Association between the incidence of infusion-related reactions by obinutuzumab and the dose of corticosteroid as premedication: a multicenter retrospective cohort study
Tatsuya Ohtsubo, Kazuhiro Yamamoto, Saori Matumoto, Kaori Ito, Yuzuka Sasa, Kosuke Tomishima, Satoshi Dote, Katuya Makihara, Yoshinori Wakasugi, Tsutomu Mitsuie, Kouhei Yamagiwa, Kazuo Sato, Hiroki Hasegawa, Nobuhiko Uoshima, Yumi Kitahiro, Kanji Tomogane

TL;DR
This study found that higher corticosteroid doses and specific drug choices may reduce infusion-related reactions during obinutuzumab treatment.
Contribution
The study identifies associations between corticosteroid type and IRR incidence, offering guidance on premedication choices.
Findings
High-dose corticosteroids were linked to lower IRR incidence compared to low-dose.
Dexamethasone was associated with lower IRR risk than hydrocortisone or methylprednisolone.
Second-generation H1-receptor antagonists were better at preventing IRR than first-generation ones.
Abstract
Premedication with corticosteroids is recommended for prophylaxis against infusion-related reactions (IRRs) caused by obinutuzumab despite a lack of solid evidence regarding the dose of corticosteroids. The incidence rates of IRR in the high-dose and low-dose corticosteroid groups were investigated and compared using Student’s t-test.Univariable and multivariable logistic regression analyses were performed on patients to explore the risk of developing IRRs with obinutuzumab. The incidence of IRRs in the high-dose and low-dose corticosteroid groups at the initial administration of obinutuzumab was 27.0% (41/152) and 48.4% (31/64), respectively, indicating that the high-dose group had a lower incidence of IRRs (p = 0.002). The incidence of IRRs at the initial administration of obinutuzumab was significantly associated with the administration of first-generation histamine 1 receptor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
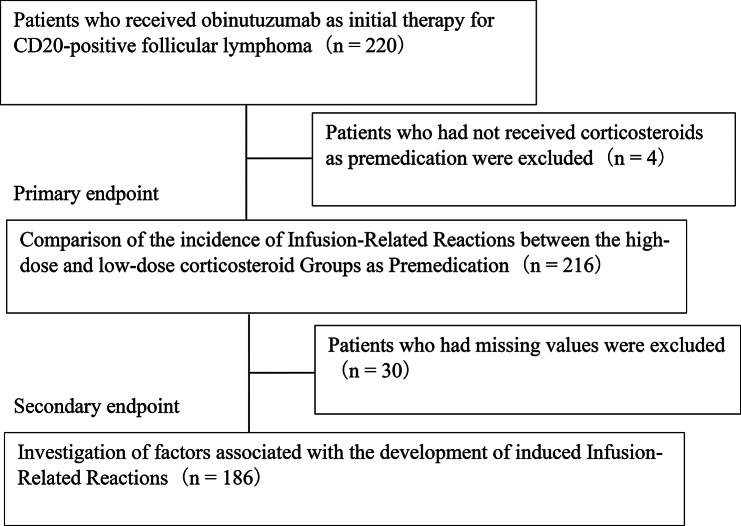 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal Hormones and Disorders · Chemotherapy-related skin toxicity · Heparin-Induced Thrombocytopenia and Thrombosis
Background
Obinutuzumab is a humanized anti-CD20 monoclonal antibody that is widely used for CD20-positive follicular lymphoma and chronic lymphocytic leukemia (including small lymphocytic lymphoma). In the GALLIUM study [1], which included patients with follicular lymphoma, patients who received obinutuzumab-based immunochemotherapy showed longer progression-free survival than those who received rituximab-based immunochemotherapy, making obinutuzumab-based immunochemotherapy a standard therapy for CD20-positive follicular lymphoma [2]. However, infusion-related reactions (IRRs) are observed as serious and frequent adverse events associated with obinutuzumab administration, which tend to occur during the initial administration [1, 3]. The incidence of IRRs in the obinutuzumab and rituximab groups in the GALLIUM study was 59% and 49% for all grades, respectively, and 11% and 5% for grades 3–5, respectively [1]. Obinutuzumab may result in the occurrence of IRRs more frequently than rituximab. Premedication with antipyretic analgesics, histamine 1 receptor antagonists, and corticosteroids is recommended for preventing IRRs caused by obinutuzumab [4, 5]. The U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) recommend corticosteroids such as prednisolone 100 mg, dexamethasone 20 mg, or methylprednisolone 80 mg, and explicitly state in the obinutuzumab package insert that hydrocortisone should not be used for IRR prevention because it is ineffective [4, 5]. However, the underlying evidence supporting this recommendation has not been established. Furthermore, although corticosteroid doses are expected to be reduced due to factors such as the presence of diabetes or the need to avoid severe infections, no published data exist regarding the corticosteroid doses, and no established dosing regimen is available. We aimed to standardize corticosteroid premedication at the time of initial obinutuzumab administration and to examine the association between corticosteroid dosage and IRR incidence.
