Diagnostic Challenges and Surgical Management of Ovarian Hydatid Cyst: A Case Report From an Endemic Region and Literature Review
Fatemeh Asadi Kohbad, Razieh Akbari, Maryam Forouzin, Fatemeh Nili, Leila Asadi, Marjan Ghaemi

TL;DR
This case report highlights the diagnostic and surgical challenges of ovarian hydatid cysts in an endemic region, emphasizing the importance of accurate diagnosis and treatment.
Contribution
The paper contributes a detailed case report and literature review on the rare condition of ovarian hydatid cysts, emphasizing diagnostic and management strategies in endemic regions.
Findings
Ovarian hydatid cysts can mimic ovarian neoplasms, requiring a high index of suspicion for accurate diagnosis.
Surgical management combined with anthelmintic therapy is effective in treating ovarian hydatid cysts.
Ultrasound and CT imaging, along with histopathological evaluation, are crucial for diagnosis.
Abstract
Ovarian hydatid cysts are an infrequent presentation of the zoonotic condition caused by Echinococcus granulosus tapeworms. These cysts can easily be mistaken for benign or malignant ovarian neoplasms, posing a diagnostic challenge. This case report describes managing a case of ovarian hydatid cyst in an endemic region. A 50‐year‐old woman, who had previously undergone surgery for a liver hydatid cyst, presented with abdominal pain and amenorrhea. Upon further investigations, it was revealed that a multilocular cystic lesion was in her left ovary through ultrasonography and computed tomography. Tumor markers were within normal limits. Intraoperative evaluation confirmed the diagnosis of a hydatid cyst, leading to a decision for a total abdominal hysterectomy with bilateral salpingo‐oophorectomy. The surgery was performed to remove the cyst safely. Following the procedure, the patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
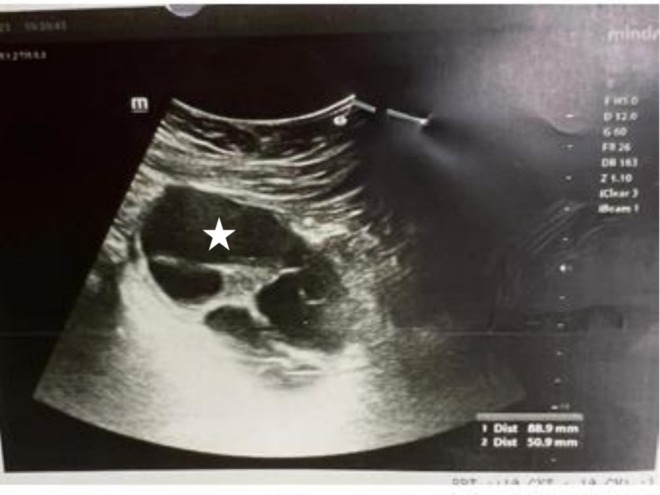 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2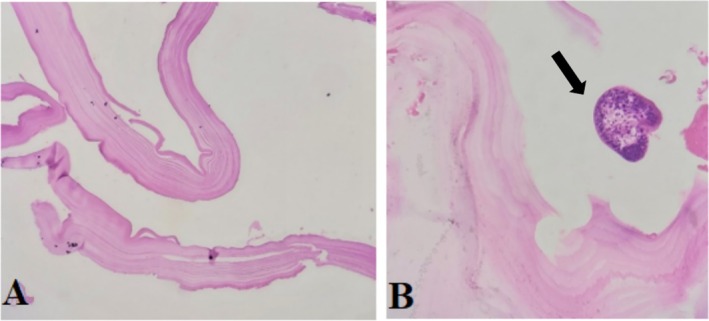 FIGURE 3
FIGURE 3| Author | Year | Diagnosis | Treatment | Follow up |
|---|---|---|---|---|
| L. Cattorini et al. [ | 2011 | Clinical examination revealed pain and abdominal distention, attributed to a large hypogastric incisional hernia. An abdominal CT scan reported: A hepatic hydatid cyst (45 mm × 41 mm) in segment 4 of the liver. A multiloculated cyst (68 mm × 62 mm) is situated in the pouch of Douglas. | The patient underwent surgical intervention, which included the following: Opening the hypogastric hernial sac. Lysis of uterine‐vaginal adhesions. Drainage and marsupialization of the cyst (considered an echinococcal cyst) after prolonged viscerolysis. Hysterectomy due to senile atrophic uterus with calcific fibroma. | Post‐operative care involved ensuring the patient recovered without complications and discharging her on the 11th postoperative day. Anticipated follow‐up might include anti‐helminthic therapy to reduce the chance of recurrence, as well as regular imaging or clinical evaluations to monitor for any signs of cyst recurrence or complications. |
