Small but mighty: Rhabdomyoblastic melanoma
Surya A. Veerabagu, Kimberly Artounian, Shelly Stepenaskie, Brian Hinds, Andrew Matsumoto

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1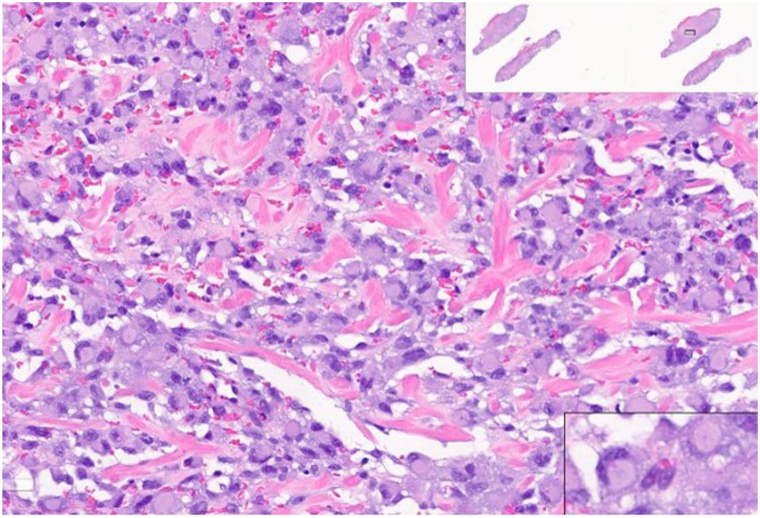 Figure 2
Figure 2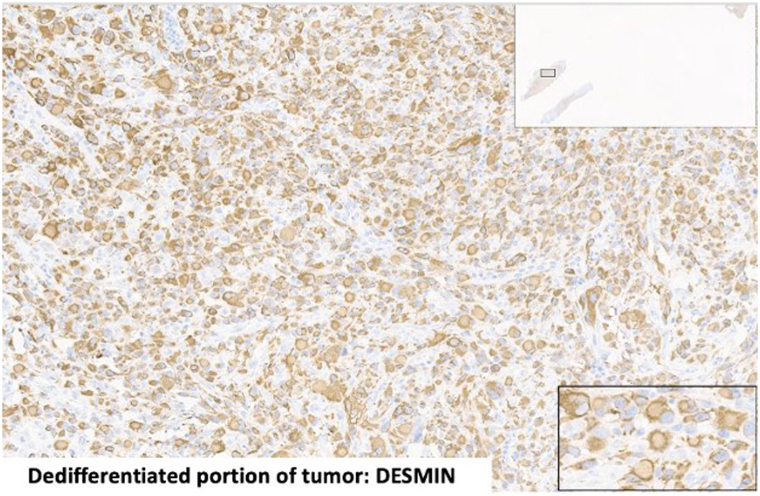 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management · Sarcoma Diagnosis and Treatment · CNS Lymphoma Diagnosis and Treatment
Introduction
Rarely, melanoma cells can lose their melanocytic phenotype while simultaneously acquiring nonmelanocytic phenotypes, a process termed transdifferentiation.1 It can occur in response to targeted immunotherapy, posing a serious threat to treatment.2 It can also occur in the absence of immunotherapy. In both instances, transdifferentiated melanomas are significantly more aggressive than conventional melanoma. Because of the rarity of this phenomenon, no formal treatment guidelines have been established. In this case, melanoma tumor cells transdifferentiated into rhabdomyoblasts, which are early–stage mesenchymal precursors of skeletal muscle cells.
Case report
An 82-year-old male patient with a history of multiple nonmelanoma skin cancers presented for Mohs consultation for his left superior helix biopsy–proven superficial spreading subtype melanoma in situ with associated dermal pleomorphic malignant melanoma with rhabdomyoblastic features. The initial biopsy was performed by an outside dermatologist, who referred the patient to our medical center. The 2.1 mm-Breslow depth placed the pathologic stage of the tumor at T2b.
