Necrotizing Fasciitis Camouflaging As Cellulitis: A Case Report Highlighting Diagnostic Pitfalls
Sakshi Palav, Shravan Gangula, Jyothi R Patri

TL;DR
This case report shows how necrotizing fasciitis can mimic cellulitis, emphasizing the need for early diagnosis and surgical intervention to prevent severe outcomes.
Contribution
The report highlights diagnostic challenges and clinical clues for identifying necrotizing fasciitis in its early stages.
Findings
Necrotizing fasciitis was initially mistaken for cellulitis due to similar early symptoms.
Subcutaneous emphysema on imaging led to the correct diagnosis and urgent surgery.
The case underscores the importance of considering NF in patients with disproportionate pain and risk factors.
Abstract
Necrotizing fasciitis (NF) is a rapidly progressive, life-threatening soft tissue infection that is often misdiagnosed in its early stages due to clinical similarities with cellulitis. Early recognition and prompt surgical intervention are essential to reducing morbidity and mortality. This report presents one case of NF initially manifesting as cellulitis in a patient with multiple risk factors, including intravenous drug use and recent incarceration. Despite initial antibiotic therapy and transient clinical improvement, the patient experienced worsening pain and systemic symptoms. Imaging identified subcutaneous emphysema, leading to urgent surgical exploration that confirmed NF. This case highlights the importance of recognizing disproportionate pain, maintaining a high index of suspicion, and seeking early surgical consultation when NF is considered. The case was managed by family…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1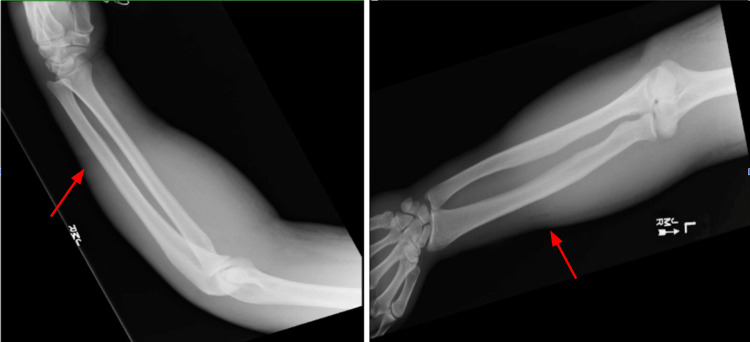 Figure 2
Figure 2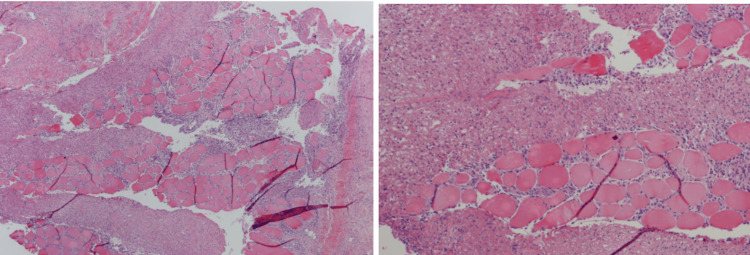 Figure 3
Figure 3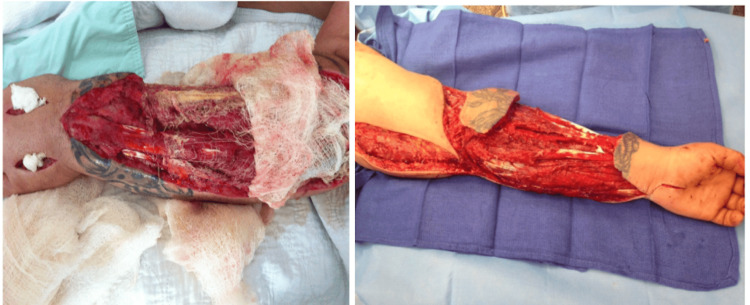 Figure 4
Figure 4| Parameter | Patient value (mg/dL) | Normal range (mg/dL) | Clinical relevance |
| Comprehensive metabolic panel | |||
| BUN | 15 | 6 to 20 | |
| Creatinine | 1.18 | 0.6 to 1.3 | Possibly early renal hypoperfusion |
| Sodium | 134 | 135 to 145 | |
| Potassium | 3.8 | 3.7 to 5.2 | |
| Chloride | 102 | 96 to 106 | |
| Bicarbonate | 24 | 22 to 32 | |
| Glucose | 105 | 70 to 100 | |
| Calcium | 7.9 | 8.5 to 10.2 | Associated with severe infection |
| Complete blood picture | |||
| WBC | 13.6 billion cells/L | 3.4 to 9.6 billion cells/L | Reactive elevation with infection |
| Hemoglobin | 12 grams/dL | 13.2 to 16.6 grams/dL | |
| Hematocrit | 35.8% | 38.3% to 48.6% | |
| Platelets | 178 billion cells/L | 135 to 317 billion cells/L | |
| Neutrophils | 80% | 40% to 60% | Suggestive of bacterial infection |
| Day/hours of case | Symptoms, findings, and treatment performed |
| Day 0 (0 hours) | Onset of pain and swelling |
| Day 1 | Fever and worsening erythema, ED presentation |
| Day 1.5 (36 hours) | CT imaging performed, broad-spectrum IV antibiotics initiated |
