
| Hiph-sugar/fat foods | 24/37/41 | 12/16/4 | 8.494 | 0.014 |
| Smoking (yes/no) | 51/51 | 19/13 | 0.858 | 0.354 |
| Sleep (normal/abnormal) | 69/33 | 17/15 | 2.234 | 0.135 |
| Exercise habits (yes/no) | 39/63 | 3/29 | 9.428 | 0.002 |
| Micronutrients (deficient/normal) | 20/82 | 12/20 | 4.290 | 0.038 |
| SAS | 31.13±8.94 | 40.25±8.73 | 5.064 | <0.001 |
| SDS | 32.90±8.34 | 40.00±9.88 | 4.015 | <0.001 |
| Factors | Assignment |
|---|---|
| Weight regains | No=1, yes=2 |
| Irregular eating, Binge eating, Nocturnal eating, <br>High-sugar/fat foods | Often=3, occasionally=2, rarely=1 |
| Exercise habits | Yes=1, no=2 |
| Micronutrients | Deficient=2, normal = 1 |
| Gastrointestinal peptide hormones, SAS, SDS | Use of raw data |
| Factors | B | S.E | Wals |
| Exp (B) | 95%Cl |
|---|---|---|---|---|---|---|
| Irregular eating | 0.736 | 1.301 | 3.543 | 0.060 | 1.087 | 0.002—1.136 |
| Binge eating | 3.943 | 1.468 | 7.209 | 0.007 | 5.566 | 2.900—16.885 |
| Nocturnal eating | 1.940 | 1.353 | 2.056 | 0.152 | 2.413 | 0.491—4.583 |
| Hiph-sugar/fat foods | 1.975 | 1.310 | 12.273 | <0.001 | 2.467 | 1.533—3.985 |
| Exercise habits | 4.216 | 1.823 | 5.345 | 0.021 | 1.900 | 1.762—4.790 |
| Micronutrients | 1.172 | 1.151 | 10.022 | <0.001 | 1.843 | 1.288—8.034 |
| SAS | 0.215 | 0.077 | 7.724 | 0.007 | 1.240 | 1.066—1.444 |
| SDS | 0.174 | 0.064 | 7.403 | 0.005 | 1.190 | 1.050—1.349 |
| INS | -0.024 | 0.014 | 13.030 | <0.001 | 0.916 | 0.642—0.991 |
| Lep | -0.889 | 0.379 | 5.502 | 0.019 | 0.411 | 0.196—0.864 |
| GLP-1 | -0.108 | 0.046 | 5.474 | 0.019 | 0.898 | 0.821—0.983 |
| GHR | 0.080 | 0.43 | 9.473 | <0.001 | 1.264 | 1.083—1.843 |
- —State Key Laboratory of Pathogenesis, Prevention and Treatment of High Incidence Diseases in Central Asia, Xinjiang Medical University (No.SKL-HIDCA-2023-26)
- —Xinjiang Medical University Student Innovation and Entrepreneurship Training Program (No. S202410760073)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiet and metabolism studies
Introduction
Obesity, defined as the abnormal or excessive expansion of white adipose tissue, has reached pandemic proportions and is recognized as a crucial health concern [1]. Extensive clinical research has firmly established that the obese population faces a markedly elevated risk of developing various conditions, including cardiovascular diseases [2], digestive tract disorders [3], infertility [4], and fractures [5], when compared to the general population. At present, the global prevalence of obesity is on an upward trajectory, particularly in developed countries. For example, approximately 42% of the U.S. population has a body mass index (BMI) greater than 30, while 9.4% of the population has a BMI exceeding 4 [6]. While the majority of obese individuals can potentially achieve weight reduction through exercise-based interventions, surgical weight loss procedures are indicated for those with concomitant organ dysfunctions [7]. Among these, obesity hypoventilation syndrome (OHS) stands out as a representative disorder in obese patients. Clinically, it has been well-established that the pathological mechanism of OHS primarily involves a decline in chest wall compliance and restricted diaphragmatic mobility induced by obesity. If not treated promptly, OHS may progress to respiratory failure, thereby posing a serious threat to the patient's life and safety [8]. Given the limitation of respiratory function in OHS patients, exercise-based therapeutic approaches are not suitable for them. With the continuous advancement of medical technology, laparoscopic sleeve gastrectomy (LSG) has witnessed an increasing application in the treatment of OHS in recent years [9]. By modifying the anatomical structure of the gastrointestinal tract and curtailing nutrient intake and absorption, LSG can effectively and rapidly achieve weight reduction and rectify obesity-associated metabolic disorders [10]. Nevertheless, approximately 25% of patients experience weight regain following LSG. Thus, the resolution of this problem remains a pivotal focus of current clinical research.
