Institut Georges Lopez-2M as a Novel Lung Preservation Solution Attenuates Ischemia-Reperfusion Injury in a Rat Ex Vivo Lung Perfusion Model
Annalisa Barbarossa, Jan Van Slambrouck, Cara Trivett, Phéline Kortleven, Cedric Vanluyten, Alberto Martin Medina, Xin Jin, Nicole Jannis, Balin Özsoy, Sandra Claes, Dominique Schols, Tine Wylin, Karen Moermans, Steve Stegen, Arnau Panisello Rosello, Ilhan Inci, Paul De Leyn

TL;DR
A new lung preservation solution, IGL-2M, reduces lung injury during cold storage in a rat model, showing better protection than existing solutions.
Contribution
IGL-2M is a novel preservation solution that effectively reduces ischemia-reperfusion injury in lungs.
Findings
IGL-2M reduced edema formation and improved lung compliance compared to OCS.
IGL-2M showed lower inflammatory markers in perfusate and bronchoalveolar lavage.
IGL-2M was not inferior to Perfadex Plus and reduced TNF-α expression.
Abstract
Institut Georges Lopez-2M (IGL-2M), a novel preservation solution containing polyethylene glycol (PEG 35kD, 5 g/L), preserves mitochondrial integrity and redox balance in liver grafts. This study assesses IGL-2M’s effect on lung preservation during prolonged cold ischemia. Rat’s heart-lung blocks were procured and subjected to 18 h cold ischemia (4 °C). Lungs were flushed and preserved using one of these preservation solutions: OCS, Perfadex Plus, IGL-2M (n = 6/group). Following ischemia, lungs underwent up to 7 h normothermic ex vivo lung perfusion. Edema was quantified by weight gain. Lung physiological