Methods
Study participants
This multicenter retrospective cohort study was conducted at Japanese Red Cross Kyoto Daini Hospital, Fujita Health University Hospital, Japanese Red Cross Osaka Hospital, Kindai University Hospital, Japanese Red Cross Kyoto Daiichi Hospital, Kyoto Katsura Hospital, Yodogawa Christian Hospital, Shiga University of Medical Science Hospital, Japanese Red Cross Otsu Hospital, Saiseikai Shiga Hospital, Japan Baptist Hospital and Rakuwakai Otowa Hospital. Patients treated with obinutuzumab as initial therapy for primary or relapsed CD20-positive follicular lymphoma from August 1, 2018, to October 31, 2021, at collaborating institutions were included. The exclusion criteria were as follows: patients who take antipyretic analgesics (including nonsteroidal anti-inflammatory drugs), histamine 1 receptor antagonists, or corticosteroids other than those included in the regimen used before obinutuzumab administration and those who were not given corticosteroids as premedication on the same day as obinutuzumab administration.
Definition of the high-dose and low-dose corticosteroid groups
The high-dose group comprised patients who received 100 mg or higher of prednisolone, 80 mg or higher of methylprednisolone, or 16.5 mg or higher of dexamethasone as premedication. The low-dose group comprised patients who received a dose lower than that in the high-dose group or those who took hydrocortisone. The cutoff dose value for the high-dose and low-dose groups was established based on recommendations from the FDA and EMA. However, for dexamethasone, since domestic formulations display the dexamethasone content without phosphate, the reference values for low-dose and high-dose dexamethasone in this study were set at 16.5 mg, which was considered equivalent to 20 mg of dexamethasone phosphate. The corticosteroid equivalent was set as 20 mg of hydrocortisone, 5 mg of prednisolone, 4 mg of methylprednisolone, and 0.75 mg of dexamethasone in equal doses [6].
Definition of IRRs
IRRs incidence was determined from a physician’s documentation in the electronic medical record that IRRs (e.g., anaphylaxis, hypotension, nausea, chills, bronchospasm, pharyngeal or throat irritation, wheezing, laryngeal edema, atrial fibrillation, tachycardia, and hypersensitivity) occurred during obinutuzumab administration. In cases where there was no description regarding the incidence of IRRs in medical records, the attending physician performed a retrospective evaluation. The severity of IRRs was assessed by referring to the physician’s medical record. If no record was available regarding severity, each principal investigator assessed it based on “Infusion related reaction” in Common Terminology Criteria for Adverse Events version 5.0.
Statistical analysis
Continuous variables are presented as means (standard deviations) and were compared using Student’s t-test. Nominal variables are presented as numbers and percentages and were compared using the chi-square test. Univariable and multivariable logistic regression analyses were performed on patients without missing values to explore the risk of developing IRRs with obinutuzumab. The explanatory variables were staging (AnnArbor classification), B symptoms, sIL-2R, LDH, dosage and type of corticosteroid, and type of histamine antagonist [7–9]. Statistical analyses were performed using Statistical Package for the Social Sciences (version 23.0; IBM Corp., New York) with a significance level of 5%.
