Posterior Mitral Valve Acute Infective Endocarditis Complicated With Brain Abscess and Infection-Related Glomerulonephritis: A Case Report
Mikunthan Mithuriha, Raja Hettiarachchi, Thamotharam Balachandran

TL;DR
A woman with a heart infection caused by Staphylococcus aureus developed brain abscesses and kidney issues, but fully recovered after treatment with antibiotics and dental surgery.
Contribution
This case report highlights the rare systemic complications of infective endocarditis and the importance of multidisciplinary care.
Findings
The patient's infection led to cerebral abscesses and acute kidney injury.
Treatment with antibiotics and dental intervention led to full recovery.
Follow-up imaging showed resolution of heart and brain complications.
Abstract
We report the case of a 48-year-old previously unevaluated woman who presented with a short febrile illness with multi-organ involvement and was later diagnosed with acute methicillin-sensitive Staphylococcus aureus infective endocarditis of the posterior mitral valve. Her illness was complicated by septic embolization, leading to cerebral abscesses and infection-related glomerulonephritis, causing acute kidney injury. She had multiple septic teeth, which were thought to be the source of bacteremia. She was managed with multidisciplinary input involving cardiology, neurology, neurosurgery, microbiology, and oral maxillofacial surgery. Six weeks of intravenous antibiotics and removal of dental foci resulted in complete clinical and biochemical recovery. Follow-up transesophageal echocardiogram demonstrated resolution of the vegetation, and interval imaging showed a reduction in the size…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4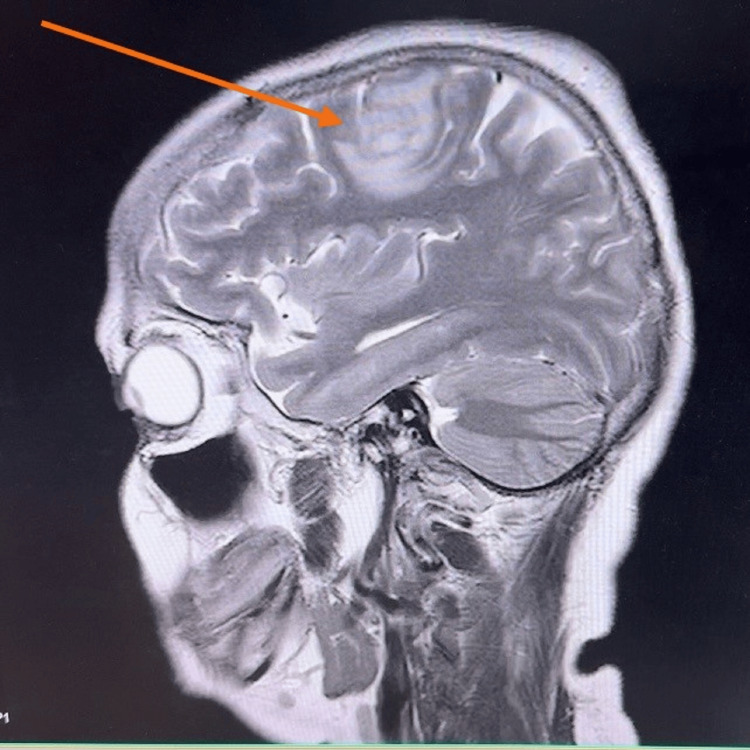 Figure 5
Figure 5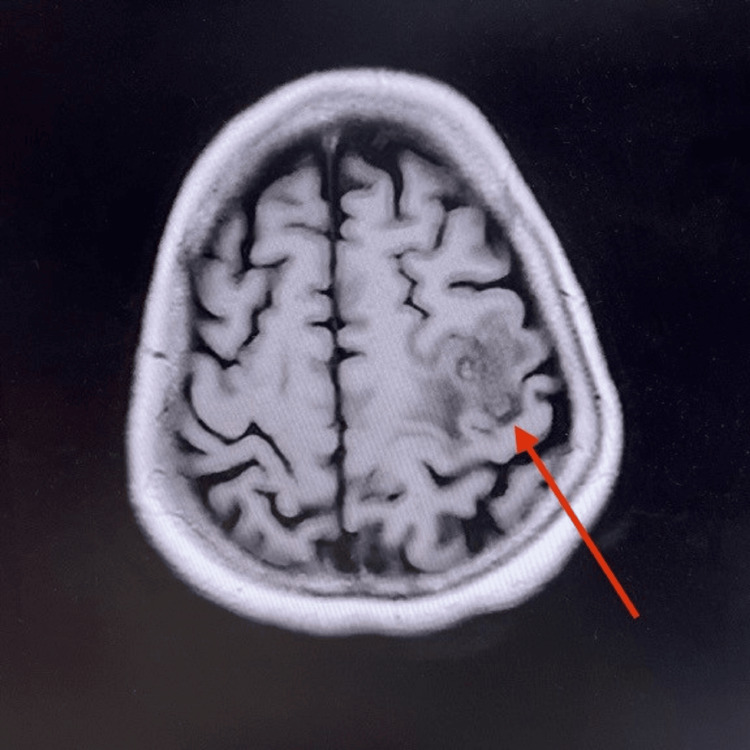 Figure 6
Figure 6| On admission | After treatment | Normal range | |
| Full blood count | |||
| White blood cells (109/L) | 17.64 | 9.7 | 4.0–11.0 |
| Neutrophils (109/L) | 14.14 | 6.3 | 2.0–7.0 |
| Lymphocytes (109/L) | 2.17 | 2.1 | 1.0–4.0 |
| Monocytes (109/L) | 1.02 | 1.0 | 0.2–0.8 |
| Eosinophils (109/L) | 0.09 | 0.1 | 0.02–0.4 |
| Basophils (109/L) | 0.22 | 0.2 | 0.01–0.1 |
| Hemoglobin (g/dL) | 9.5 | 11 | 12.0–15.5 |
| Platelets (109/L) | 155 | 250 | 150–450 |
| Blood picture | The blood picture shows normocytic normochromic anemia with evidence of ongoing severe bacterial infection. Thrombocytopenia could be due to infection. No evidence of MAHA | ||
| Erythrocyte sedimentation rate (mm/hour) | 115 | 40 | 0–20 |
| C-reactive protein (mg/dL) | 294 | 20 | <5 |
| Procalcitonin (ng/ml) | 47 | N/A | <0.1 |
| Serum creatinine (µmol/L) | 586 | 80 | 62–115 |
| Blood urea (mg/dL) | 184 | 10 | 7–20 |
| Aspartate aminotransferase (U/L) | 309 | 28 | 10–40 |
| Alanine aminotransferase (U/L) | 292 | 32 | 7–56 |
| Alkaline phosphatase (U/L) | 61 | 53 | 40–120 |
| Gamma-glutamyl transferase (U/L) | 25 | 21 | 10–60 |
| Serum albumin (g/dL) | 3.5 | 3.6 | 3.5–5.0 |
| Serum sodium (mmol/L) | 134 | 138 | 135–145 |
| Serum potassium (mmol/L) | 3.5 | 4 | 3.5–5.0 |
| Serum total calcium (mmol/L) | 1.8 | 1.9 | 2.1–2.6 |
| Serum magnesium (mmol/L) | 0.8 | 0.9 | 0.7–0.95 |
| Serum phosphate (mmol/L) | 1.8 | 1 | 0.8–1.5 |
| Electrocardiography | Sinus rhythm | ||
| Troponin I (ng/L) | 2,741 | 5 | <16 |