Recent research indicates that the gastrointestinal tract and the central nervous system interact closely via the autonomic nervous system, the brain-gut peptide transmitter system, and other neuroendocrine networks. This phenomenon is termed the brain-gut axis [11]. Following LSG, significant alterations in the brain-gut axis occur in patients, which may be a crucial factor contributing to weight regain. However, this hypothesis remains unsubstantiated by definitive research. Gastrointestinal peptide hormones are known to play a central role in brain-gut axis interactions by regulating appetite, energy metabolism, gastrointestinal motility, and mood [12]. For example, glucagon-like peptide-1 (GLP-1) suppresses appetite by acting on the arcuate nucleus of the hypothalamus, inhibiting neuropeptide Y (NPY) and acanthamoeba-associated protein (AgRP) neurons, and activating neurons of pheomelanocortino- gen (POMC) [13]. Leptin (Lep) suppresses appetite and increases mood by acting on the hypothalamic leptin receptors, suppressing appetite and increasing energy expenditure [14]. Studies have confirmed that gastrointestinal peptide hormones have a direct relationship with carbohydrate and fat metabolism in humans [15], which suggests the promise of our gastrointestinal peptide hormones as a clinical assessment indicator for regaining weight.
Consequently, this study aims to analyze the factors influencing weight regain after LSG in OHS patients based on gastrointestinal peptide hormones. The findings are expected to offer more reliable and safer clinical guidance for the future implementation of LSG.
Materials and methods
Research subjects
This study enrolled patients diagnosed with OHS who underwent LSG at our institution between January 2023 and May 2024. Based on the sample-size calculation formula for sampling surveys, N = (Z^2^ x σ^2^)/d^2^ (Confidence interval Z = 1.96, σ=0.5, overall standard deviation σ=0.5, error d = 10%), a minimum of 96 participants were determined to be necessary for this study. Subsequently, well-defined inclusion and exclusion criteria were formulated.
Inclusion criteria:
(1) Availability of complete clinical records without missing data.(2) BMI > 30 kg/m^2^, with awake arterial carbon dioxide tension (PaCO_2_) ≥ 45 mmHg, accompanied by significant hypoventilation.(3) Absence of preoperative interventions that could influence gastrointestinal hormone levels.(4) Postoperative percent excess weight loss (EWL%) exceeding 50%.
Exclusion criteria:
(1) Comorbid conditions such as chronic obstructive pulmonary disease, or pulmonary hypertension that could impair ventilation.(2) Active inflammatory or intestinal diseases.(3) Diagnosed psychiatric disorders.(4) History of gastrointestinal surgery within the preceding six months.(5) Use of medications affecting the central nervous system within the past six months.(6) Inability to complete follow-up assessments for prognosis evaluation.
After strict screening according to these criteria, a total of 134 subjects were finally enrolled. The study protocol was approved by the Institutional Ethics Committee (Approval number:250303-245), and written informed consent was obtained from all participants. Moreover, the entire research process adheres strictly to the principles outlined in the Declaration of Helsinki.
Sample collection
Baseline data, including age and gender, were collected from all patients. Body measurements such as BMI, waist circumference, chest circumference, and hip circumference were recorded both preoperatively and on the 7th day postoperatively. Subsequently, 3-5 mL of early-morning elbow venous blood samples were collected from all patients upon admission and 7 days after the surgical procedure. After centrifugal separation of the serum, the concentrations of insulin (INS), Lep, GLP-1, and ghrelin (GHR) were determined using the enzyme-linked immunosorbent assay (ELISA) method.
Prognostic follow-up
All patients underwent a 6-month prognostic follow-up following LSG. The follow-up was implemented through regular hospital visits at a frequency of once per month. Follow-up included the patient's height and weight, distance from the patient's regained weight. (1) rebound of ≥10%-15% of the lowest postoperative weight; or (2) rebound of more than 25% of the excess preoperative weight; or (3) increase in BMI of ≥5 kg/m^2^ from the lowest postoperative value or BMI≥30 kg/m^2^; or (4) regain of ≥80% of the preoperative weight. Fulfillment of any of the above criteria was judged as regaining weight [16].
