Gut microbiota and sarcoidosis: a concise review
Roberto G. Carbone, Francesco Puppo, Victor F. Tapson

TL;DR
This review explores the possible role of gut and lung microbiota in sarcoidosis, a disease characterized by granulomas, and compares it to other lung diseases.
Contribution
The paper provides a concise review of microbial involvement in sarcoidosis pathogenesis and compares the lung microbiome in sarcoidosis with other interstitial lung diseases.
Findings
The lung microbiome in sarcoidosis differs from healthy individuals, with conflicting results on bacterial and fungal abundance.
Cutibacterium acnes and Mycobacterium tuberculosis are strongly associated with sarcoidosis in a meta-analysis of over 6,000 patients.
Microbial presence in sarcoid granulomas is often detected genomically, with limited bacteriological or proteomic confirmation.
Abstract
Microbial involvement in sarcoidosis pathogenesis is suggested by the observation that histological findings in sarcoid granulomas are like those of leprosy, tuberculosis and parasitic infection. Some studies have shown that the lung microbiome in patients with sarcoidosis is different from healthy individuals. Results are conflicting, reporting an abundance or decrease in bacterial and fungal species. The altered composition of the microbiome in sarcoidosis can contribute to the formation of granulomas, typical lesions of the disease, through interactions with the host immune system. However, no single microbe has been clearly demonstrated as a cause of sarcoidosis, several microorganisms have been involved in the formation of granulomas and are under study. In fact, various microorganisms have been detected in sarcoid granulomas and in the tissue of different organs. Microorganisms…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
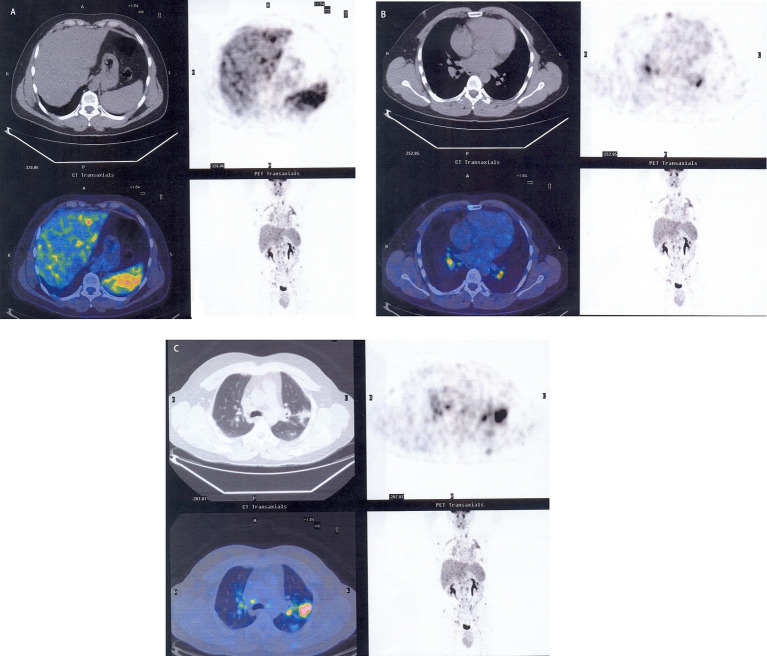 Figure 1
Figure 1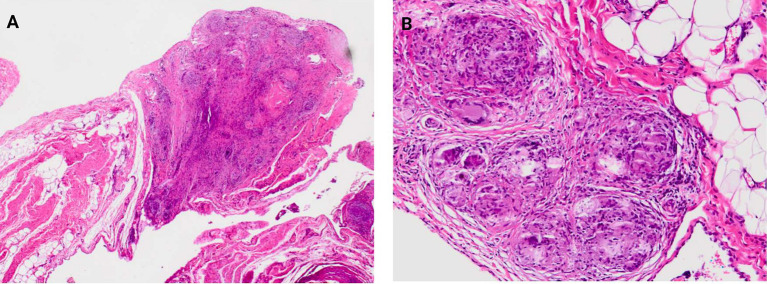 Figure 2
Figure 2| Comparison group | Observation in sarcoidosis group | Observation in other ILD group |
|---|---|---|
| Sarcoidosis vs. ILD | No difference between groups. | No differences in most comparative studies. |
| Sarcoidosis vs. AE-ILD | ⬆ Prevotella, Streptococcus, and Veillonella compared to AE-ILD. | No differences between AE-ILD and IPF |
| Sarcoidosis vs. ILD vs. COPD | ⬇ Proteobacteria and Firmicutes compared to COPD/AE-COPD. | ⬆ Proteobacteria in ILD compared to other groups; Klebsiella and |
| Sarcoidosis vs. healthy controls | ⬇ Bacterial in lower airways; | Not comparable in most studies. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · Gut microbiota and health · Cancer Research and Treatments
Introduction
Sarcoidosis, a disease characterized by noncaseating granulomas formation in various organs, is thought to involve interactions between the host immune system and microbiome, particularly in the lungs, gut, and blood (1–5). However, the exact origin of sarcoidosis is yet unknown.