parameters were recorded. Perfusate, bronchoalveolar lavage (BAL), and tissue samples were collected. All lungs in IGL-2M group completed 7 h EVLP protocol. Compared to OCS, IGL-2M reduced edema formation (p < 0.01), preserved superior compliance (p < 0.01), and maintained lower…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
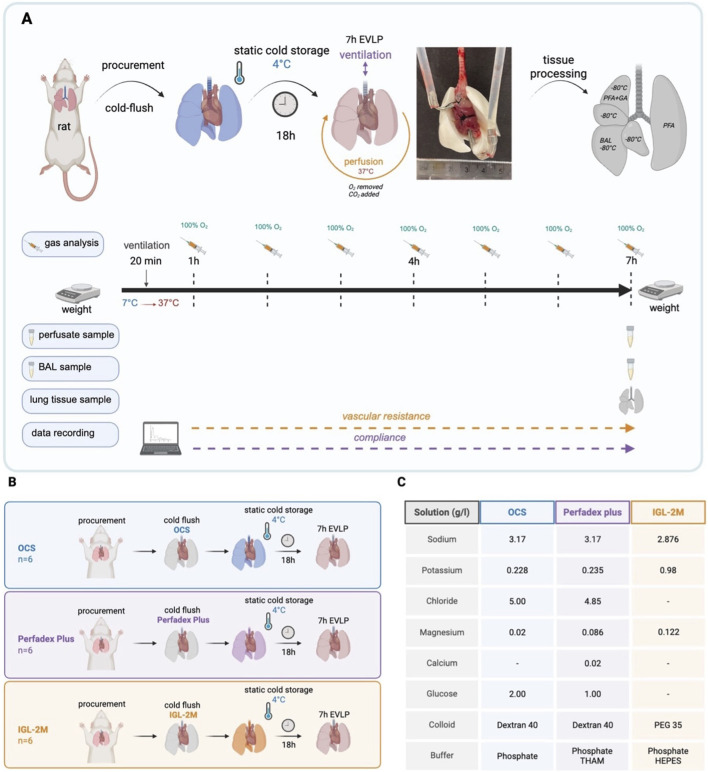 FIGURE 1
FIGURE 1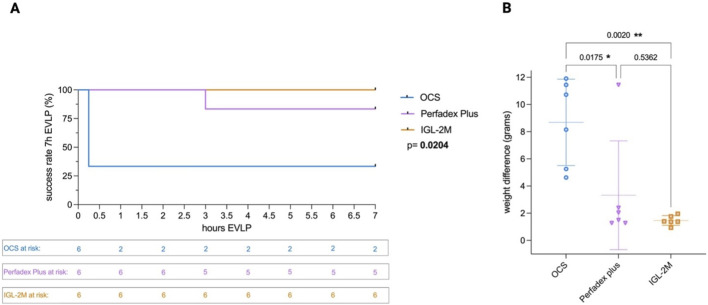 FIGURE 2
FIGURE 2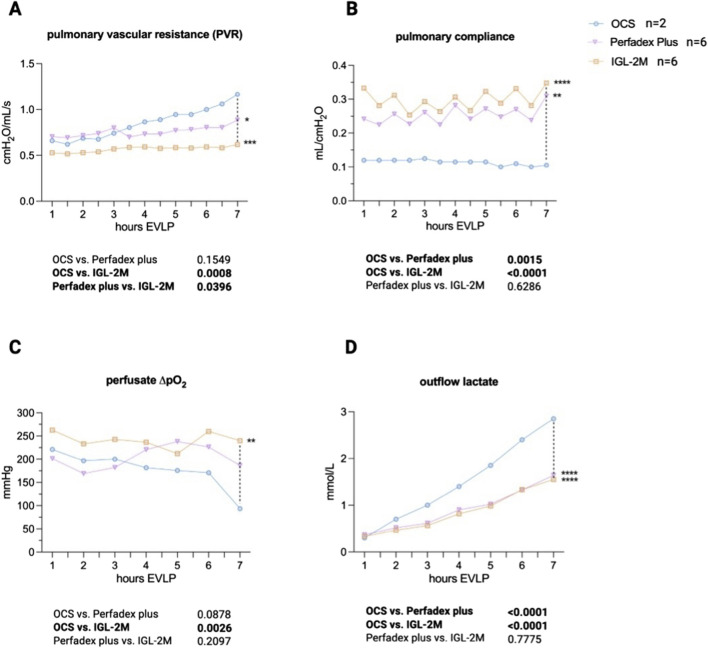 FIGURE 3
FIGURE 3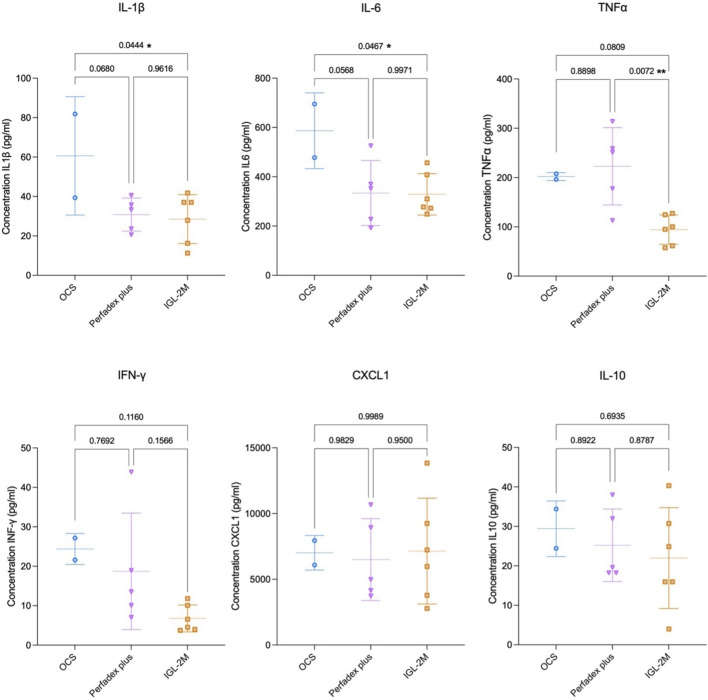 FIGURE 4
FIGURE 4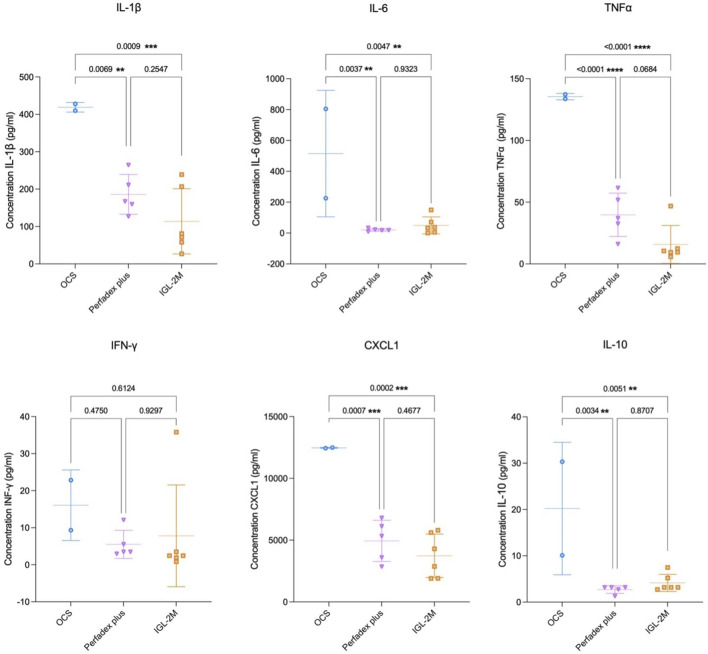 FIGURE 5
FIGURE 5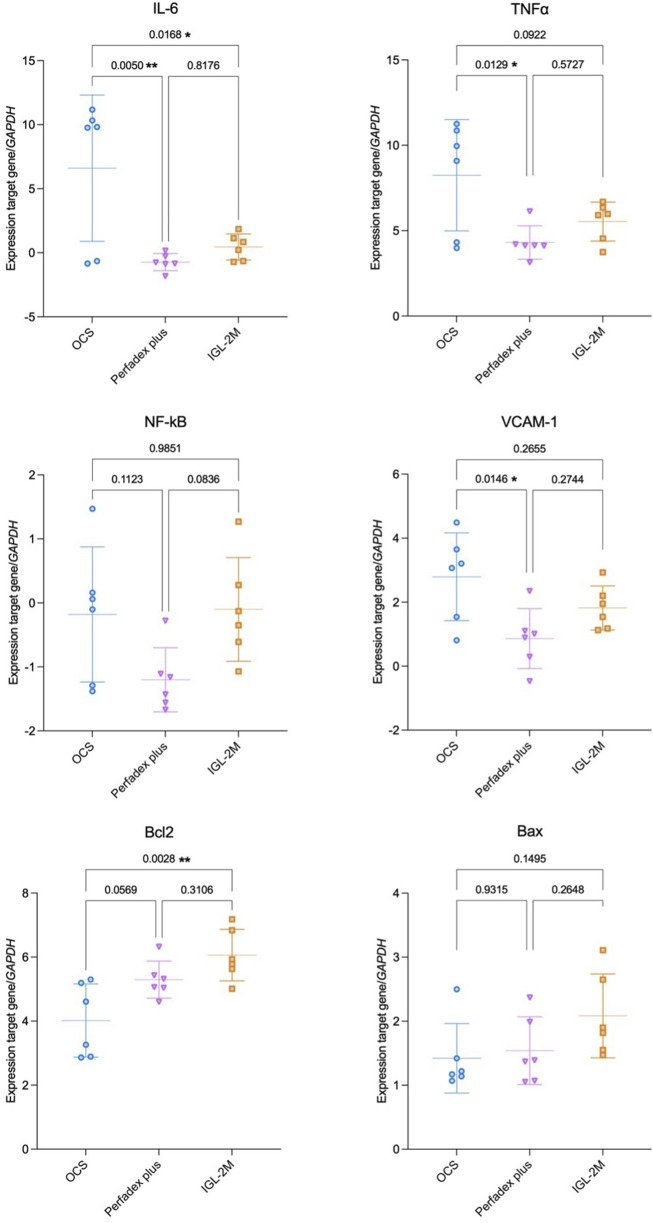 FIGURE 6
FIGURE 6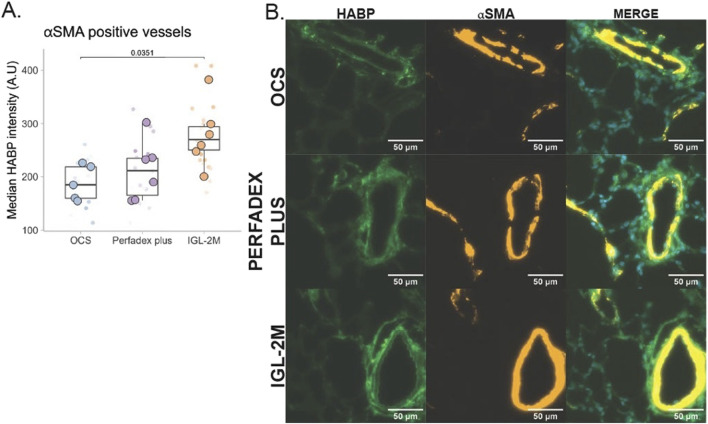 FIGURE 7
FIGURE 7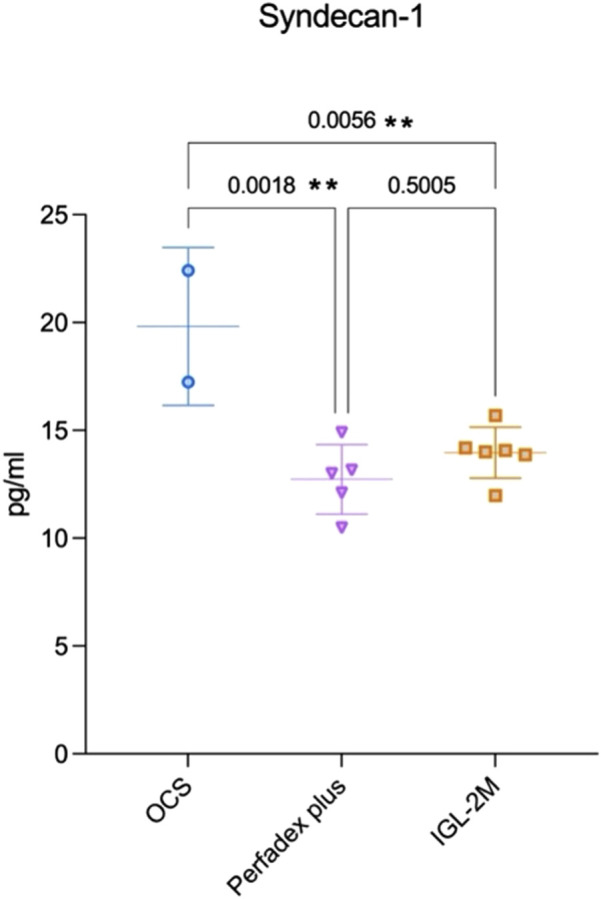 FIGURE 8
FIGURE 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Organ Transplantation Techniques and Outcomes · Cardiac Ischemia and Reperfusion
Introduction
Ischemia–reperfusion injury (IRI) is one of the key challenges in lung transplantation and plays a pivotal role in the development of primary graft dysfunction (PGD), leading to early morbidity and mortality [1]. The sequence of ischemia during organ procurement, static cold storage, and subsequent reperfusion after implantation triggers a cascade of cellular and molecular events that culminate in tissue injury [2]. At the onset of ischemia, an imbalance between metabolic supply and demand disrupts epithelial and endothelial homeostasis, alters mitochondrial function, and induces ionic