Observation indicators
The alterations in gastrointestinal peptide hormone levels before and after surgery were recorded. Additionally, the predictive mechanism of these gastrointestinal peptide hormones regarding prognostic weight regain was comprehensively analyzed. Finally, factors influencing prognostic weight regain in patients were investigated.
Statistical analysis
All statistical analyses were performed using SPSS 22.0 software. After the Shapiro-wilk test, it was confirmed that all the measurement data were normally distributed. Measurement data were expressed as mean ± standard deviation (x̄±s), and comparisons between groups were conducted using t-tests or Mann-Whitney U tests. Categorical data were expressed as frequencies and percentages [n(%)], and inter-group comparisons were performed using chi-square tests (χ^2^) or Fisher's exact tests. The Receiver operating characteristic (ROC) curve is used to analyze the predicted value, and the cut-off value is determined based on the largest Youden index scale as well as the Area under curve (AUC). Multivariate logistic regression analysis was employed to identify independent risk factors for weight regain. Statistical significance was set at a P-value < 0.05.
Results
Changes in gastrointestinal peptide hormones before and after surgery
Compared to preoperative levels, postoperative levels of NS, Lep, and GLP-1 were significantly increased, while GHR levels were decreased (P < 0.05, Table 1). These findings indicate a correlation between gastrointestinal peptide hormones and the process of LSG.
Association between gastrointestinal peptide hormones and weight regain
Prognostic follow-up results indicated that 32 out of 134 patients experienced weight regain, corresponding to a weight regain rate of 23.88%. Patients who regained weight demonstrated significantly lower levels of INS, Lep, and GLP-1, as well as elevated levels of GHR, compared to those without weight regain (P < 0.05, Table 2). These results suggest that gastrointestinal peptide hormones may be implicated in the mechanisms underlying weight regain.
Predictive value of gastrointestinal peptide hormones for weight regain
ROC curve analysis further revealed that INS, Lep, GLP-1, and GHR all exhibited strong predictive value for post-LSG weight regain (P < 0.05, Figure 1 and Table 3). Notably, GLP-1 demonstrated the highest predictive efficacy, with an AUC of 0.724, sensitivity of 68.75%, and specificity of 71.5%.
ROC curve of gastrointestinal peptide hormones for predicting weight regain.
Univariate analysis of factors associated with weight regain
Comparative analysis of baseline characteristics between patients with and without weight regain revealed no significant differences in postoperative sex, waist circumference, or chest circumference (P > 0.05). However, in the comparison of poor dietary habits, there was a significant difference between re-fatting patients and non-re-fatting patients (P < 0.05). At the same time, the number of patients with no exercise habits and micronutrient deficiencies was more than that of patients who had not regained weight, and the SAS and SDS were higher (P < 0.05, Table 4).
Multivariate analysis of factors associated with weight regain
We assigned values to the above single-factor indicators and gastrointestinal peptide hormones that differed from each other (Table 5), and logistic regression analysis was performed with regaining weight as the independent variable and single-factor indicators as the covariates. The results, as shown in Table 6, showed that gastrointestinal peptide hormones, poor dietary habits, and micronutrient deficiencies were all independent risk factors affecting patients' regaining weight, while maintaining exercise habits was an independent protective factor for regaining weight (P < 0.05).