Several studies report on the possible relationship of sarcoidosis with an autoimmune process while others suggest a possible close familial genetic correlation with sarcoidosis development. Furthermore, additional studies hypothesized that microorganisms such as Cutibacterium acnes and Mycobacterium tuberculosis could be involved in sarcoidosis development. Because of possible infectious mechanisms as a cause of disease, antibiotics have been included in the treatment approach. Current research suggests that changes in microbiota, particularly in the lungs, may play a role in sarcoidosis progression.
Interestingly, some sarcoidosis patients may have an increased risk of lymphoma, developing a condition defined as sarcoidosis-lymphoma syndrome, where sarcoidosis precedes lymphoma (6). Moreover, sarcoidosis or sarcoid-like granulomas have been reported in patients suffering from cancer, especially those treated with immunotherapy, perhaps related to excessive immune response against cancer cells (7–10).
The link between sarcoidosis and microbiome is supported by the hypothesis that changes in the microbiome community could influence its development especially in the lungs and gut. Research suggests a potential role for microbial dysbiosis (an imbalance in the microbiome) in immune dysregulation that drives sarcoidosis, possibly through the gut-lung axis where gut microbiota influence lung health. Specific microbial shifts have been observed in the airways and blood of sarcoidosis patients and some microorganisms like Cutibacterium acnes and Mycobacterium tuberculosis have been implicated.
The aims of the review are: (1) to clarify the role of microbial involvement in sarcoidosis pathogenesis, (2) to describe microbiota in lungs with sarcoidosis and to compare the data with other interstitial lung diseases.
History of lung microbiome
The history of the lung microbiome began with the outdated belief that the lungs were sterile; a view disproven by new sequencing technologies in the 2010s. Early studies identified a bacterial community in the lower respiratory tract and subsequently linked the lung microbiome to diseases such as chronic obstructive pulmonary disease (COPD), cystic fibrosis, and pneumonia. This emerging topic is now exploring the roles of the entire microbiome including its interaction with the immune system and its connection to conditions such as lung cancer and COVID-19 infection.
The history can be divided into three sections: pre-2010, 2010–2019 and post −2019 to present. Around 2010, the sterile lung theory was dispelled based on the discovery of several bacteria in the lower respiratory airways even in healthy subjects. Thereafter, mycobiome (fungi) and viruses were included. During the 2014–2016 period the relationship between lung microbiome and pulmonary diseases began to be uncovered with studies regarding COPD, cystic fibrosis, pneumonia, and interstitial lung disease (ILD). The early study of lung sarcoidosis, a form of ILD associated with microbiome, has been reported by Garzoni et al. in 2013 (11). At that point, the role of the lung microbiome was linked to immune responses and this became a major focus. From the end of 2019 to the present, research has found significant connections between the lung microbiome, lung cancer, and COVID-19 infection (12).
Sarcoidosis and microbiome
Many years ago, Du Bois et al. (13) proposed the possible microbial involvement in sarcoidosis pathogenesis based on the finding of numerous microorganisms in sarcoid granulomas. Interest in the gut microbiome’s role in sarcoidosis has grown in recent years, whereas the role of the pulmonary microbiome is largely unknown (14). Changes in the microbiome, particularly in the lungs, are believed to result in an immune response probably exacerbating the state of the disease in combination with pulmonary fungal and bacterial infections. A low number of antimicrobial peptides in the lung could lead to dysbiosis representing a pathogenic trigger for sarcoidosis development (14).
Many microorganisms have been identified at the genomic level, whereas only a few studies have demonstrated the presence of microbes using bacteriological or proteomic procedures. Notably, using monoclonal antibodies, Cutibacterium acnes was present in 63% of granulomas in cardiac sarcoidosis. These microorganisms introduce foreign substances, inducing an immune response. Moreover, mycobacteria produce mycobacterial heat shock proteins, superoxide dismutase A, and mycobacteria catalase-peroxidase and may be responsible for granuloma formation.