disequilibrium. Cold preservation further amplifies this process through the generation of reactive oxygen species (ROS), inflammatory cytokine release, microvascular injury, and epithelial barrier disruption, ultimately resulting in lung edema and PGD following reperfusion [3, 4].
A central element in IRI is the inflammatory response, which is amplified upon reperfusion. Pro-inflammatory cytokines such as IL-1β, IL-6 and TNF-α, play a key role by activating endothelial cells, promoting leukocyte adhesion, and increasing vascular permeability [5, 6]. Chemokines like CXCL1 further drive neutrophil recruitment, while dysregulation of anti-inflammatory mediators such as IL-10 contributes to an imbalance between pro- and anti-inflammatory signaling [7, 8]. This cytokine storm accelerates endothelial dysfunction, microcirculatory failure, and edema formation, ultimately impairing graft function, leading to PGD [9].
Progress in optimizing lung preservation remains limited. Current preservation solutions differ across centers but share common design principles: colloids to counteract cellular edema, buffers to stabilize pH, antioxidants to scavenge ROS, and metabolic precursors to support ATP regeneration [10, 11]. However, clinical outcomes indicate that existing solutions provide partial protection, and novel approaches are needed to better preserve vascular integrity and attenuate IRI, especially in the context of evolving lung preservation practices toward controlled hypothermic storage and prolonged preservation time [12].