Results
Patient characteristics
Of the 220 patients who received obinutuzumab as initial therapy for CD20-positive follicular lymphoma, 216 were included, excluding four patients who did not receive corticosteroids as premedication on the same day as obinutuzumab administration (Fig. 1). The patient backgrounds in the high- and low-dose corticosteroid groups are shown in Table 1. The number of patients in the high- and low-dose groups was 152 and 64, respectively. The high-dose group had a significantly lower age and a significantly lower percentage of patients with clinical stage III or higher than the low-dose group. Furthermore, the high-dose group had a significantly higher percentage of patients with PS of 0 and untreated patients, significantly higher ALP levels, and a higher percentage of patients with azole antifungal drug use. The details of corticosteroids, histamine 1 receptor antagonists, and antipyretic analgesics used as premedication are shown in Table 2. The most commonly used corticosteroid was dexamethasone [n = 151 (69.9%)]. The most commonly used histamine 1 receptor antagonist and antipyretic analgesic were d-chlorpheniramine maleate [n = 96 (44.4%)] and acetaminophen [n = 125 (57.9%)], respectively.
Fig. 1. Research design overview
Table 1. Comparison of patient characteristics between high-dose and low-dose corticosteroid groupsHigh dose (n = 152)Low dose (n = 64)p-valueAge [Mean (SD)]66.4 (10.3)69.9 (9.2)0.019Sex, [n (%)]Male77 (50.7)35 (54.7)0.59PS [n (%)]0115 (75.6)31 (48.4)0.034≧ 136 (23.7)20 (31.3)Unknown1 (0.7)13 (20.3)Ann Arbor Staging [n (%)]< Ⅲ35 (23.0)5 (7.8)0.012≧Ⅲ114 (75.0)55 (85.9)Unknown3 (2.0)4 (6.3)Line [n (%)]Untreated94 (61.8)29 (45.3)0.025Relapsed58 (38.2)35 (54.7)BM involvement [n (%)]Yes56 (36.8)29 (45.3)0.066No90 (59.3)26 (40.6)Unknown6 (3.9)9 (14.1)Splenomegaly [n (%)]Yes32 (21.1)12 (18.8)0.67No118 (77.6)52 (81.2)Unknown2 (1.3)0 (0)B symptoms [n (%)]Yes20 (13.2)10 (15.6)0.29No129 (84.8)41 (64.1)Unknown3 (2.0)13 (20.3)ALP (U/L) (Mean, SD)224.6 (150.8)182.2 (91.1)0.042sIL-2R (U/mL) (Mean, SD)1925.6 (2948.2)2602.4 (4091.1)0.17LDH (U/L) (Mean, SD)211.8 (74.5)229.3 (105.2)0.17Hb (g/dL) (Mean, SD)12.7 (1.8)12.8 (2.1)0.81Combination regimen [n (%)]Bendamustine127 (83.6)58 (90.6)0.282CHOP21 (13.8)4 (6.3)CVP4 (2.6)2 (3.1)Concomitant drugs [n (%)]Aprepitant58 (38.2)21 (32.8)0.46Azole antifungal drugs25 (16.4)3 (4.7)0.02Macrolide antibiotics1 (0.7)0 (0)0.52Antipyretic analgesicAcetaminophen85400.37NSAIDs6724Types of corticosteroids [n (%)]DEX120 (79.0)31 (48.4)< 0.01HDC0 (0)28 (43.8)PSL11 (7.2)3 (4.7)mPSL21 (13.8)2 (3.1)Types of histamine antagonists [n (%)]First generations74 (48.7)56 (87.5)< 0.01Second generations67 (44.1)8 (12.5)First and second concomitant11 (7.2)0 (0)PS: performance status, BM: bone marrow, ALP: alkaline phosphatase, sIL-2R: soluble interleukin-2 receptor, LDH: lactate dehydrogenase, Hb: hemoglobin, CHOP: cyclophosphamide, doxorubicin, vincristine, prednisolone, CVP: cyclophosphamide, vincristine, prednisolone, NSAIDs: non-steroidal anti-inflammatory drug, DEX: dexamethasone, HDC: hydrocortisone, PSL: prednisolone, mPSL: methylprednisolone