| Day 2 | Surgical consultation, irrigation, and debridement × 1 and NF confirmed |
| Day 4 | Second-look debridement, ICU monitoring |
| Day 6 | Irrigation and debridement × 3, clinical stabilization |
| Day 9 | Irrigation and debridement × 4, transition to targeted antibiotics |
| Day 11 | Irrigation and debridement × 5 with Integra placement |
| Day 15 | STSG reconstruction performed |
| Day 16 | Infection resolved, PICC line taken out, patient released with Integra in place, and plastic surgery follow-up in four to six weeks |
| Feature | Cellulitis | Necrotizing fasciitis |
| Pain | Proportional | Out of proportion |
| Progression | Over days (gradual) | Within a few hours (rapid) |
| Systemic toxicity | Mild | Severe |
| CT imaging | No gas | Subcutaneous emphysema |
| Surgical findings | Not required | Diagnostic |
| Diagnostic modality | Salient features | Strengths | Weaknesses |
| Ultrasound | Fascial thickening, fluid collections, early gas | Bedside, no radiation, early clue to gas | Operator-dependent, limited depth, incomplete fascial view |
| Plain radiography (X-ray) | Subcutaneous gas, soft tissue swelling, foreign bodies | Fast, inexpensive, widely available | Low sensitivity, often normal early |
| CT | Gas along fascial planes, fluid tracking, soft tissue changes | Rapid, excellent detail, reliable for gas | Radiation, contrast limits in renal disease |
| MRI | Diffuse fascial edema, clear tissue plane contrast | Most sensitive for soft tissue involvement | Expensive, slow, contraindications (implants, claustrophobic) |
| LRINEC | Integrates CRP and routine labs into a risk score | Quick risk stratification from routine labs | False negatives, cannot replace clinical judgment |
| SIARI | Combines epidemiology + labs for risk estimates | Emerging alternative with promising diagnostic performance | Limited validation, adjunct only |
| Variable | Clinical manifestations |
| Skin | Redness, swelling, tenderness, erythema, increasing temperature of the area, skin discoloration to purple, blue, and black, bullae, edema, skin necrosis, crepitus |
| Pain | Out of proportion, severe at presentation |
| Physical | Nausea, fever, diarrhea, dizziness |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Infectious Diseases and Tuberculosis · Eosinophilic Disorders and Syndromes
Introduction
Necrotizing fasciitis (NF) is a rapidly progressing bacterial infection that destroys superficial fascia, subcutaneous tissue, and deep tissue. Bacterial entry typically occurs through a skin laceration, resulting in local pain, fever, systemic toxicity, tissue damage, and potentially fatal outcomes if not diagnosed and treated promptly [1]. As the infection advances, the skin may change from red and purple discoloration to patches of blue-gray. Eventually, the skin can break down into bullae, and cutaneous gangrene may develop. Tissue damage and systemic toxicity are caused by the release of cytokines and bacterial toxins, which trigger severe physiological responses [2].