| Creatine phosphokinase (U/L) | 1,254 | 90 | 30–135 |
| Urine full report | |||
| Appearance | Clear | N/A | Clear |
| Pus cells (/HPF) | 99 | N/A | 0–5 |
| Red blood cells (/HPF) | 55 | N/A | 0–2 |
| Protein | Trace | N/A | Nil |
| Sugar | Negative | N/A | Negative |
| Fasting blood sugar (mg/dL) | 90 | N/A | 70–99 |
| Serum ferritin (ng/mL) | 2,200 | N/A | 15–150 |
| Blood/Urine/Stool cultures | Blood culture: MSSA isolated; other blood cultures negative/contaminated urine and stool culture negative | ||
| Cerebrospinal fluid analysis | |||
| Color | Colorless | N/A | Colorless |
| Protein (mg/dL) | 41 | N/A | 5–45 |
| Glucose (mg/dL) | 55 | N/A | 45–80 |
| Polymorphs (cells/µL) | 0 | N/A | 0 |
| Lymphocytes (cells/µL) | 5 | N/A | 0–5 |
| Red blood cells (cells/µL) | 330 | N/A | 0 |
| Adenosine deaminase (U/L) | 2 | N/A | 0.67–2.07 |
| CSF TB Gene-pert | Negative | N/A | Negative |
| Anti-nuclear Antibody | Negative | N/A | Negative |
| Anti-neutrophil cytoplasmic antibodies | Negative | N/A | Negative |
| Infective screening | |||
| Toxocariasis | Negative | N/A | Negative |
| Cryptococcal antigen | Negative | N/ A | Negative |
| Melioidosis antibody | Negative | N/A | Negative |
| Rickettsia serology: | Negative | N/A | Negative |
|
| Negative | N/A | Negative |
| Brucellosis Ab | Negative | N/A | Negative |
| Hepatitis B/C | Negative | N/A | Negative |
| Retroviral studies | Negative | N/A | Negative |
| Malaria | Negative | N/A | Negative |
| Investigations | Findings |
| Chest X-ray | Bilateral reticular nodular shadows; left lower zone opacity |
| High-resolution CT chest | Normal |
| Ultrasound abdomen | L/pyelonephritis |
| Non-contrast CT brain | Left frontal hypodense area noted |
| MRI brain |
Early cerebral abscess in the left frontal lobe; small lesion in the right temporal region (Figures |
| Transthoracic echocardiogram | 7 mm oscillating mass on the posterior mitral valve leaflet; mild mitral regurgitation |
| Transesophageal echocardiogram | Hyperechogenic oscillating lesion (0.7 × 0.5 cm) on the posterior mitral valve leaflet — vegetation |
| Follow-up transesophageal echocardiogram after treatment | No vegetations; normal mitral valve; no abscess |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Otolaryngology and Infectious Diseases · Cardiovascular and Diving-Related Complications
Introduction
Infective endocarditis (IE) is one of the life-threatening conditions associated with high morbidity and mortality due to systemic embolization and diffuse organ dysfunction [1]. Staphylococcus aureus is a common cause of acute IE and is frequently associated with rapid clinical deterioration and septic embolization, especially cerebral abscesses. Infection-related glomerulonephritis is also a recognized immune-mediated complication of IE, presenting with microscopic hematuria, proteinuria, and acute kidney injury. Early diagnosis, identification of the infectious source, and targeted antimicrobial therapy for the recommended duration are important management principles to prevent complications [2]. Here, we report a case of acute methicillin-sensitive Staphylococcus aureus (MSSA) IE of the posterior mitral valve, which was complicated by septic embolic (brain abscesses) and infection-related glomerulonephritis, successfully managed with patient-centered targeted medical therapy and a multidisciplinary team approach.