| A.A. Mohammad et al. [ | 2021 | lower abdominal pain and frequent urination. The Pain was poorly localized. Ultrasound revealed a cystic left adnexal lesion measuring 56 mm by 39 mm, unilocular and containing fluid. | laparoscopic surgery included the identification of a hydatid cyst in the left ovary. Injection of chlorhexidine around the cyst, followed by aspiration. Extraction of the hydatid cyst using a retrieval bag. | Postoperative care involved a 2‐day hospital admission. Anthelmintic medications were prescribed for 3 months following the surgery to prevent recurrence. A follow‐up ultrasound was scheduled 6 months post‐surgery, showing normal findings. |
| M.K. Maharlooei et al. [ | 2009 | Abdominal pain in the left lower quadrant, primarily at night. Vaginal spotting for several days each month for the past 3 months. Left adnexal mass on bimanual examination—second‐grade uterine prolapse with cystocele and rectocele. CT scan confirmed a multivesiculated cystic mass with peripheral enhancement, raising suspicion for a malignant process. Preoperative tumor marker CA‐125 was elevated at 50 U/mL. The preoperative diagnosis was an ovarian tumor. | The patient underwent laparotomy, during which multiple cysts resembling hydatid cysts were identified in the left ovary. A total abdominal hysterectomy and left salpingo‐oophorectomy were performed. | Pathological examination confirmed the diagnosis of hydatid cysts with no signs of malignancy. Counter‐current immunoelectrophoresis for the detection of hydatid cysts was strongly positive. Follow‐up would typically include monitoring for recurrence and managing any complications related to the surgery. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic infections in humans and animals · Amoebic Infections and Treatments · Echinoderm biology and ecology
Background
1
Cystic echinococcosis can be a life‐threatening helminthic disease, which Echinococcus granulosus induces. It occurs worldwide but is most common in some parts of Eurasia (especially the Mediterranean region), north and east Africa, Australia, and South America [1]. Mortality of cystic echinococcosis is considerable in endemic areas. Studies report mortality rates ranging from 1.29% to 1.94% [2]. Cysts are almost always hepatic and/or found in the lung, although symptomatic cysts have been observed in several organs with much less incidence including the peritoneum, Spleen, kidney, heart muscle, vascular system (segmental or general); muscular tissue, brain, and bone [3]. The ovary is the most common location for hydatid cysts within the female genital tract, but overall, this occurrence is infrequent (less than 1% of cases). These cysts typically present in a manner that resembles a malignant tumor [4]. In this case, we represent a patient with an ovary hydatid cyst.
Case Presentation
2
A 50‐year‐old woman G2P2, from Karaj in Tehran State, Iran, was hospitalized after experiencing a short instance of abdominal pain in the hypogastric area, particularly in the left lower quadrant (LLQ). The patient said she had been amenorrheic for 8 months and mentioned that she had not had any digestive or urinary issues during this period.
She had surgery for a liver hydatid cyst 3 years ago, but she doesn't remember the specifics. There are no medical records of her previous treatment. Upon admission, the patient was not taking any medication.
Imaging and Diagnosis
3
A sonography was requested (Figure 1), which yielded the following findings:
Ultrasound imaging demonstrating a multilocular cystic lesion in the left ovary, characterized by internal echogenic septa, prompting further evaluation to assess potential underlying conditions.