Table 2. Summary of premedications for administration of obinutuzumabCategoryDrugDoseAdministration route n CorticosteroidDEX3.3 mgi.v.36.6 mgi.v.269.9 mgi.v.216.5 mgi.v.3219 mgi.v.1119.8 mgi.v.6833 mgi.v.9HDC15 mgi.v.1100 mgi.v.10200 mgi.v.16500 mgi.v.1PSL30 mgp.o.260 mgp.o.1100 mg100 mgp.o.i.v.65mPSL40 mgi.v.162.5 mgi.v.180 mgi.v.18100 mgi.v.1125 mgi.v.1250 mgi.v.1Antipyretic analgesicsAcetaminophen400 mgp.o.12500 mgp.o.57600 mgp.o.24800 mgp.o.3900 mgp.o.61000 mgp.o.61000 mgi.v.17Diclofenac25 mgp.o.5Loxoprofen60 mgp.o.86Antihistamined-Chlorpheniramine maleate(First generation)2 mgp.o.44 mgp.o.15 mgi.v.596 mgp.o.3012 mgp.o.2Diphenhydramine hydrochloride(First generation)30 mgp.o.2540 mgp.o.150 mgp.o.8Epinastine(Second generation)20 mgp.o.62Mequitadine(Second generation)3 mgp.o.3Levocetirizine hydrochloride(Second generation)2.5 mgp.o.15 mgp.o.9Hydroxyzine pamoate(First generation) andlevocetirizine hydrochloride(Second generation)25 mg5 mgp.o.11DEX: dexamethasone, HDC: hydrocortisone, PSL: prednisolone, mPSL: methylprednisolone
IRRs incidence according to the corticosteroid dose group and combinations of high-dose/low-dose corticosteroids and second-generation/first-generation antihistamines
The number of patients who had IRRs in the high-dose corticosteroid group was 41 (27.0%), which was significantly lower than that in the low-dose group [n = 31 (48.4%), p = 0.002] (Table 3). The severity of IRRs incidence in the high-dose group was grade 1 in 14 patients, grade 2 in 23 patients, and grade 3 in 4 patients, whereas, in the low-dose group, the severity of IRRs incidence was grade 1 in 8 patients, grade 2 in 20 patients, and grade 3 in 3 patients. Supplemental Table 1 shows the background of the 151 patients who received dexamethasone as premedication in the high- and low-dose corticosteroid groups. In the subgroup for the use of dexamethasone, the number of patients who had IRRs in the high- and low-dose groups was 26 (21.7%) and 10 (32.3%), respectively, with no significant difference (p = 0.22). The severity of IRRs in the high-dose group was grade 1 in 7 patients, grade 2 in 15 patients, and grade 3 in 4 patients. In the low-dose group, the severity of IRRs was grade 1 in 3 patients, grade 2 in 5 patients, and grade 3 in 2 patients. The number of patients who had IRRs in the High-dose corticosteroid/2nd generations histamine antagonists, High-dose corticosteroid/ 1st generations histamine antagonists, Low-dose corticosteroid/2nd generations histamine antagonists, and Low-dose corticosteroid/1st generations histamine antagonists was 11(14.7%), 27(40.3%), 2(50%), and 17(42.5%), respectively.