One promising strategy involves the use of polyethylene glycol (PEG)-based preservation solutions. Institut Georges Lopez-2 (IGL-2®), with PEG 35 kDa at 5 g/L, has been shown to stabilize mitochondrial function, preserve redox balance, and reduce endothelial injury in experimental liver transplantation [13, 14].
The aim of this study is to evaluate whether a further modified PEG-based preservation solution IGL-2M improves lung preservation during prolonged cold ischemia compared to clinically used Organ Care System lung solution (OCS) and Perfadex Plus. The primary endpoint of the study is to assess the success rates of 7 h of EVLP and edema formation. We analyzed the effect on edema, inflammation, and endothelial injury, using a rat ex vivo lung perfusion (EVLP) model to mimic IRI.
Materials and Methods
Animals
Male Sprague-Dawley rats (350–400 g, Janvier Labs, France) received adequate care, and the study was performed after authorization by local Ethical Committee for Animal Experimentation (Ethische Commissie Dierproeven) (P128/2023).
Surgical Techniques
Rats were anesthetized with 5% isoflurane and maintained with 3% isoflurane during lung procurement. A tracheostomy was performed, followed by mechanical ventilation with rodent ventilator (R415VentStarSmallAnimalVentilator; RWD Life Science Co., Ltd. Guangdong, P.R. China). A tidal volume (TV) of 8 mL/kg, ventilatory rate (VR) of 70/min, positive end-expiratory pressure (PEEP) of 3cmH_2_O, and a fraction of inspired oxygen (FiO_2_) of 50% were applied. A laparotomy was performed, and 200U/kg heparin (LeoPharma, Denmark) was injected into abdominal caval vein followed by sternotomy with removal of thymus to gain access to the pulmonary artery (PA). Exsanguination was obtained by cutting abdominal caval vein. The PA (inflow) was cannulated through an incision in the right ventricular outflow tract, while left atrium (outflow) was cannulated through an incision in the apex of left ventricle and after dilatation of mitral valve. Cold pulmonary antegrade flush was performed using one of three preservation solutions (20cc at 4 °C): OCS, Perfadex Plus, IGL-2M and 500U heparin. After pulmonary flush, pneumonectomy was performed. Trachea was clamped at inspiration and transected. The heart-lung block was weighed, submerged in same cold preservation solution used for the flush, and stored for 18 h in a temperature-controlled cold room at 4 °C. A cold ischemic time of 18 h was chosen to establish a severe, robust and reproducible injury model that mimics ischemia reperfusion injury, thereby enabling discrimination between preservation solutions under extreme conditions, which would not be achievable with shorter cold ischemia times.
Ex-Vivo Lung Perfusion
Lungs were mounted on an isolated perfused lung system for rats (IPL-2 platform; Hugo-Sachs Elektronik, Germany). The ex vivo lung perfusion protocol used was inspired by the protocols employed in the research laboratories of Lausanne and Zurich [15, 16]. A 75 mL of acellular albumin-rich Steen solution (XVIVO, Sweden) at 7 °C was used as perfusate supplemented with 1 mL of diluted Tham Koler 3M. Flow-controlled perfusion was started at 1% of cardiac output (CO) and was increased to 7.5% CO at incremental steps within 20 min. Perfusate temperature was increased to 37 °C within 25 min. Volume-controlled ventilation was started after 20 min reperfusion time at a 3 mL/kg TV, 10/min VR, 21% FiO_2_ and 3cmH_2_O PEEP. TV was increased to 6 mL/kg and VR to 30/min after 30min. The perfusate was continuously deoxygenated through a membrane filter (D150, Medica, Italy) with a 12% CO_2_/6% O_2_/82% N_2_ sweep gas. A recruitment maneuver with a TV of 10 mL/kg was performed every hour, followed by 3min of ventilation at 100% FiO_2_ and subsequent gas analysis of inflow and outflow perfusate samples (ABL800 FLEX, Radiometer, Denmark). Differential perfusate pO_2_ (outflow-inflow) (ΔpO_2_) and outflow perfusate lactate levels were recorded.
Respiratory physiology data were measured and recorded using dedicated software (Pulmodyn HSE software, Germany). Pulmonary arterial pressure (PAP), pulmonary vascular resistance (PVR), and compliance were monitored. Left atrium pressure was set at 2-3 cmH2O. Hourly outflow perfusate samples (1 mL) were collected, immediately snap frozen in liquid nitrogen and stored at −80 °C.
EVLP protocol was continued for a total of 7h, unless massive edema impeding further ventilation forced a premature stop to prevent fluid from reaching the trachea, afterwards heart-lung block was weighed. Prolonged EVLP (7 h) was chosen to allow clear detection of inflammatory differences between groups. An EVLP model to mimic reperfusion, rather than a transplant model, was used to reduce animals required. Bronchoalveolar lavage (BAL) samples of 1 mL 0.9% NaCl were collected from right lower lobe and snap-frozen in liquid nitrogen. Left lobe was instilled and fixed with 4% formaldehyde (Avantor, U.S). Remaining lobes were snap-frozen in liquid nitrogen and stored at −80 °C (Figure 1A).
(A) Experimental protocol and ex vivo lung perfusion sampling. (B) Study groups; (C) Composition of preservation solutions. Information about OCS solution’s composition was found on the clinic bag that held the solution. Details about Perfadex Plus were found on XVIVOgroup website, and information about IGL-2M was provided by IGL-company. Created in https://BioRender.com.
Study Groups and Preservation Solutions
Cold pulmonary antegrade flush and static preservation were performed using one of three preservation solutions: OCS lung solution (TransMedics), Perfadex Plus (XVIVO), or IGL-2M (Institut Georges Lopez 2 modified) after unblinded randomization.