Case presentation
A 48-year-old previously healthy woman presented with a four-day history of high-grade intermittent fever with chills and rigors and watery loose stools with frequency of four to five times daily. There was no vomiting, abdominal pain, or blood/mucus in the stools. She also reported arthralgia, myalgia, generalized weakness, and mild headache. There was no cough, dyspnea, chest pain, urinary symptoms, recent travel, intravenous drug use, or muddy-water exposure. She was a non-smoker, non-alcoholic, and a housewife. On examination, she was febrile and pale with poor oral hygiene and multiple dental caries (Figure 1). Cutaneous stigmata suggestive of IE were present: splinter hemorrhages (Figure 2), painless palmar and plantar macules (Janeway lesion) (Figure 3), and painful digital pulp lesions (Osler’s node) (Figure 4). Cardiovascular examination revealed a regular pulse (80 beats/minute); however, there were no audible murmurs. Respiratory and abdominal examinations were normal. Neurological examination showed normal fundoscopy, mild generalized hypotonia, preserved reflexes, and power of 4/5 in all limbs. During the course of ward stay, she developed sudden-onset right upper limb weakness and right upper motor neuron facial nerve palsy for which she was further evaluated.
Poor oral hygiene with multiple septic teeth.
Splinter hemorrahges.
Painless plantar lesions (Janeway lesions).
Painful palmar pulp lesion (Osler’s nodes).
Table 1 summarizes the investigations of a patient with severe MSSA sepsis, characterized by neutrophilic leukocytosis, markedly elevated inflammatory markers, and complicated by acute kidney injury, transaminitis, rhabdomyolysis, and sepsis-related myocardial injury. Blood cultures grew MSSA, while extensive infective, autoimmune, and cerebrospinal fluid evaluations were negative. Following treatment, there was marked clinical and biochemical improvement with normalization of organ function, recovery of blood counts, and reduction of inflammatory markers.
Table 2 summarizes the imaging and procedural findings. Figure 5 and Figure 6 show coronal and sagittal contrast-enhanced MRI of the patient’s brain, demonstrating cerebral abscesses consistent with septic embolization.
Coronal section of the patient’s brain contrast MRI showing brain abscess in left frontal lobe (24 mm × 15 mm × 17 mm) (red arrow) and a further small area of early abscess formation in the right posterior temporal lobe.
Sagittal section of the patient’s brain contrast MRI showing brain abscess in left frontal lobe (24 mm × 15 mm × 17 mm) (red arrow) and a further small area of early abscess formation in the right posterior temporal lobe.
The likely source of MSSA bacteremia was identified as multiple septic teeth, which were removed by the Oral and Maxillofacial Surgery team. A multidisciplinary approach was adopted involving cardiology, neurology, microbiology, nephrology, and infectious diseases. She was given intravenous antibiotic therapy for six weeks via a central venous line. The neurosurgical team recommended purely medical management for the brain abscesses. Supportive management for renal impairment and electrolyte abnormalities was provided. No dialysis was required.