Table 3. Incidence of the infusion‑related reactions according to the dose of corticosteroid as premedicationIRRs (any grade), n (%)High dose (n = 152)Low dose (n = 64)p-value41 (27.0)31 (48.4)0.002Grade 011133-Grade 1148-Grade 22320-Grade 343-IRRs: infusion‑related reactions
Associated factors for the development of IRRs
Excluding 30 patients with missing values from 216 eligible patients, we explored associated factors for the incidence of IRRs in 186 patients (Fig. 1). Multivariable logistic regression analysis showed that first-generation histamine 1 receptor antagonist use as premedication [odds ratio (OR) = 3.31, 95% confidence interval (CI): 1.16–9.47; reference: second-generation histamine 1 receptor antagonist use], hydrocortisone use as premedication [OR = 7.21, 95% CI: 1.57–33.15; reference: dexamethasone], and methylprednisolone use as premedication [OR = 3.99, 95% CI: 1.13–14.10; reference: dexamethasone] were significantly associated with the incidence of IRRs during initial obinutuzumab administration (Table 4). Variance inflation factor (VIF) for the dosage and type of corticosteroids and the type of histamine antagonists was 1.048, 1.048, and 1.096, respectively. Low corticosteroid doses were not associated with the incidence of IRRs [OR = 0.84, 95% CI: 0.31–2.26] in the multivariable analysis. Prednisolone equivalent was not associated with the incidence of IRRs [OR = 0.99, 95% CI: 0.99–1.00] (Supplemental Table 2).
Table 4. Logistic regression analysisVariablesUnivariable analysisMultivariable analysisCategoryOR (95% CI)p-valuesOR (95% CI)p-valuesAnnArbor classification≥ Ⅲ3.04 (1.20–7.73)0.022.17 (0.75–6.30)0.15B symptoms+2.94 (1.31–6.59)0.011.37 (0.52–3.60)0.52sIL-2R (U/mL)-1.0 (1.0–1.0)0.351.0 (1.0–1.0)0.16LDH (U/L)-1.0 (0.99–1.0)0.251.0 (0.99–1.0)0.08Types of Antipyretic analgesicsAcetaminophenReference-Reference-NSAIDs0.82 (0.31–2.11)0.67Dosage of corticosteroidsLow dose2.10 (1.03–4.20)0.040.84 (0.31–2.26)0.73Types of corticosteroidsDEXReference-Reference-HDC6.88 (2.19–21.57)< 0.017.21 (1.57–33.15)0.013PSL4.01 (1.26–12.78)0.022.52 (0.66–9.65)0.18mPSL3.44 (1.20–9.88)0.023.99 (1.13–14.10)0.032Types of histamine antagonistsSecond generationsReference-Reference-First generations4.58 (2.06–10.19)< 0.013.31 (1.16–9.47)0.03First and second concomitant3.75 (0.91–15.41)0.072.38 (0.46–12.31)0.30sIL-2R: soluble interleukin-2 receptor, LDH: lactate dehydrogenase, NSAIDs: non-steroidal anti-inflammatory drug, DEX: dexamethasone, HDC: Hydrocortisone, PSL: prednisolone, mPSL: methylprednisolone
Discussion
Patients who received high-dose corticosteroids prior to obinutuzumab administration had a lower incidence rate of IRR compared to the low-dose corticosteroid group. However, the corticosteroid dose itself was not recognized as an independent risk factor. On the other hand, hydrocortisone or methylprednisolone and first-generation H1 antihistamines were identified as factors potentially influencing the incidence of obinutuzumab-induced IRR. Furthermore, the combination of high-dose corticosteroids and second-generation antihistamines was suggested to be associated with a lower incidence of IRRs. This study is the first to report findings regarding the dosage and type of corticosteroids and the type of antihistamines in the prevention of obinutuzumab-induced IRR.