Lung sarcoidosis is associated with microbial dysbiosis, meaning an imbalance of bacteria and fungi in the lungs, which is linked to lower levels of antimicrobial peptides (AMPs) and an increase in microbes such as Aspergillus. Lower AMPs in sarcoidosis demonstrate an interaction between microbiota and immune system. The pathogenic role played by dysbiosis in sarcoidosis development needs to be confirmed by large experimental studies (14).
Candida and Aspergillus are the most common fungi detected in sarcoidosis, as confirmed by an increased level of antifungal antibodies in bronchoalveolar lavage (BAL) fluid and serum, suggesting that fungal infections may represent possible sarcoidosis etiologic agents (15).
Dysbiosis is an emerging area of research, and it is still being investigated whereas it is a cause or a consequence of sarcoidosis. Microbial/fungal imbalance may play a pathogenic role and could potentially be a target for future treatments. A higher abundance of Aspergillus has been observed in the lower airways of sarcoidosis patients. Additionally, increased levels of Atopobium and Fusobacterium were identified in sarcoidosis samples. Some research suggests that several fungal components, like those from Aspergillus nidulans, may trigger an immune response (CD + T cell activation) in sarcoidosis patients (16, 17).
Gut and lung axis
The link between sarcoidosis and microbiome is supported by the hypothesis that changes in microbiome community could influence sarcoidosis development, especially in the lungs and gut. Research suggests a potential role for gut dysbiosis in the immune dysregulation that drives sarcoidosis, possibly through the gut-lung axis where gut microbiota may influence lung health. This concept implies that the gut microbiome communicates with the lungs. An unhealthy gut microbiome may trigger an exaggerated immune and inflammatory response in the lungs leading to sarcoidosis development. Therefore, changes in gut microbiome composition and function have been linked to inflammatory processes and granuloma formation in sarcoidosis (18).
Specific microbial shifts have been observed in the airways and blood of sarcoidosis patients and some microorganisms like Cutibacterium acnes and Mycobacterium tuberculosis have been implicated. Different bacterial and fungal components have been detected in the lower airways of sarcoidosis patients compared to healthy individuals, indicating a potential microbial imbalance. Furthermore, specific microbial genera have been identified that are more or less abundant in the blood of sarcoidosis patients and suggested that this finding could be a potential biomarker for the disease.
Pathways in amino acid and energy metabolism, redox process, and iron transport are significantly underrepresented in sarcoidosis patients. This suggests that microbial metabolites such as short-chain fatty acids which normally have immunomodulatory properties, may be altered and contribute to inflammation. Microbial antigens or their components can circulate through blood from the gut to other organs where they may trigger T-helper1 (Th1) and Th17 immune responses characteristic of granuloma formation (19). Specifically, activation and secretion of pro-inflammatory cytokines (IL-6, IL-12, IL-18, and TNF-alfa) contribute to alterations in gut microbiota and promote sarcoid granuloma production in various organs (19). Moreover, microbes are a source of ligands whose interplay with pattern recognition receptors of innate immunity cells may contribute to granulomatous inflammation (20).
Sarcoidosis is usually diagnosed through a positron emission tomography/computed tomography (PET/CT) scan to exclude disease-affected lung and extrapulmonary sites. A definitive diagnosis of sarcoidosis is made through histology (Figures 1A–C, 2A,B) (21). Interestingly, increased levels of Cereibacter sphaeroides which are capable of heme synthesis, correlate with heme-related inflammation, a process potentially responsible for granuloma formation.
The figures highlight the sites affected by sarcoidosis through PET/CT scan: liver and spleen (A), bilateral hilar lymph nodes (B), subpleural area of the left upper lobe (C).
The figures highlight the omentum (A) with granulomas, H&E magnification X40 and at higher magnification sarcoidosis granulomas (B) in the same location, H&E magnification X100.
Finally, altered microbiome composition can affect gut integrity, potentially leading to increased intestinal permeability which allows microbes and their products to enter the systemic circulation.