For each group (n = 6/group), the lungs were flushed with 20cc sterile preservation solution, pre-cooled to 4 °C, via pulmonary artery during procurement. Lungs were then preserved in the specific preservation solution at 4 °C for 18 h. After the preservation phase, EVLP was performed (Figure 1B). During EVLP, Steen solution (XVIVO, Sweden) was used as perfusate for all groups.
OCS lung solution is an FDA-cleared extracellular, low-potassium solution based on colloid Dextran 40 (50 g/L). It is used in clinics for normothermic perfusion and in our center for static cold preservation of donor lungs.
Perfadex Plus is a ready-to-use extracellular colloid-based (Dextran 40, 50 g/L) and is used by most lung transplant centers for cold flush and static preservation. Unlike OCS, Perfadex Plus is pre-buffered and pre-supplemented with calcium ions and THAM.
IGL-2M is a novel polyethylene glycol (PEG-35kDa) based extracellular preservation solution, representing a modified version of IGL-1 and IGL-2 with improved antioxidant and anti-inflammatory properties. Originally designed to offer protection for steatotic livers [17]. It has not been used in clinic (Figure 1C)
Perfusate Samples, Bronchoalveolar Lavage Samples, and Lung Tissue Analysis
For analysis of cytokines, a 50 μL volume of either perfusates collected at 7 h EVLP and BAL was assayed using Rat Procarta 6-plex Luminex assay (Thermo Fisher Scientific).
RNA was isolated from frozen tissue biopsies. 25mg of frozen tissue RNA from the upper, middle, lower, and accessory lobes was combined with a 3 mm tungsten carbide bead (Qiagen, Ref#69997) and 300 µL of Aurum™ RNA lysis buffer (Bio-Rad, Ref#7326820), then homogenized using a TissueLyser II (Qiagen). RNA extraction was performed with TRIzol™ Reagent (Thermo Fisher Scientific, Ref#15596026) following the manufacturer’s protocol, and the RNA phase was further purified using the Aurum™ Total RNA Mini Kit (Bio-Rad, Ref#7326820). The RNA concentration and purity were assessed using NanoDrop oneC (Thermo Fisher Scientific). c-DNA was synthesized from 200 ng RNA using Moloney Murine Leukemia Virus Reverse Transcriptase (M-MLV, Life Technologies, CA, USA). Next, the real-time qPCR reaction was performed on a LightCycler 96W system (Roche Diagnostics, Vilvoorde, Belgium) with Taqman Fast Universal PCR Master Mix and Taqman Gene Expression Assays IL-1β (Gene expression assay: Rn00580432_m1), IL-6 (Gene expression assay: Rn01410330_m1), TNF-α (Gene expression assay: Rn00562055_m1), NFKB (Gene expression assay: Rn01399572_m1), VCAM-1 (Gene expression assay: Rn00563627_m1), Bcl2 (Gene expression assay: Rn99999125_m1), Bcl2l1 (Gene expression assay: Rn00437783_m1), bax (Gene expression assay: Rn01480160_g1) and TaqMan^®^ Fast Universal PCR Master Mix (Applied Biosystems^®^, Life Technologies, CA, USA). Thermocycling conditions consisted of an initial denaturation of 60s at 95 °C, followed by 45 cycles of 95 °C for 5s and 60 °C for 30s. Quantification of input target amount was analyzed by cycle threshold (Ct) value, the point at which the sample PCR amplification plot crosses the threshold. All data were normalized to GAPDH (Gene expression assay: Rn00562055_m1), and differences in gene expression were calculated as dCt values.
Lung Tissue Staining for Hyaluronan-Binding Protein
Paraffin-embedded sections were used for hyaluronic acid staining using a biotinylated hyaluronan binding protein (Sigma, 385911-50UG). Sections were baked at 65 °C and allowed to cool completely. Deparaffinization and dehydration were performed by sequentially immersing slides in xylene followed by a reducing ethanol gradient (100%, 95%, 70%, 50%). Slides were then washed once with distilled water before performing antigen retrieval (Target Retrieval Solution, Dako). Following incubation with protein blocking solution (TNB protein blocking solution) and endogenous biotin blocking (Biolegend) samples were incubated in solution containing hyaluronan binding protein (1/100) and αSMA-Cy3 antibody (1/400, Sigma, C6198) overnight with gentle rocking. Slides were washed three times with TNT Buffer (0.1M Tris.HCl (pH 7.5), 0.15M NaCl, 0.05% Tween®-20). To detect bound hyaluronan, slides were incubated in the dark with streptavidin conjugated to Alexa488 (1/400, Thermo Fisher Scientific) for 1 h. Slides were washed three times in TNT, counterstained with DAPI and mounted with ProLong™ Gold Antifade Mountant (Thermo Fisher Scientific). All steps were performed at room temperature.
Fluorescent images were taken with a Zeiss 700 M confocal microscope (×20 magnification). Per animal, 3-4 tiled regions were captured. Images were analyzed using ImageJ software (Fiji). First each channel underwent background subtraction. Image segmentation was achieved using Cy3 channel to identify αSMA positive vessels. Images were then binarized using the triangle algorithm for thresholding. The binary image was converted to a mask and Cy3+ve areas were eroded to remove small particles, remaining positive areas were then dilated to capture the areas surrounding vessels. The segmented image was used to define measured areas on 488-channel image by redirecting measurements and using the “Analyze Particles” function in ImageJ. Results per image were written to csv files analyzed in R4.5.1.
Statistics
Continuous physiology and weight data were reported as mean with SD. Edema was quantified by measuring difference in heart-lung block weight after vs. before EVLP. Repeated measurements were compared using 2-way analysis of variance (ANOVA). Static data were compared using one-way ANOVA. Statistical significance was assigned to a p < 0.05. GraphPad Prism Version 10.3.1 was used for all statistical analyses.