The use of high-dose corticosteroids may be an effective preventive measure against IRR. The high-dose group in this study was defined based on FDA recommendations, suggesting that the use of sufficient corticosteroids as recommended dose is important for preventing IRRs. Studies have suggested that corticosteroids have a dose-dependent effect on IRRs prophylaxis and that intravenously administered dexamethasone has a dose-dependent effect on preventing IRRs in the case of trastuzumab administration [10]. Although the report targeted patients who received trastuzumab therapy, this report supports the dose-dependent effect of corticosteroids on IRRs. Moreover, although some patient backgrounds significantly differed between the high- and low-dose groups in this study, they were not identified as risk factors for IRRs incidence in a previous study including patients treated with rituximab [7–9]; therefore, it is likely that those factors did not affect the incidence of IRRs. Although high tumor volume and bone marrow involvement may be risk factor for IRRs incidence in patients receiving obinutuzumab [11, 12], no significant differences in sIL-2R or LDH and bone marrow involvement were observed between the two groups in this study. In addition, because aprepitant is known to inhibit CYP3A4 and may increase corticosteroid exposure, we examined its potential influence on corticosteroid dose classification. Among the 21 patients in the low-dose group who received concomitant aprepitant, no patient was considered to meet the high-dose definition based on the predefined corticosteroid potency assessment (data not shown); therefore, the potential impact of aprepitant on high-dose/low-dose classification was minimal. We also examined the proportion of patients receiving concomitant aprepitant in both the high-dose and low-dose groups and found no significant difference between the two groups (Table 1), suggesting that corticosteroid exposure was not systematically biased by aprepitant use. Therefore, the comparison of infusion-related reaction incidence between dose groups was unlikely to have been confounded by this pharmacokinetic interaction. The concomitant use of azole antifungals has been reported to potentiate the effects of corticosteroids [13]. In this study, a higher percentage of patients in the high-dose group received concomitant azole antifungals; although increased corticosteroid exposure may have contributed to the suppression of IRRs, the possibility that the use of concomitant azole antifungals contributed to the lower incidence of IRRs in the high-dose group cannot be ruled out.
On the other hand, being in the low-dose group was not identified as a risk factor for IRR occurrence (Table 4). Furthermore, prednisolone equivalent dose was not associated with IRR incidence (Supplementary Table 2). In this study, the comparison group was classified based on the dose and type of corticosteroid administered. To exclude the influence of corticosteroid type, a post-hoc analysis was performed in the subgroup of patients receiving dexamethasone, which had the largest number of cases. The results showed no difference in IRR incidence between the high-dose and low-dose groups. However, due to insufficient sample size, it was impossible to replicate equivalent incidence rates between high- and low-dose groups in the entire study population and detect a difference with sufficient statistical power; further research is needed. Furthermore, prednisolone equivalents may not accurately reflect antibody titers [6], and equivalents based on standardized conversion factors may not be significant covariates for IRR. Additionally, since premedication involved the combined use of corticosteroids, antipyretic analgesics, and antihistamines, factors other than the corticosteroid dosage were considered to potentially influence the outcome.
The use of hydrocortisone and methylprednisolone was shown to be associated with a higher incidence of infusion-related reactions (IRRs) compared with the use of dexamethasone. Furthermore, variance inflation factor values were assessed in the multivariable logistic regression analysis, and no multicollinearity was detected, supporting the robustness of these findings. Notably, no data are available in the FDA or EMA package inserts to support the use of hydrocortisone for reducing IRRs. Importantly, hydrocortisone is commonly administered intravenously at doses of 100–200 mg for the management or prevention of allergic or infusion-related reactions. Higher doses are generally reserved for severe or refractory cases [14, 15]. In the present study, 96.4% of patients receiving hydrocortisone were classified into the low-dose group when doses were converted to prednisolone-equivalent values, and high-dose hydrocortisone administration was uncommon. Therefore, the higher incidence of IRRs observed in patients receiving hydrocortisone may reflect limited prophylactic effectiveness under typical dosing conditions rather than an intrinsic adverse effect of hydrocortisone itself. In contrast, 91.3% of patients who received methylprednisolone were classified into the high-dose group after dose conversion, suggesting that differences in the pharmacological and pharmacokinetic profiles of each corticosteroid, in addition to dose, may have influenced the incidence of IRRs. Although dexamethasone is known to have a longer biological half-life than hydrocortisone or methylprednisolone [6], the mechanisms underlying its apparent efficacy in preventing IRRs require further investigation.