Although the progression of NF is well documented, definitive diagnosis is achieved only through surgical debridement. Studies indicate that 70-85% of patients with NF are initially misdiagnosed due to symptoms that resemble those of other soft-tissue infections [3,4]. The clinical presentation, evaluation, and management of this patient are analyzed to demonstrate how NF can mimic other soft-tissue infections and to emphasize the importance of including it in the differential diagnosis. Despite advances in diagnostic imaging and laboratory testing, NF is frequently misdiagnosed in its early stages. This case illustrates key diagnostic pitfalls and highlights clinical features that should prompt early reconsideration of an initial diagnosis of cellulitis.
Case presentation
A 33-year-old white male with a history of intravenous drug use, recent incarceration, and extensive upper extremity tattooing presented with progressive swelling, erythema, and pain of the left forearm. Initial examination demonstrated localized erythema and purulent drainage, consistent with cellulitis, and was treated with oral Bactrim by the jail nurse for 24 hours. Despite antibiotic management, the patient developed a temperature of 100.9°F with worsening symptoms and was transferred to the emergency department for further evaluation and management. Physical examination demonstrated an indurated and erythematous left forearm and a 1.5-cm opening on the distal forearm exuding foul-smelling discharge, as in Figure 1.
Clinical appearance of the left forearm lesion at presentationClose-up views of the left forearm demonstrate an open necrotic wound with surrounding erythema and soft-tissue destruction overlying a tattooed area.Written informed consent was obtained from the patient to publish identifying information.
Range of motion in the left hand was limited, with increased temperature and fluctuating tenderness from the left cubital fossa to the hand. Initial laboratory evaluation revealed leukocytosis with neutrophilia, mild renal dysfunction, normal blood glucose (suggesting that hyperglycemia was not a contributing factor in this case), and hypocalcemia, consistent with a severe inflammatory process, as seen in Table 1.
At this stage, the working diagnosis was cellulitis with abscess formation. Intravenous vancomycin (15 mg/kg every 12 hours) and Zosyn (3.375 g every six hours) were initiated to provide broad-spectrum antimicrobial coverage, and intravenous fluids were administered to address hemodynamic instability. Ibuprofen was given for analgesia. The patient initially responded favorably to treatment, with no reports of fever or severe pain.
Twelve hours after admission, the patient experienced worsening induration despite an improved white blood cell count of 9.7 and reported pain disproportionate to the clinical findings. The severity of the pain relative to the physical findings raised concern about a deeper soft-tissue infection. Plain radiography of the left forearm demonstrated extensive soft tissue swelling with subcutaneous emphysema, a finding highly suggestive of NF in the appropriate clinical context (Figure 2).
Plain radiographs of the left forearmRadiographs demonstrating subcutaneous emphysema (arrow), a key radiographic clue supporting necrotizing fasciitis.
These factors, along with preliminary wound cultures positive for gram-positive cocci, gram-positive bacilli, and gram-negative bacilli, raised a high index of suspicion for NF Type I infection. The patient was taken emergently to the operating room, where surgical exploration confirmed NF by frozen section (Figure 3).
Histopathological findings from surgical debridementHistopathological features of NF. Hematoxylin and eosin stain sections showing necrotic skeletal muscle fibers and infiltration by dense, acute inflammatory infiltrate (original magnification ×10, 20).NF, necrotizing fasciitis
Final wound cultures were positive for Streptococcus species, Peptostreptococcus, and Prevotella intermedia. Following infectious disease consultation, Zosyn was discontinued, and vancomycin (15 mg/kg every 12 h IV) and Unasyn (3 g every six hours IV) were continued. Due to the patient's history of substance use disorder, patient-controlled analgesia with Dilaudid was used for pain management. The patient was gradually weaned and transitioned to oral Norco with adjunct gabapentin.