Discussion
As obesity becomes increasingly prevalent in modern society, the incidence of OHS has also risen steadily [17]. Although LSG effectively alleviates obesity-related ventilation dysfunction in OHS patients, postoperative weight regain remains a significant concern. To address this issue, this study investigated the factors influencing weight regain in OHS patients, with a focus on gastrointestinal peptide hormones. The key findings are summarized below:
The aim of this study was to assess the likelihood of obesity recurrence in patients at an early stage after receiving LSG by means of gastrointestinal peptide hormone levels, thus providing a clinical reference point and thus early intervention. Therefore, the samples were all collected mainly before and after LSG. Firstly, our observations indicated that following LSG in OHS patients, the levels of INS, Lep, and GLP-1 increased, while GHR levels decreased, suggesting an underlying correlation between these gastrointestinal peptide hormones and obesity progression. Previous research has demonstrated that these hormones modulate appetite and feeding behavior by regulating hypothalamic activity. Specifically, INS, Lep, and GLP suppress appetite and feeding, whereas GHR promotes them. As such, the dysregulation of gastrointestinal peptide hormones is regarded as a key factor contributing to energy metabolism imbalance in obese patients [18]. We posit that LSG, by altering the gastrointestinal anatomy, regulates the levels of these hormones, thereby influencing the gut-brain axis [19]. Additionally, this study revealed a strong correlation between gastrointestinal peptide hormones and post-LSG weight regain, with the hormones showing remarkable predictive value. This can be attributed to the well-established physiological principle that body weight is regulated by hormones [20]. Bariatric-metabolic surgeries induce significant alterations in the normal structure and function of the gastrointestinal tract, as well as modulate the secretion of gut hormones. Research by Carvalho C et al. [21] revealed that patients undergoing LSG and Roux-en-Y gastric bypass exhibit elevated postprandial serum GLP-1 levels, with these changes potentially persisting over the long term. Furthermore, bariatric surgery has been shown to increase levels of peptide YY, suppress the Y2 receptor in the hypothalamic arcuate nucleus, and reduce the expression of gamma-aminobutyric acid, neuropeptide Y, and agouti-related protein. This cascade of effects activates adjacent pro-opiomelanocortin neurons, initiating a series of signaling pathways that suppress appetite and promote weight loss [22]. In addition, altered intestinal flora may affect the production of short-chain fatty acids (SCFAs) [23], and SCFAs may stimulate GLP-1 secretion [24]. If the flora is dysbiot- ic, SCFAs decrease and GLP-1 secretion declines, which may also be one of the mechanisms by which GLP-1 affects weight regain. In essence, gastrointestinal peptide hormones like GLP-1 are crucial for maintaining long-term weight stability in post-surgical patients. Once this balance is disrupted, patients' appetite and nutrient absorption capabilities reactivate, resulting in weight regain [25]. In the study by Çalik Basaran N et al. [26], GLP-1 was identified as a risk factor for weight regain following bariatric surgery, aligning with our findings. Building on these results, Jensen AB et al. [27] have proposed that GLP-1 receptor agonists represent a promising therapeutic strategy for achieving sustained weight control after bariatric-metabolic surgery. Nevertheless, further clinical trials are necessary to validate their efficacy and facilitate broader clinical application.
Apart from gastrointestinal peptide hormones, we must not overlook other factors associated with weight regain. The results of this study indicated that unfavorable dietary habits—including binge eating and a preference for high-sugar and high-fat foods—are risk factors for weight regain. These habits are widely recognized as the most direct lifestyle contributors to obesity [28] [29]. Additionally, a lack of regular exercise is identified as a factor that increases the risk of weight regain. Research by van Baak MA et al. [30] found that patients who engaged in regular physical activity after bariatric-metabolic surgery experienced greater weight loss over time. However, some studies suggest that exercise is not associated with weight regain following such surgeries [31]. This discrepancy may be attributed to the lack of standardized criteria for defining weight regain after bariatric surgery, as well as variations in exercise intensity, duration, and modalities across different studies. Exercise has long been known for its positive effects in improving physical fitness and maintaining health. Regular moderate-intensity exercise improves all aspects of human health and is widely accepted as a preventive and therapeutic strategy for a variety of diseases [32]. Therefore, we prefer to advocate our patients to maintain a good exercise habit. Moreover, trace element deficiencies are also an independent factor influencing weight regain, as trace elements play a critical role in regulating metabolism, hormones, and energy balance in patients. Research has confirmed that trace element deficiencies are prevalent among individuals with obesity [33]. Therefore, addressing these deficiencies is essential for maintaining long-term weight stability and overall health after bariatric-metabolic surgery. Finally, we found that low scores on the Self-Rating Anxiety Scale (SAS) and Self-Rating Depression Scale (SDS) increased the risk of weight regain in patients. Research by Mishali M et al. [34] has shown a link between obesity and depression. Depression is associated with unhealthy lifestyles, uncontrolled eating behaviors, and postbariatric weight regain. Obese patients with comorbid depression and anxiety may exhibit intermittent binge eating behaviors, hampering weight control and worsening psychological issues. In light of these findings, for future LSG procedures, we propose: 1. Monitoring patients' gastrointestinal peptide hormone levels regularly to evaluate postoperative weight regain risk. 2. Enhancing health education for patients, including fostering good dietary and exercise habits. 3. Tracking patients' trace element status and intervening with medications when necessary. 4. Prioritizing patients' psychological well-being, offering guidance and support to alleviate negative emotions.