Hydrocortisone and methylprednisolone were identified as factors contributing to IRR occurrence, whereas prednisolone was not. This finding may be attributable to the fact that 64.3% (9/14) of patients who received prednisolone as premedication were administered the oral formulation. In addition to cytokine-induced infusion reactions, hypersensitivity reactions of an allergic nature are also known to occur following rituximab administration [16], accounting for approximately 5–10% of post-dose reactions [17, 18]. Because these reactions present with clinical features similar to IRRs, it is difficult to distinguish them in routine practice, and the outcomes collected in this study may include a mixture of these phenotypes. Succinate esters are known inducers of hypersensitivity [19], and injectable formulations of hydrocortisone, prednisolone, and methylprednisolone are manufactured as succinate esters due to their poor water solubility. Therefore, the use of these injectable corticosteroids may have contributed to an increased frequency of hypersensitivity reactions. However, the exact proportion of hypersensitivity as a phenotype of IRRs in this study remains unknown and warrants further investigation.
The administration of first-generation histamine 1 receptor antagonists was shown to be a possible factor for the incidence of IRRs. No studies have examined the effect of histamine 1 receptor antagonist on obinutuzumab-induced IRRs. A study comparing the histamine 1 receptor antagonists fexofenadine and bepotastine in terms of efficacy as IRRs countermeasures during the initial administration of rituximab reported that bepotastine significantly suppressed the incidence of IRRs compared with fexofenadine [20], suggesting that differences in pharmacokinetics and other aspects of histamine 1 receptor antagonists affect the incidence of IRRs. Studies investigating the preventive effect of diphenhydramine and cetirizine on IRRs in patients who received rituximab and other anticancer therapies have demonstrated that cetirizine may be a viable alternative for diphenhydramine in preventing IRRs [21]. A randomized controlled trial is ongoing to evaluate the efficacy of bepotastine besilate compared with hydroxyzine pamoate on IRR [22]. The first-generation H1-receptor antagonist d-Chlorpheniramine maleate administered in this study exhibited dose variability within the range of 2 to 12 mg, and it cannot be ruled out that it may have been insufficiently effective in cases involving low doses and oral administration. First-generation histamine 1 receptor antagonists are contraindicated in patients with prostatic hypertrophy and glaucoma, and their central nervous system depressant effects cause side effects, such as drowsiness and dizziness. Although the reasons why second-generation histamine 1 receptor antagonists are more effective as IRRs countermeasures than first-generation histamine 1 receptor antagonists have not been examined, it was considered desirable to use second-generation histamine 1 receptor antagonists, which have less anticholinergic and central nervous system depressant effects than first-generation histamine 1 receptor antagonists, from the perspective of side effects.
Premedication with obinutuzumab involves concomitant use of corticosteroids, antipyretic analgesics, and antihistamines, so we examined the effects of these combinations. Analgesics/antipyretics were not identified as factors affecting IRR (Table 4). Therefore, we further investigated the IRR incidence rate based on combinations of corticosteroid dosage and antihistamine generation. The results suggested that the combination of high-dose corticosteroids and second-generation antihistamines may be associated with a lower incidence of IRRs (Table 5). However, these findings should be interpreted cautiously and should not be taken as evidence that corticosteroid dose alone is protective.
Table 5. Incidence of IRR based on corticosteroid dosage and combination with histamine antagonistsIRR group (n = 57)No IRR group (n = 129)p-valueHigh-dose corticosteroid and 2nd generations histamine antagonists, n (%)11 (14.7)64 (85.3)< 0.01High-dose corticosteroidand1st generationshistamine antagonists, n (%)27 (40.3)40 (59.7)-Low-dose corticosteroidand2nd generationshistamine antagonists, n (%)2 (50.0)2 (50.0)Low-dose corticosteroidand1st generationshistamine antagonists, n (%)17 ( 42.5)23 (57.5)IRRs: infusion‑related reactions