Extensive debridement was performed, followed by multiple subsequent surgical interventions. After the procedure, a wound vacuum-assisted closure device was applied, and the patient was transferred to the intensive care unit, where hemodynamic status improved. Serial debridement and irrigation were performed on days 1, 3, 5, and 8, with additional debridement, irrigation, and Integra placement on day 11. By day 15, the infection had resolved, and the patient's wound was closed via split-thickness skin grafting reconstruction. Ultimately, broad-spectrum antibiotic therapy, debridement, and reconstruction led to a favorable clinical outcome, and the patient subsequently returned to the correctional facility with a good functional recovery (Figure 4).
Forearm after debridementForearm after debridement on day five (left) and day 15 (right).
A structured timeline of the patient’s clinical course, including symptom progression, diagnostic evaluation, and therapeutic interventions, is summarized in Table 2.
Discussion
NF is a rapidly progressing bacterial infection that targets the subdermal fascial planes, leading to destruction of superficial fascia, subcutaneous tissue, and deep tissue. The annual incidence in the USA is between 500 and 1,500 cases reported, with mortality rates for cases receiving treatment ranging from 6% to 76%, but nearing 100% for cases without treatment [5]. Literature suggests that surgical intervention beyond 24 hours from diagnosis is directly correlated to increased mortality, and failure to diagnose promptly can result in death [6].
NF is classified into two types. Type I is polymicrobial, caused by a combination of gram-negative and anaerobic bacteria, whereas Type II is monomicrobial and typically results from a single pathogen, such as group A Staphylococcus aureus or Streptococcus, in single-site infections. Type I is generally associated with enteric pathogens and occurs in patients with diabetes, peripheral vascular disease, recent surgery, or immunocompromised states. Type II infections are due to skin flora and can affect otherwise healthy individuals of any age. In both types, the infection initially travels along the fascial plane, sparing surrounding tissues and making early diagnosis challenging. As the infection progresses, it rapidly spreads to the fascia and perifascial planes, resulting in secondary infection of the skin, soft tissues, and muscles [7].
Clinical manifestations of NF may be acute or sub-acute. Affected areas are typically erythematous, swollen, warm, shiny, and excessively tender. Patients often experience pain that is disproportionate to clinical findings, and the skin may progress from red and purple discoloration to patches of blue and gray. As the disease advances, bullae develop, and ultimately, frank cutaneous gangrene occurs [8].
Several factors contributed to the delayed recognition of NF in this case. The patient’s NF was initially misdiagnosed as cellulitis, likely due to the presence of an open wound on the left distal forearm and the erythematous, indurated appearance, which are consistent with cellulitis, especially in the context of intravenous heroin use. Extensive tattooing obscured early cutaneous changes, while transient initial improvement with antibiotics provided false reassurance. While both cellulitis and NF can cause necrosis, cellulitis is confined to the skin, whereas NF extends into deeper tissues [9]. Although cellulitis is more common, NF must be considered when pain is disproportionate to physical findings or when clinical progression is rapid. Table 3 outlines key distinctions between these two conditions.
This case underscores the importance of thorough clinical examination. As most cases are initially misdiagnosed, clinicians should include NF in the differential diagnosis when patients present with signs of acute or sub-acute infections such as cellulitis, abscess, necrotizing myositis, gas gangrene, deep venous thrombosis, septic arthritis, warfarin-induced skin necrosis, brown recluse spider bite, and gangrene with secondary infection. Because many of these conditions are soft-tissue infections, clinicians should maintain a high index of suspicion for NF in similar presentations. When clinical suspicion is high, prompt biopsy is necessary to confirm the diagnosis and facilitate timely debridement, thereby reducing morbidity and mortality.
Diagnosis of NF relies on clinical and laboratory findings that prompt surgical exploration, with tissue biopsy serving as the definitive diagnostic test. Imaging modalities such as X-rays, ultrasound, CT, and MRI can assist in revealing asymmetrical fascial thickening, soft-tissue air, blurring of fascial planes, inflammatory fat stranding, reactive lymphadenopathy, and nonenhancement of muscular fascia with biopsy findings revealing extensive tissue destruction, vascular thrombosis, and infiltration of fascial planes with inflammatory cells and bacteria [9,10]. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score differentiates NF from other soft-tissue infections using CRP, WBC, hemoglobin, sodium, creatinine, and glucose levels; however, waiting for laboratory results may not be feasible in acute settings [11].