Upon our examination, on the left superior helix was a 1.2 cm ulcerated dark brown papule (Fig 1). Physical examination was negative for cervical, parotid, and axillary lymphadenopathy. Positron emission tomography-computed tomography scan was negative for metastatic disease.Fig 1. Rhabdomyoblastic melanoma of the ear helix.
Our team performed a confirmatory biopsy. Routine slide evaluation demonstrated a classic superficial spreading subtype melanoma in situ (positive for Sox-10, S100, and PRAME) with an invasive tumor component showing multiple atypical, pleomorphic polygonal tumor cells in the dermis. These atypical, polygonal tumor cells resided within the dermis, without a junctional component (Fig 2). Dermal tumor cells were positive for immunostains Ki-67, PRAME, desmin, myogenin, myoD1, and negative for other melanocytic markers (Sox-10, Melan-A, HMB-45, MiTF, and S100), confirming the diagnosis of an ulcerated, transdifferentiated melanoma with associated rhabdomyosarcomatous phenotype (Fig 3). The malignant dermal cells were negative for common melanoma mutation BRAF V600E. Given the aggressive tumor subtype and Breslow thickness, the patient underwent partial auriculectomy (wide local excision) with sentinel lymph node biopsy performed by head and neck surgery. Lymph node biopsies were negative for tumor. Both the melanoma in situ and invasive transdifferentiated component were excised with clear margins.Fig 2. Atypical polygonal cells with prominent cytoplasm and eccentric nucleus.Fig 3. Dedifferentiated tumor portion that was positive for desmin.
After the surgery site healed, the patient successfully completed adjuvant radiation therapy 2 months after surgical excision and is currently undergoing adjuvant pembrolizumab immunotherapy for 1 year. The patient is being closely followed with regular skin checks and regular imaging for monitoring of recurrence or metastatic disease. As of 9 months after surgery, he remains without clinical evidence of recurrence.
Discussion
Primary cutaneous melanoma with rhabdomyoblastic transdifferentiation is incredibly rare, with only 10 cases confirmed with immunohistochemical evaluation demonstrating loss of melanocytic markers and positivity of both desmin and myogenin.3^,^4 Patient ages ranged from 41 to 96 with a 7:2 male-to-female ratio. Melanoma subtypes included undisclosed (4/10), superficial spreading (2/10), desmoplastic melanoma (2/10), lentigo maligna melanoma (1/10), and nodular melanoma (1/10) with Breslow depths ranging from 4.1 to 80 mm.3 Only 1 of the 10 cases did not include patient outcome information.5
The majority (6/10) of cases in the literature were diagnosed with tumor metastases concurrently present. In some cases, patients initially presented to the hospital due to the symptoms from their metastases rather than from the tumors themselves, despite large (>5 cm) clinical sizes.6 Of these 6 cases, 6 patients died; however, 1 death was unrelated to cutaneous disease. Three of the 4 melanoma-related deaths occurred, while patients were undergoing various adjuvant therapies, including chemotherapy (dacarbazine), anti-PD1 immunotherapy, and radiotherapy. All 4 patients were male ranging in age from 41 to 76. Notably, patients’ melanoma Breslow depths (4.1-9 mm) were smaller in comparison to other reported cases (4.1-80 mm). Two of the living patients with known metastases were undergoing adjuvant chemotherapy (unnamed agents).
Of the 9 immunohistochemically confirmed cases of primary cutaneous melanoma with rhabdomyosarcomatous transdifferentiation, only 3 cases did not present with metastases, similar to our case.6^,^7 Two reports only mentioned tumor excision, and it is assumed that neither patient underwent adjuvant therapy. Both cases involved patients in their 80s with facial desmoplastic melanomas (temple and chin) with 18.0 and 80 mm Breslow depths. The third case presented with an associated lentigo maligna melanoma with a Breslow depth of 4.1. However, within 3 months, the tumor recurred twice after excision. After the third excision, the patient underwent adjuvant radiation therapy and remained disease free. All studies, including our own, followed patients for at least 6 months after the original diagnosis.6^,^7
When reviewing the data, primary cutaneous melanoma with rhabdomyosarcomatous transdifferentiation appears to oppose standard melanoma trends, when reviewing the data-patients with more aggressive melanoma subtypes, such as desmoplastic and lentigo melanoma with larger Breslow depths (18-80 mm), appeared to positively respond to therapy, whereas those with smaller Breslow depths (4.1-9.0 mm) responded poorly. The Breslow depth of these cases ranges from double to 40 times the Breslow depth of our case (2.1 mm).3 Furthermore, for most cases, the rhabdomyoblastic de-differentiation was only identified retrospectively after recurrence or nodal metastasis, not at primary presentation like ours.1 Whether these are trends or coincidences, these cases emphasize the unpredictability and high mortality of this disease.