On the imaging examination, the liver was normal in size and echogenic, with no visible hydatid cysts. The portal and hepatic veins were normal. The gallbladder was not seen in its anatomical location (history of cholecystectomy). The intrahepatic and extrahepatic bile ducts had a normal diameter (CBD: 5 mm, PV: 9 mm). No lymphadenopathy was evident in the para‐aortic areas. The spleen was normal in size and echogenicity. The left ovary showed a multilocular cystic lesion measuring 50 × 89 mm. The right ovary was normal in size and echogenicity. There was no free fluid in the pelvis or abdomen. The bladder wall thickness was normal, with no stones or parietal space‐occupying lesions. The radiologist suggested a consultation with a pathologist for tumor markers. On investigation, the tumor markers were within normal limits, and the Pap smear was negative for intraepithelial lesion or malignancy (NILM). There was no leukocytosis, and the inflammatory tests were negative. Following abdominal and pelvic computed tomography (CT) with intravenous and oral contrast, no pathological findings, except for the previous cholecystectomy, were observed. Given the patient's age and the imaging designated, the presence of an 89‐mm cyst in the ovary, accompanied by constant pain, was observed, and the patient became a candidate for surgery.
Surgery
4
A bilateral salpingo‐oophorectomy (TAH BSO) was performed on the patient considering her age and surgical risks. This approach minimizes the risk of cyst contents spilling, which is critical to prevent infection recurrence. During the procedure, a sterile gauze was used to avoid contamination, and the cysts were carefully removed and sent to the pathologist in a sterile container. During the surgery, daughter cysts and additional evidence consistent with hydatid cysts were identified, supporting the diagnosis. Postoperatively, an infectious disease consultation was requested to assess potential complications that did not reveal any significant findings that would require further intervention. Following the surgical procedure, the patient was discharged with a medical régime that involved albendazole 400 mg administered every 12 h. She was advised to attend follow‐up appointments at the infectious disease clinic as an outpatient to monitor her condition and ensure proper management (Figure 2).
Extracted cysts from the patient with intact membrane.
Pathology Findings
5
The pathology samples were examined using hematoxylin and rosin (H&E) staining, and the results, presented in the following images at 20× magnification (Figure 3).
(A) The microscopic examination reveals a cyst wall structure. The outer acellular laminated membrane is observed, showing a characteristic layered appearance: (B) image illustrates the cyst wall, with protoscolices budding from the wall.
Literature Review
6
In the following section, all similar reports of an ovarian hydatid cyst and the approaches reported are summarized in Table 1.
B. Geramizadeh [7] did a review on unusual hydatid cysts in Iran. In the review, 9 of them were reported as ovarian hydatid cysts, and the preferred method of diagnosis was reported to be ultrasonography, CT scan, and MRI, all of which are much more sensitive than immunologic tests.
Discussion
7
Hydatid disease is an exclusive parasitic condition that is endemic in many parts of the world. This parasitic disease is an important public health concern in Iran, an endemic country [8]. Unilocular cysts caused by Echinococcus granulosus and multilocular cysts caused by E. multilocularis are considered important human diseases due to the negative effect they have on disability‐adjusted life years (DALYs) and economic loss [9]. The clinical manifestations of hydatid cysts in most parts of the body are often too nonspecific to make a diagnosis based only on signs and symptoms before surgical intervention [7]. In a review aimed at assessing the occurrence of hydatid cysts in unusual places endemic to Iran, it was found that according to the literature [7], there have been 9 published cases of ovarian hydatid cysts from Iran.
The initial phase of primary infection is always asymptomatic, with small cysts potentially remaining symptomless for many years or even indefinitely. Symptoms may occur if the cysts rupture or apply pressure, leading to complications like urinary issues or life‐threatening anaphylactic reactions [10]. The nonspecific clinical presentations of the disease make a detailed preoperative diagnosis challenging [1]. Symptomatic examples of the condition may become apparent with characteristic features, but not limited to, abdominal pain, typically localized in the right upper quadrant, jaundice, nausea, vomiting, and abnormalities in liver function tests [11].