However, factors like fasting plasma glucose (FPG) and glycated hemoglobin (HbAlc), which have been previously identified in similar studies as factors related to weight regain [35] [36], were not associated with weight regain in this study. This discrepancy may be attributed to the fact that the observation indicators in this study were collected 7 days postoperatively, rather than being real-time data from the patients, which might explain the absence of significant differences. The findings of this paper are more oriented towards offering clinical references for the early assessment of weight regain. Of course, in subsequent research, we intend to incorporate patients' real-time data for validation and further analysis based on the above-mentioned results.
Furthermore, another limitation of this study lies in the relatively small sample size, which may introduce contingency in the analysis results. In the future, it is essential to augment the sample size and prolong the research duration to enhance the reference significance of the research findings. Moreover, incorporating a broader range of observational indicators is necessary to offer more comprehensive assessment insights for clinical weight-regain evaluation. As this study was a retrospective analysis, the prognostic follow-up investigation of the patients was not conducted by members of the research team. The routine follow-up in our hospital only included patients' weight and height, and did not detect gastrointestinal peptides, which also resulted in our inability to add dynamic monitoring of prognostic gastrointestinal peptide hormones. Of course, we cannot ignore the potential impact of medication adherence. Although the postoperative medication was the same for all patients (vitamins + protein supplements + proton pump inhibitor + simethicone), we were unable to monitor the patients' actual daily medication after discharge.
Conclusion
Gastrointestinal peptide hormones are intricately linked to weight changes in OHS patients after LSG. In the future, the clinic can provide an early assessment of the risk of prognostic weight regain by detecting patients' gastrointestinal peptide hormone levels after LSG, so that early intervention can be managed. Additionally, unfavorable dietary habits, lack of regular exercise, trace element deficiencies, and negative emotional states are identified as independent risk factors influencing weight regain after LSG. Clinicians are thus urged to attach great importance to these factors.
Dodatak
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding
This study was supported by the State Key Laboratory of Pathogenesis, Prevention and Treatment of High Incidence Diseases in Central Asia, Xinjiang Medical University (No.SKL-HIDCA-2023-26); Xinjiang Medical University Student Innovation and Entrepreneurship Training Program (No. S202410760073).
Acknowledgements
Not applicable.
Conflict of interest statement
All the authors declare that they have no conflict of interest in this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1713202310.3390/biom 13071084 Caruso A Gelsomino L Panza S Accattatis F M Naimo G D Barone I et al Biomolecules Leptin: A Heavyweight Player in Obesity-Related Cancers 37509120 PMC 10377641 · doi ↗ · pubmed ↗
- 2273378202310.1016/j.pcad.2023.04.006 Iacobellis G Prog Cardiovasc Dis Epicardial fat links obesity to cardiovascular diseases 37105279 · doi ↗ · pubmed ↗
- 35732599160202110.1053/j.gastro.2020.10.057 Aron-Wisnewsky J Warmbrunn M V Nieuwdorp M Clément K Gastroenterology Metabolism and Metabolic Disorders and the Microbiome: The Intestinal Microbiota Associated With Obesity, Lipid Metabolism, and Metabolic Health-Pathophysiology and Therapeutic Strategies 33253685 · doi ↗ · pubmed ↗
- 4e 20222784932022 Marinelli S Napoletano G Straccamore M Basile G Acta Biomed Female obesity and infertility: outcomes and regulatory guidance 3604395310.23750/abm.v 93i 4.13466 PMC 9534231 · doi ↗ · pubmed ↗
- 5885589273202210.5603/ep.a 2022.0077 Kupisz-Urbańska M Stuss M Kuryłowicz A Jankowski P Pilz S Sewerynek E et al Endokrynol Pol Fracture risk in obesity: a narrative review 36591811 · doi ↗ · pubmed ↗
- 6311331927202110.1097/mcc.0000000000000823 Kacmarek R M Wanderley H V Villar J Berra L Curr Opin Crit Care Weaning patients with obesity from ventilatory support 33797429 · doi ↗ · pubmed ↗
- 7226223343202410.5937/jomb 0-44411 Ma Q He X Fu Z Ren X Sun R Zhu S Bian Y Li X J Med Biochem Clinical observation of laparoscopic sleeve gastrectomy and metformin treatment in obese PCOS patients 38699692 PMC 11062340 · doi ↗ · pubmed ↗
- 8zpae 03315202410.1093/sleepadvances/zpae 033 Orozco Gonzalez B N Rodriguez Plascencia N Palma Zapata J A Llamas Dominguez A E Rodriguez Gonzalez J S Diaz J M et al Sleep Adv Obesity hypoventilation syndrome, literature review 38966619 PMC 11223067 · doi ↗ · pubmed ↗