Results
IGL-2M Prevents Edema Development After Prolonged Static Cold Preservation
All six IGL-2M experiments reached 7 h EVLP. In Perfadex Plus group, 5/6 experiments reached 7 h EVLP while one experiment failed prematurely after 3 h due to massive edema. In OCS group 2/6 reached 7 h EVLP while 4 experiments failed prematurely after 0.25 h due to massive edema (p < 0.05) (Figure 2A).
Proportion of experiments developing edema. (A) 7 h ex vivo lung perfusion success rate. Log-rank test: p < 0.05. (B) Lung weight gain after ex vivo lung perfusion. Statistical analysis was performed using one-way ANOVA.
Weight difference between heart-lung block after vs. before EVLP was taken as indicator of edema development. Weight gain in IGL-2M group was lower compared to OCS (p < 0.01) and no significant difference was found compared to Perfadex Plus (p = 0.54) (Figure 2B).
IGL-2M Results in Stable Pulmonary Vascular Resistance and Results in Higher Pulmonary Compliance Compared to OCS
After 7 h EVLP, pulmonary vascular resistance remained stable and was lower in IGL-2M compared to OCS, which showed a worsening trend over time (p < 0.01) and Perfadex Plus (p < 0.05) (Figure 3A). Compliance was higher in IGL-2M than in OCS, which started with a lower value from the beginning (p < 0.01), with no difference compared to Perfadex Plus (p = 0.63) (Figure 3B). Pulmonary gas exchange was evaluated using perfusate ΔpO2, showing better oxygenation in IGL-2M than in OCS (p < 0.01) and no difference compared to Perfadex Plus (p = 0.21) (Figure 3C). Cellular damage was assessed by lactate levels in the effluent, with both IGL-2M and Perfadex Plus having lower lactate levels than OCS (p < 0.01) with a trend over time (Figure 3D).
Physiological data during 7 h ex vivo lung perfusion. (A) Pulmonary vascular resistance. (B) Pulmonary compliance. (C) Perfusate oxygenation (differential outflow minus inflow partial O2 pressure). (D) Outflow lactate levels. Statistical analysis was performed using two-way ANOVA.
IGL-2M Results in a Limited Release of Inflammatory Biomarkers in the Perfusate
Perfusate samples collected after 7 h EVLP in IGL-2M showed lower concentrations of pro-inflammatory cytokines IL-1β (p < 0.05) and IL-6 (p < 0.05) compared to OCS, and no difference compared to Perfadex Plus (p = 0.96; p = 0.99). IGL-2M showed the lowest concentration of TNF-α (vs. OCS p = 0.08; vs. Perfadex plus p < 0.05). Compared to OCS, Perfadex Plus showed a trend towards lower inflammatory cytokine release (Figure 4).
Cytokine expression in the perfusate at 7 h of ex vivo lung perfusion. Data are plotted as effective concentrations (pg/mL). Statistical analysis was performed using one-way ANOVA.
IGL-2M Results in a Limited Release of Inflammatory Biomarkers in the Bronchoalveolar Lavage
BAL samples collected after 7 h EVLP in IGL-2M showed reduced release of pro-inflammatory cytokines IL-1β (p < 0.01); IL-6 (p < 0.01); TNF-α (p < 0.01); CXCL1 (p < 0.01) and anti-inflammatory cytokine IL-10 (p = 0.05) compared to OCS; and no difference for the same biomarkers compared to Perfadex Plus. Compared to OCS, Perfadex Plus showed reduced release of IL-1β (p < 0.05); IL-6 (p < 0.01); TNF-α (p < 0.01); CXCL1 (p < 0.01) and anti-inflammatory cytokine IL-10 (p < 0.01) (Figure 5).
Cytokine expression in the bronchoalveolar lavage samples at 7 h of ex vivo lung perfusion. Data are plotted as effective concentrations (pg/mL). Statistical analysis was performed using one-way ANOVA.
IGL-2M and Perfadex Plus Reduce Inflammation in Lung Tissue
Lung tissue analysis with RT-qPCR showed lower IL-6 gene expression (p < 0.05) in IGL-2M compared to OCS, with no difference compared to Perfadex Plus (p = 0.82). Compared to OCS, Perfadex Plus showed lower gene expression of IL-6 (p < 0.01); TNF-α (p < 0.05); VCAM-1 (p < 0.05) (Figure 6).
The mRNA expression of cytokines, transcription factor (NF-kB), adhesion molecule (VCAM-1) and proteins involved in the apoptotic signaling in the lung tissue were quantified relative to the housekeeping gene GAPDH after ex vivo lung perfusion. Statistical analysis was performed using one-way ANOVA.
IGL-2M Induces the Expression of Anti-apoptotic Gene
The anti-apoptotic Bcl2 gene expression was higher in IGL-2M (vs. OCS, p < 0.01) with no difference compared to Perfadex Plus (p = 0.31) (Figure 6).
Hyaluronan Associated With the Lung Endothelium Is Preserved With IGL-2M
Hyaluronan detected by biotinylated hyaluronan-binding protein was present in the adventitia of αSMA positive vessels, as well as in the bronchial and bronchiolar epithelium, in the region of the basement membrane. Hyaluronan levels were decreased in αSMA positive vessels across the groups (F (2, 14) = 4.384, p < 0.05). Lungs preserved with OCS showed reduced vascular hyaluronan levels as compared to IGL-2M preserved lungs (Figure 7, p < 0.05).