Interestingly, rhabdomyoblastic transdifferentiation in primary melanoma cases tends to generally occur later (mean, 70 years old; range, 41-96 years old) and in male patients (4:1 male-to-female ratio) in comparison to rhabdomyoblastic transdifferentiation cases in nodal/distant melanoma metastases. In those cases, patients were significantly younger (mean, 40 years old; range, 21-59) with a female predominance (5:2).4^,^8
This case not only adds to the literature of this rare diagnosis but also draws attention to the aggressive nature of this tumor subtype that can be mitigated with early, prompt multidisciplinary care. This case also highlights the importance of incorporating extensive, specific dermatopathologic review for consensus pathologic confirmation of these rare diagnoses.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tran T.A.N.Linos K.de Abreu F.B.Carlson J.A.Undifferentiated sarcoma as intermediate step in the progression of malignant melanoma to rhabdomyosarcoma: histologic, immunohistochemical, and molecular studies of a new case of malignant melanoma with rhabdomyosarcomatous differentiation Am J Dermatopathol 413201922122910.1097/dad.000000000000123630085960 · doi ↗ · pubmed ↗
- 2Mehta A.Kim Y.J.Robert L.Immunotherapy resistance by inflammation-induced dedifferentiation Cancer Discov 88201893594310.1158/2159-8290.Cd-17-117829899062 PMC 6076867 · doi ↗ · pubmed ↗
- 3Iliesiu A.Nimigean V.Tapoi D.A.Costache M.Primary cutaneous rhabdomyosarcomatous melanomas-a report of two cases and literature review Diagnostics (Basel)15112025135710.3390/diagnostics 1511135740506928 PMC 12155165 · doi ↗ · pubmed ↗
- 4Țăpoi D.A.Gheorghişan-Gălățeanu A.A.Dumitru A.V.Primary undifferentiated/dedifferentiated cutaneous melanomas-a review on histological, immunohistochemical, and molecular features with emphasis on prognosis and treatment Int J Mol Sci 24122023998510.3390/ijms 2412998537373134 PMC 10298704 · doi ↗ · pubmed ↗
- 5Kuwadekar A.Allard J.Dardik M.Smith F.Melanoma with rhabdomyosarcomatous differentiation BMJ Case Rep 20182018 bcr 201822426310.1136/bcr-2018-224263 PMC 601146729880623 · doi ↗ · pubmed ↗
- 6Ferreira I.Droop A.Edwards O.The clinicopathologic spectrum and genomic landscape of de-/trans-differentiated melanoma Mod Pathol 341120212009201910.1038/s 41379-021-00857-z 34155350 · doi ↗ · pubmed ↗
- 7Choy A.Wang A.Thayaparan G.K.The diagnostic utility of PRAME in primary cutaneous dedifferentiated and transdifferentiated melanomas J Cutan Pathol 523Mar 202521221910.1111/cup.1478339748565 · doi ↗ · pubmed ↗
- 8Gupta A.Wagman R.Kuwadekar A.Scoppetuolo M.Dardik M.Smith F.Use of immunotherapy and radiation treatment in the management of metastatic melanoma with rhabdomyosarcomatous differentiation Adv Radiat Oncol 51202013413910.1016/j.adro.2019.07.01932051900 PMC 7004934 · doi ↗ · pubmed ↗