Genetics
Sarcoidosis development is closely influenced by genetic factors which interact with the microbiome. This includes: (i) genetic predisposition, (ii) key genes, (iii) and gene-microbiome interaction. The premise of genetic susceptibility is supported by familial clustering and a higher incidence of sarcoidosis within specific ethnic groups. Additionally, some genetic loci have been identified within human leukocyte antigens (HLA) region, as HLA -DRB1, HLA-B, and BTNL2 that are linked with sarcoidosis development. Moreover, variants of other non-HLA genes, like ANXA11 and XAF1, may increase granuloma duration (22).
Interestingly, specific HLA alleles associated with sarcoidosis, like HLA-DRB 103, have been linked to T cell responses to certain fungal antigens such as Aspergillus nidulans. Certain genes associated with sarcoidosis risk such as SLC11A1 are also involved in susceptibility to certain bacterial infections (i.e., Mycobacterium species) suggesting a complex gene-microbe interaction. Genomic studies are currently underway (e.g., the GRADS study) to integrate microbiome and genomic data from patients to better understand disease mechanisms and identify potential biomarkers or treatments. Current research highlights sarcoidosis as a complex disorder where the genetic background of the host interacts with environmental triggers, specific microbial antigens and gut dysbiosis, that drive chronic, dysregulated immune response and granuloma production (21).
Proteomics
Prior research indicates a significant relationship between microbiome and proteomics suggesting that dysbiosis influences a host’s immune response and protein expression contributing to sarcoidosis development and progression.
Proteomics helps identify proteins that can serve as biomarkers for sarcoidosis, including zinc finger protein 688 and mitochondrial ribosomal protein L43 which is especially linked to severe disease. Studies on alveolar macrophages found that protein alterations are related to key cellular functions such as Fcy-mediated phagocytosis and clathrin-mediated endocytosis.
Proteomics data when combined with other omics data, such as transcriptomics, helps identify biological pathways involved in sarcoidosis such as those related to neuro-inflammation and integrin signaling. Identifying these protein alterations provides insights into disease pathogenesis and can lead to the discovery of new therapeutic targets.
Therefore, there is evidence of a connection between microbiome composition, the host’s immune response to microbial proteins and sarcoidosis development (14).
Microbiome and interstitial lung disease
Microbiome imbalance or dysbiosis in gut microbiome is associated with ILD (23). Notably, lung microbiome impacts ILD progression and studies have shown a role for lung dysbiosis in the pathogenesis of some ILD such as idiopathic pulmonary fibrosis (IPF) and sarcoidosis. As previously described, this correlation is largely explained by gut-lung axis, a bidirectional communication pathway between the gut and the immune system of distal organs like the lungs. Sarcoidosis patients exhibit significant differences in their gut’s microbiome composition compared to healthy individuals (different beta diversity). In sarcoidosis patients, the proportion of the phyla Actinobacteria and Firmicutes are expanded. Specific species such as Cereibacter sphaeroides are significantly more abundant. Other genera as Veillonella, Prevotella, Cutibacterium, and Streptococcus have been found to be enriched in studies of sarcoidosis patients. In healthy controls, the proportion of Bacteroides and Verrucomicrobia are lower. Functional pathways of gut microbiome are also changed (12). When comparing sarcoidosis with ILD, the abundance of Haemophilus, Stenotrhophomonas and Enterobacter is higher in ILD while the abundance of Cutibacterium and Neisseria is higher in sarcoidosis (24).
The microbiota difference between sarcoidosis and other ILD are reported in Table 1. Moreover, 16S RNA gene studies of the lung microbiome in sarcoidosis patients did not show the same changes that have been reported in other ILD (25).
Therapeutic implications
The strong association between gut and sarcoidosis suggests that gut microbiome may offer potential innovative therapeutic strategies for sarcoidosis. These potential approaches include: (1) probiotic supplementation, (2) dietary changes, (3) antimicrobial use, (4) fecal microbiota transplantation (FMT).
Probiotic supplementation allows the restoration of gastrointestinal health. Dietary changes influence microbial composition. Antimicrobial use is still under investigation. FMT shows encouraging results in other conditions, which may also be explored in future research. More research is needed to validate the effectiveness of these innovative therapies in sarcoidosis treatment (26).
Antibiotics are primarily experimental or used for their immunomodulatory properties, rather than to treat active infections, in sarcoidosis treatment. Standard treatment typically relies on corticosteroids like prednisone to reduce inflammation.