Vascular hyaluronan was quantified using the Hyaluronan Binding Protein (HABP), co-stained with α smooth muscle actin (αSMA), in the rat lung after ex vivo lung perfusion. (A) Median intensity of HABP signal around αSMA positive vessels. Smaller points represent median intensity values from individual images. Large circles represent the average intensity derived from the individual images obtained per animal. (B) representative image of binding protein (green) positive co-localized with αSMA (orange). Statistical analysis was performed using one-way ANOVA.
IGL-2M and Perfadex Plus Preserve Endothelial Glycocalyx Integrity Compared to OCS
Perfusate samples collected after 7 h EVLP in IGL-2M and Perfadex Plus showed lower concentrations of Syndecan-1 compared to OCS (p < 0.05; p < 0.01) (Figure 8).
Syndecan-1 expression in the perfusate at 7 h of ex vivo lung perfusion. Data are plotted as effective concentrations (pg/mL). Statistical analysis was performed using one-way ANOVA.
Discussion
This rat model of prolonged lung preservation assessed over 7 h EVLP shows for the first time that IGL-2M, a PEG-based preservation solution, can be successfully used to flush and preserve rat lungs subjected to prolonged cold ischemia of 18 h. Compared to OCS, IGL-2M markedly reduced edema formation, preserved pulmonary vascular resistance and compliance, improved oxygenation, reduced lactate release, and attenuated the inflammatory cytokine response. IGL-2M was not inferior to Perfadex Plus, the current gold standard, and showed an additional effect of TNF-α suppression.
PGD remains a leading cause of early morbidity and mortality after lung transplantation, with an incidence of 30%, largely driven by IRI. While IRI encompasses the cascade of cellular metabolic, inflammatory, and endothelial responses initiated by ischemia and reperfusion, PGD is the clinical manifestation characterized by pulmonary edema, hypoxemia, and impaired compliance [1]. One key feature of IRI is microvascular leakage secondary to endothelial barrier disruption, resulting in uncontrolled transvascular fluid and leukocyte extravasation [4, 18].
Controlled hypothermic storage (CHS) has been introduced in clinical practice, reshaping static lung preservation and allowing prolonged ischemic time [12, 19, 20]. Therefore, minimizing ischemic damage is a key area of investigation. One of the strategies to reduce IRI is to explore new preservation solutions, where the components should aim to prevent the inflammatory processes that typically start during preservation. Minimizing the inflammatory response to ischemia and strengthening endothelial barrier integrity are key therapeutic strategies for reducing IRI and decreasing the incidence of PGD. Our data show that lungs preserved with IGL-2M had less edema, lower expression of pro-inflammatory cytokines such as IL-1β, IL-6, TNF-α, and CXCL1, and reduced shedding of syndecan-1, supporting improved preservation of endothelial integrity compared to OCS.
The Perfadex Plus is the most widely used lung preservation solution [21], with OCS lung solution used in the context of portable normothermic perfusion [22]. Both solutions are dextran-based. Perfadex Plus is pre-buffered with THAM and supplemented with calcium, which stabilizes endothelial junctions and maintains contractile tone [23]. This likely explains the superior protection compared to OCS observed in our model, where lungs preserved with Perfadex Plus developed less edema and released lower levels of inflammatory mediators in perfusate, BAL, and tissue. On the other hand, IGL-2M replaces dextran with PEG 35kDa, adding anti-inflammatory, antioxidant, and membrane-stabilizing effects [24, 25]. Our data indicate that IGL-2M achieves similar preservation compared to Perfadex Plus, while showing an additional anti-inflammatory effect through TNF-α suppression.
Physiologically, IGL-2M-preserved lungs showed stable and lower pulmonary vascular resistance from the onset of reperfusion, whereas OCS-preserved lungs had a progressive rise in resistance during EVLP. Compliance followed a similar pattern, with better compliance in the IGL-2M group already at the start of reperfusion. These early differences suggest that lungs preserved with IGL-2M experienced less structural and molecular damage during ischemia, allowing for more favorable baseline function when reperfusion began. The vascular staining of HA is likely around veins and venules, both based on structure and previous reports [26]. HA is essential in controlling permeability, but also plays a structural role and affects inflammation [27]. PEG has been shown to stabilize endothelial junctions by promoting VE-cadherin clustering and reducing paracellular gap formation [28]. The protective role of PEG 35 kDa in IGL-2M is further supported by in vitro studies demonstrating up to a 125% increase in transendothelial electrical resistance (TEER), sustained for over 40 h, compared to the transient effects of other agents. PEG reduces paracellular permeability to FITC-dextran by more than fourfold [28]. Together, these cellular mechanisms likely explain the lack of edema, the immediate physiological stability during EVLP, the decreased vascular leak, lower pulmonary vascular resistance, and reduced inflammatory cytokine release observed in IGL-2M-preserved lungs.
IGL-2M showed an anti-inflammatory effect at multiple levels. Perfusate analysis demonstrated reduced IL-1β and IL-6 compared to OCS, while BAL samples showed lower release of IL-1β, IL-6, TNF-α, and CXCL1. These findings were corroborated by tissue analysis, where IL-6 expression was reduced, and Bcl2 expression increased, indicating anti-apoptotic signaling. Moreover, IGL-2M suppressed TNF-α release compared to both OCS and Perfadex Plus. TNF-α plays a central role in IRI by amplifying endothelial activation, promoting leukocyte adhesion, and driving vascular leak [5]. Its reduction in the IGL-2M group points to PEG-mediated modulation of intracellular signaling pathways, beyond colloid effects alone.
Whether this effect will translate into reduced rates of PGD in clinical transplantation remains to be determined.