Factors for the incidence of IRRs by rituximab have been reported to include high LDH and sIL-2R level, low hemoglobin level, presence of B symptoms and bone marrow infiltration, indolent lymphoma, and bulky disease [7–9]. High tumor volume may be risk factor for IRRs incidence in patients receiving obinutuzumab [11]. In this study, factors that could reflect tumor volume, such as staging, B symptoms, sIL-2R, and LDH, were examined but not identified as factors. The Groupe d’Etude des Lymphomes Folliculaires has developed criteria for predicting tumor volume in follicular lymphoma [23], which included B symptoms, but not sIL-2R or LDH. It was considered possible that the level of sIL-2R and LDH are unlikely to immediately reflect tumor volume because follicular lymphoma progresses slowly. We investigated the effect of the administration sequence of chemotherapy and obinutuzumab on IRR occurrence. The treatment schedule for chemotherapy combined with obinutuzumab is described as follows. Bendamustine is administered on days 1 and 2. CHOP therapy consists of cyclophosphamide, doxorubicin, and vincristine on day 1, followed by prednisolone/methylprednisolone on days 1–5. CVP therapy consists of cyclophosphamide and vincristine on day 1, with prednisolone/methylprednisolone administered on days 1–5. Obinutuzumab was administered before and after this combination chemotherapy. Since the administration sequence was considered a potential factor affecting infusion reaction occurrence, it was also investigated in this study; however, no effect was observed. (Data not shown)
This study has several limitations. This study was a retrospective survey, and collecting data using a uniform evaluation method for IRRs was impossible. In the GALLIUM study, the incidence of IRRs in the obinutuzumab and rituximab groups was 59% and 49%, respectively [1]. Other retrospective studies on IRRs caused by rituximab have reported IRRs incidence rates of 32.9% [7] and 37.9% [8] at the initial administration of rituximab. Two retrospective studies for IRRs caused by obinutuzumab have reported IRRs incidence rates of 36% [24] and 55.6% [12], at the time of initial obinutuzumab administration. The incidence of IRRs in this study was 33.3%, which is comparable to those reported in previous retrospective studies, although it differs from clinical trials in which precise evaluation can be performed. The possibility that IRRs may be underestimated in real-world data is an important limitation in this study. Furthermore, since the stepwise administration rate of obinutuzumab and the timing of premedication were not investigated, it cannot be ruled out that deviations from the recommended administration method may have influenced the occurrence of IRR.Logistic regression analysis was performed on 186 patients. The eight factors were selected as explanatory variables in the multivariable analysis with reference to clinical findings from previous reports. However, IRRs occurred in 57 patients, which may have reduced the reliability and robustness of the analysis. Bone marrow infiltration was not selected as an explanatory variable in the logistic regression analysis due to missing these examination data.
Conclusions
Dexamethasone may be more effective than hydrocortisone or methylprednisolone, and second-generation H1-antihistamines may be more effective than first-generation agents in preventing IRR, whereas corticosteroid dose alone was not. Specific combinations of premedications may influence the incidence of infusion reactions, but further investigation is needed.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Comprehensive Cancer Network Inc. NCCN clinical practices in oncology; B-cell lymphomas-verssion 2 [Internet]. 2024 [cited 2024 April 30]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf.
- 2Food & Drug Administration. Drugs @FDA: FDA-Approved Drugs. obinutuzumab drug label. November, 2013. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/125486 s 034lbl.pdf. Date accessed: July 17, 2024.
- 3European Medical Agency. Drugs @EMA: EMA-Approved Drugs. obinutuzumab drug label. July, 2014. Available from: https://www.ema.europa.eu/en/documents/product-information/gazyvaro-epar-product-information_en.pdf. Date accessed: July 17, 2024.
- 4Hayama T, Miura K, Uchiike A, Nakagawa M, Tsutsumi D, Sakagami M, et al. A clinical prediction model for infusion-related reactions to rituximab in patients with B cell lymphomas. Int J Clin Pharm. 2017;39:380-5.10.1007/s 11096-017-0429-328144804 · doi ↗ · pubmed ↗
- 5Tachi T, Yasuda M, Usui K, Umeda M, Nagaya K, Osawa T, et al. Risk factors for developing infusion reaction after rituximab administration in patients with B-cell non-Hodgkin’s lymphoma. Pharmazie. 2015;70:674–7.26601425 · pubmed ↗
- 6Post TW, editor. Glucocorticoid therapy: Pharmacology and principles of use. In: Up To Date, Waltham. MA: Up To Date Inc.; Available at: https://www.uptodate.com. Accessed [January 8, 2026].
- 7Anaphylaxis MA. Up To Date Inc. Available at: https://www.uptodate.com. Accessed [January 8, 2026].