Wei et al. (2023) discussed in detail the diagnostic modalities used for NF evaluation and management [12], as shown in Table 4.
Despite advancements in imaging modalities, clinical diagnosis remains essential for the timely identification of NF. While scoring systems and imaging can support clinical judgment, definitive diagnosis requires surgical exploration. Early multidisciplinary involvement and prompt operative management are critical to improving outcomes. As intraoperative biopsy is the only definitive diagnostic modality, clinicians should not delay intervention in favor of imaging or other diagnostic methods. This highlights the importance of clinical acumen in promptly recognizing symptoms suggestive of NF, even when diagnostic methods are inconclusive. Yu et al. describe clinical modalities for initial evaluation of NF based on clinical signs and symptoms, as shown in Table 5 [13].
Management of NF requires aggressive surgical debridement of all necrotic tissue. Early operative intervention within 12 hours remains the cornerstone of improved survival in NF [6]. Debridement should be performed daily or at regular intervals until healthy, viable, bleeding tissue is observed. Empiric broad-spectrum antibiotics are initiated and subsequently tailored to target specific bacterial organisms once cultures are available [14]. In severe cases involving gas-forming organisms, intravenous immunoglobulin (IVIG) therapy may be considered [15].
Conclusions
NF is a life-threatening condition that can initially resemble cellulitis, leading to diagnostic delays, particularly when tattoos or skin alterations obscure early clinical signs. Prompt surgical consultation upon suspicion of NF is essential to facilitate timely debridement and reduce morbidity and mortality. This case highlights the significance of recognizing disproportionate pain as an early warning sign, monitoring for rapid clinical progression, and identifying imaging features such as subcutaneous emphysema on plain radiography that suggest deep soft-tissue infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Consensus on the diagnosis and treatment of adult necrotizing fasciitis (2025 edition)Burns Trauma Zhou L Li H Luo G 013202510.1093/burnst/tkaf 031PMC 1222567440612051 · doi ↗ · pubmed ↗
- 2Polymicrobial necrotizing fasciitis - a fatal outcome following a motor vehicle accident Indian J Forensic Med Toxicol Chaudhari VA Pan AK 164169172023
- 3Necrotizing fasciitis: treatment concepts & clinical outcomes - an institutional experience BMC Surg Raveendranadh A Prasad SS Viswanath V 3362420243946853610.1186/s 12893-024-02638-2PMC 11514789 · doi ↗ · pubmed ↗
- 4A case of necrotizing fasciitis initially misdiagnosed as cellulitis Int J Surg Case Rep Joshi A Alomar T Kaune DF Bourgeois J Solomon D 10970111820243866980210.1016/j.ijscr.2024.109701 PMC 11064608 · doi ↗ · pubmed ↗
- 5Necrotizing fasciitis of the upper extremity - a review Orthop Rev (Pavia) Ditsios K Chitas K Christidis P Charatsis K Katsimentzas T Papadopoulos P 353201420223603472410.52965/001c.35320 PMC 9404292 · doi ↗ · pubmed ↗
- 6Practical review of necrotizing fasciitis: principles and evidence-based management Plast Reconstr Surg Glob Open Guliyeva G Huayllani MT Sharma NT Janis JE 012202410.1097/GOX.0000000000005533 PMC 1079870338250213 · doi ↗ · pubmed ↗
- 7Current concepts in the management of necrotizing fasciitis Front Surg Misiakos EP Bagias G Patapis P Sotiropoulos D Kanavidis P Machairas A 36120142559396010.3389/fsurg.2014.00036 PMC 4286984 · doi ↗ · pubmed ↗
- 8Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America Clin Infect Dis Stevens DL Bisno AL Chambers HF 1471595920142494753010.1093/cid/ciu 296 · doi ↗ · pubmed ↗