The treatment approach for cystic echinococcosis involves the use of anthelmintic drugs both before and after surgery to help decrease the recurrence rate [5]. It is noteworthy that while anthelmintic drugs can be used before surgery in selected cases, the cure rate with medications alone is low, and they are also indicated after surgery to reduce the recurrence rate [5]. Surgical intervention is typically necessary, especially for those at risk of rupture, infected cysts, and those in critical anatomical locations with a significant mass effect. During surgery, it is crucial to avoid leakage to minimize the chances of recurrence [12]. Imaging methods such as radiology, ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) are crucial for final diagnosis [13]. Chemotherapy utilizing benzimidazole compounds such as albendazole and mebendazole represents a common practice, with albendazole demonstrating efficacy in diminishing cyst size and quantity. Although adverse reactions like nausea, hepatotoxicity, neutropenia, and alopecia have been associated with albendazole use, continuous treatment has exhibited promising outcomes with manageable side effects [14]. The suggestion that long‐term albendazole (ABZ) treatment may serve as a safe and effective therapeutic approach for individuals with disseminated abdominal cystic echinococcosis highlights the importance of clinical trials to outline the optimal management strategies for this parasitic infection [15].
Estimations indicate a predominant global prevalence of individuals harboring hydatid cysts, with the potential to result in prominent morbidity and mortality in the absence of timely intervention [16].
Conclusion
8
This case highlights the challenges in diagnosing ovarian hydatid cysts, which can be mistaken for other ovarian conditions. Early detection is crucial, especially in endemic regions, for accurate management. Imaging tests aid in diagnosis, but histopathological examination confirms it. Surgery and anthelmintic therapy are key for treatment, reducing recurrence risks. This highlights the need to consider hydatid disease in ovarian cyst diagnoses, even without prior history. A multidisciplinary approach is essential for effective management of this rare condition.
Author Contributions
Fatemeh Asadi Kohbad: conceptualization. Razieh Akbari: supervision. Maryam Forouzin: writing – original draft. Fatemeh Nili: investigation, methodology. Leila Asadi: writing – review and editing. Marjan Ghaemi: investigation.
Funding
The authors have nothing to report.
Consent
Informed written and verbal consent was obtained from the patient for the publication of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1L. Cattorini , S. Trastulli , D. Milani , et al., “Ovarian Hydatid Cyst: A Case Report,” International Journal of Surgery Case Reports 2, no. 6 (2011): 100–102.22096695 10.1016/j.ijscr.2010.12.005PMC 3199687 · doi ↗ · pubmed ↗
- 2A. S. Khachatryan , “Analysis of Lethality in Echinococcal Disease,” Korean Journal of Parasitology 55, no. 5 (2017): 549–553.29103270 10.3347/kjp.2017.55.5.549PMC 5678460 · doi ↗ · pubmed ↗
- 3D. P. Mc Manus , W. Zhang , J. Li , and P. B. Bartley , “Echinococcosis,” Lancet 362, no. 9392 (2003): 1295–1304.14575976 10.1016/S 0140-6736(03)14573-4 · doi ↗ · pubmed ↗
- 4R. Makhlouf , A. Gamoudi , T. Bouzid , et al., “Hydatid Cyst of Ovary. Report of 7 Cases,” La Tunisie Médicale 84, no. 9 (2006): 592–594.17263211 · pubmed ↗
- 5A. A. Mohammed and S. H. Arif , “Hydatid Cyst of the Ovary–a Very Rare Type of Cystic Ovarian Lesion: A Case Report,” Case Reports in Women's Health 31 (2021): e 00330.10.1016/j.crwh.2021.e 00330 PMC 817302634123734 · doi ↗ · pubmed ↗
- 6M. Khosravi Maharlooei , A. Attar , A. Goran , S. Amuee , A. Dehghan , and A. Monabati , “Hydatid Cyst of Ovary: A Case Report,” Iranian Journal of Medical Sciences 34, no. 1 (2009): 76–79.
- 7B. Geramizadeh , “Unusual Locations of the Hydatid Cyst: A Review From Iran,” Iranian Journal of Medical Sciences 38, no. 1 (2013): 2–14.23645952 PMC 3642939 · pubmed ↗
- 8S. R. Mousavi , M. Samsami , M. Fallah , and H. Zirakzadeh , “A Retrospective Survey of Human Hydatidosis Based on Hospital Records During the Period of 10 Years,” Journal of Parasitic Diseases 36, no. 1 (2012): 7–9.23542872 10.1007/s 12639-011-0093-9PMC 3284625 · doi ↗ · pubmed ↗