In this context, a study reported that 63% of granulomas in cardiac sarcoidosis patients tested positive for Propionibacterium acnes. Of interest, bacteria were also found in 63% of high-grade inflammatory lesions, suggesting they may act as a trigger for the disease’s characteristic immune response (27). Although not standard care, some studies explored the efficacy of antibiotic regimens in sarcoidosis. An exploratory trial showed that 63.2% of participants saw clinical improvements in King’s Sarcoidosis Questionnaire (KSQ) lung scores after azithromycin treatment for chronic cough (27). Moreover, the CLEAR Regimen, a combination of levofloxacin, ethambutol, azithromycin, and rifampin, has shown potential improvement of lung function and skin lesions in some clinical trials (28). Lastly, low-dose minocycline or doxycycline have been used to induce remission in cutaneous sarcoidosis (29). Therefore, antibiotics remain an experimental treatment for sarcoidosis.
Discussion
Little is currently known about the correlation between the microbiome and sarcoidosis. There is a growing area of research that utilizes modern techniques including genetic analysis and proteomics aimed at the evaluation of possible linkages between gut and lung dysbiosis and sarcoidosis development.
For decades, scientists suspected that sarcoidosis was caused by an infectious agent, but no single pathogen was consistently identified. Recently, gut and blood microbiomes have been explored to see how they are related to sarcoidosis. These studies suggest that sarcoidosis and granuloma formation are likely determined by a combination of genetic predisposition with environmental triggers including active immune response to an unknown microbial trigger or a dysregulated microbiome.
However, the sarcoidosis microbiome compared to the microbiomes in other ILD has not been consistent across studies (23, 26).
The exact cause of sarcoidosis remains unknown, the microbiome is considered a significant contributing factor, and ongoing research is focused on dissecting the mechanism by which microbial imbalances drive the disease’s immune pathology. In addition, most studies conclude that there is no unique microbial signature that clearly distinguishes sarcoidosis from other ILD in stable condition. The pulmonary microbiota in both conditions appears to be similar, often dominated by bacteria commonly found in the oral/upper respiratory tract. Differences are more apparent when comparing either disease group to healthy controls (for example, lower diversity in the presence of disease) or when comparing stable disease to acute ILD exacerbation (21, 26, 30, 31).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baughman RP Lower EE Engel P. "Sarcoidosis" In: Baughman RP Carbone RG Bottino G, editors. Pulmonary arterial hypertension and interstitial lung diseases. NY, USA: Humana Press (2009). 213–42.
- 2Carbone RG Puppo F. "Microbiome and interstitial lung disease" In: Carbone RG Puppo F Wille K Shah P, editors. Interstitial lung disease from diagnosis to treatment. NY, USA: NOVA Publisher (2022). 113–9.
- 3Baughman RP Culver DA Judson MA. A concise review of pulmonary sarcoidosis. Am J Respir Crit Care Med. (2011) 183:573–81. doi: 10.1164/rccm.201006-0865 CI 21037016 PMC 3081278 · doi ↗ · pubmed ↗
- 4Baughman RP Valeyre D Korsten P Mathioudakis AG Wuyts WA Wells A. ERS clinical practice guidelines on treatment of sarcoidosis. Eur Respir J. (2021) 58:2004079. doi: 10.1183/13993003.04079-2020, 34140301 · doi ↗ · pubmed ↗
- 5Carbone RG Conway F Shah P. "A clinical approach to interstitial lung disease diagnosis" In: Carbone RG Puppo F Wille K Shah P, editors. Interstitial lung disease from diagnosis to treatment. NY, USA: NOVA Publisher (2022). 121–44.
- 6London J Grados A FerméC Charmillon A Maurier F Deau B . Sarcoidosis occurring after lymphoma: report of 14 patients and review of the literature. Medicine (Baltimore). (2014) 93:e 121. doi: 10.1097/MD.000000000000012125380084 PMC 4616278 · doi ↗ · pubmed ↗
- 7Dimitriou F Frauchiger AL Urosevic-Maiwald M Naegeli MC Goldinger SM Barysch M . Sarcoid-like reactions in patients receiving modern melanoma treatment. Melanoma Res. (2018) 28:230–6. doi: 10.1097/CMR.000000000000043729485531 PMC 5929490 · doi ↗ · pubmed ↗
- 8Fakhri G Akel R Salem Z Tawil A Tfayli A. Pulmonary sarcoidosis activation following neoadjuvant pembrolizumab plus chemotherapy combination therapy in a patient with non-small cell lung cancer: a case report. Case Rep Oncol. (2017) 10:1070–5. doi: 10.1159/000484596, 29515398 PMC 5836160 · doi ↗ · pubmed ↗