Perfadex Plus also demonstrated clear anti-inflammatory effects compared to OCS, lower levels of IL-1β, IL-6, TNF-α, CXCL-1 and IL-10, consistent with its calcium supplementation. Calcium is essential for preserving endothelial and epithelial integrity by stabilizing adherens junctions. Perfadex Plus contains a modified dextran formulation with a lower viscosity and carefully balanced electrolyte/osmolarity profile, reducing the risk of vascular leak. This likely accounts for the lower edema and reduced cytokine release observed in the Perfadex Plus group. Thus, while both solutions limit inflammation and preserve function, they probably act through different mechanisms: calcium-mediated stabilization for Perfadex Plus and PEG-mediated for IGL-2M.
Our findings are consistent with prior studies in liver transplantation, where PEG-containing solutions have been shown to preserve mitochondrial function, redox balance, and endothelial glycocalyx integrity more effectively than traditional solutions [25, 29–32]. PEG has also demonstrated anti-inflammatory, immunosuppressive, and cell-membrane-stabilization effects in the setting of intestinal IRI, increasing with higher dose [33–36]. The reproducibility of PEG’s protective effects across organs suggests the feasibility of a universal preservation solution. A single PEG-based formulation for multiple organs could streamline procurement, simplify logistics, and expand the use of marginal donors.
This study has several limitations. Firstly, the high failure rate in the OCS group reduced the number of evaluable data points at the 7 h EVLP time point to only n = 2. This affects the statistical power, so the 7 h comparison should be interpreted with caution. However, this reflects the inability of OCS-preserved lungs to withstand prolonged cold ischemia followed by EVLP, resulting in edema and endothelial injury, which serve as important biological indicators of inferior preservation capacity under extended cold ischemia, rather than a technical failure. Secondly, 18 h of cold ischemia may exceed the tolerance of the OCS, potentially leading to early EVLP failure. However, this observation is indicative of solution-specific performance rather than a real limitation inherent to the study design. Third, direct visualization of endothelial glycocalyx integrity was not possible due to the experimental setup, as HA is only one component of the glycocalyx. Nonetheless, an ongoing transmission electron microscopy study will offer further evidence. Fourth, since this is a rodent model, caution is needed when translating findings to human lungs. Fifth, mechanistic studies were limited by the limitation of obtaining sequential tissue samples during ischemia and reperfusion. Nevertheless, the robust physiological, biochemical, and inflammatory data provide consistent evidence supporting the protective role of IGL-2M.
Conclusion
IGL-2M preserved lung function during prolonged cold ischemia at least as effectively as Perfadex plus, with additional anti-inflammatory benefits on TNF-α. Compared with OCS, IGL-2M limited edema formation and improved physiological stability. These findings justify further evaluation of IGL-2M in large animal models and provide a strong rationale for clinical translation, with the potential to establish a single PEG-based fluid as a universal organ preservation solution.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Van Slambrouck J Van Raemdonck D Vos R Vanluyten C Vanstapel A Prisciandaro E A Focused Review on Primary Graft Dysfunction After Clinical Lung Transplantation: A Multilevel Syndrome. Cells (2022) 11(4):745. 10.3390/cells 11040745 35203392 PMC 8870290 · doi ↗ · pubmed ↗
- 2Van Slambrouck J Loopmans S Prisciandaro E Barbarossa A Kortleven P Feys S The Effect of Rewarming Ischemia on Tissue Transcriptome and Metabolome Signatures: A Clinical Observational Study in Lung Transplantation. J Heart Lung Transpl (2024) 44:S 1053249824019053. 10.1016/j.healun.2024.10.020 39486771 · doi ↗ · pubmed ↗
- 3Pizanis N Gillner S Kamler M De Groot H Jakob H Rauen U . Cold-Induced Injury to Lung Epithelial Cells Can Be Inhibited by Iron Chelators — Implications for Lung Preservation. Eur J Cardiothorac Surg (2011) 12:S 1010794011001199–955. 10.1016/j.ejcts.2011.01.052 21398140 · doi ↗ · pubmed ↗
- 4Ta HQ Kuppusamy M Sonkusare SK Roeser ME Laubach VE . The Endothelium: Gatekeeper to Lung Ischemia-Reperfusion Injury. Respir Res (2024) 25(1):172. 10.1186/s 12931-024-02776-4 38637760 PMC 11027545 · doi ↗ · pubmed ↗
- 5Krishnadasan B Naidu BV Byrne K Fraga C Verrier ED Mulligan MS . The Role of Proinflammatory Cytokines in Lung Ischemia-Reperfusion Injury. J Thorac Cardiovasc Surg (2003) 125(2):261–72. 10.1067/mtc.2003.16 12579094 · doi ↗ · pubmed ↗
- 6Ali MH Schlidt SA Chandel NS Hynes KL Schumacker PT Gewertz BL . Endothelial Permeability and IL-6 Production During Hypoxia: Role of ROS in Signal Transduction. Am J Physiol-Lung Cell Mol Physiol (1999) 277(5):L 1057–65. 10.1152/ajplung.1999.277.5.L 1057 10564193 · doi ↗ · pubmed ↗
- 7Eppinger MJ Ward PA Bolling SF Deeb GM . Regulatory Effects of Interleukin-10 on Lung Ischemia-Reperfusion Injury. Cardiovasc Surg (1996) 112(5):1301–5. 10.1016/S 0022-5223(96)70144-7 8911327 · doi ↗ · pubmed ↗
- 8Sharma AK Mulloy DP Le LT Laubach VE . NADPH Oxidase Mediates Synergistic Effects of IL-17 and TNF-α on CXCL 1 Expression by Epithelial Cells After Lung Ischemia-Reperfusion. Am J Physiol-Lung Cell Mol Physiol (2014) 306(1):L 69–79. 10.1152/ajplung.00205.2013 24186876 PMC 3920214 · doi ↗ · pubmed ↗