After six weeks of intravenous antibiotics, the patient became afebrile and clinically stable. Inflammatory markers and renal function progressively improved. Follow-up transesophageal echocardiogram showed complete resolution of vegetation. Repeat MRI demonstrated an interval reduction of abscess size. She was discharged with scheduled outpatient follow-up and remained clinically well at her two-week review, with improved appetite and no neurological symptoms.
Discussion
IE is an infection (acute or subacute) affecting the cardiac endothelium, mainly the heart valves. It has a high mortality rate, reaching up to one-third of the affected patients. Early disease recognition and proper early treatment are essential to prevent the disease-related complications and mortality [1]. There is a wide range of infectious etiologies causing IE. Poor oral hygiene and multiple infected teeth likely served as the portal of entry in this case, consistent with the well-established association between dental sepsis and left-sided endocarditis.
IE caused by S. aureus remains one of the most aggressive forms of bacterial endocardial infection and is frequently associated with multisystem complications. MSSA IE typically presents with a rapid onset of high-grade fever and systemic inflammatory manifestations. In this patient, classical peripheral stigmata, including splinter hemorrhage, Janeway lesions, and Osler’s nodes, were prominent, supporting an embolic and immunological component of the disease. Our patient fulfilled the modified Duke criteria, which is currently widely used for clinical diagnosis of IE with clinical, laboratory, and echocardiographic findings [2].
According to studies, the risk of septic embolization in IE depends on several factors, including the vegetation’s size, motility of the vegetation, location on the mitral valve, and staphylococcal bacteremia [3]. IE associated with a central nervous system event is one of the common complications and is associated with high mortality and an important factor determining prognosis [4]. Neurological complications occur in approximately 20-40% of S. aureus IE cases, with stroke being the most common. Patients can also develop transient ischemic attack due to vaso-occlusion, cerebral abscesses, mycotic aneurysms, and intracranial and subarachnoid hemorrhages as neurological complications [5]. Brain abscess is more frequently a feature of acute endocarditis than subacute endocarditis. The abscesses may be single or multiple, and their clinical presentation may be that of a space-occupying lesion, encephalopathy, or with features of meningitis [6]. Our patient demonstrated two abscesses in the frontal and temporal regions, an expected distribution given hematogenous spread. MRI remains the most sensitive modality for identifying early abscess formation, where brain abscesses are seen as multiple ring-enhancing lesions at the gray-white matter junction.
Glomerulonephritis associated with IE can result from multiple mechanisms, including drug toxicity, septic emboli, or immune-complex glomerulonephritis. It has a broad spectrum and is relatively rare, especially in cases with no previous heart disease [7]. The patient’s acute kidney injury, accompanied by proteinuria and microscopic hematuria, aligned most closely with infection-related glomerulonephritis. This is consistent with elevated inflammatory markers, presence of a high systemic bacterial load, and the absence of features suggestive of primary vasculitis or direct septic embolization. S. aureus-associated infection-related glomerulonephritis is increasingly recognized and may present with severe but reversible renal dysfunction, as demonstrated by gradual improvement following withdrawal of nephrotoxic agents and infection control.
This patient was managed by a multidisciplinary team comprising cardiology, neurology, neurosurgery, microbiology, nephrology, and oral maxillofacial surgery, as recommended by the latest guidelines that emphasize coordinated care for complex IE presentations. The duration of intravenous antibiotics is six to eight weeks, along with serial monitoring of clinical and biochemical parameters and serial imaging to assess the size of the cerebral abscess and vegetation in the heart to guide the treatment.
Conclusions
Overall, this case emphasizes the classical yet challenging natural history of S. aureus IE with multisystem involvement, as in our case, cerebral abscesses and infection-related glomerulonephritis. It reinforces the importance of early recognition of peripheral stigmata, the role of thorough multisystem evaluation, actively looking for the infectious source, and the importance of serial imaging and laboratory monitoring. It also highlights that severe complications, such as cerebral abscesses and infection-related glomerulonephritis, can be treated successfully with timely diagnosis and targeted antimicrobial therapy with multidisciplinary management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Infective endocarditis and septic emboli: diagnostic delays, implications, and challenges Cureus Ibnian AM Vincent ME Amadi J 017202510.7759/cureus.83117 PMC 1211759240438856 · doi ↗ · pubmed ↗
- 2Infective endocarditis: a case with prolonged fever Cardiovasc Cardiometabolic J Prismadani M Subagjo A 8422021 https://e-journal.unair.ac.id/CCJ
- 3Infective endocarditis complicated by cerebral abscess and mycotic intracranial aneurysm: a case report Radiol Case Rep Musthafa I Kandel D Rajlawot K Neupane NP Sitaula A 36903693172022 https://doi.org/10.1016/j.radcr.2022.06.0683594226810.1016/j.radcr.2022.06.068PMC 9356087 · doi ↗ · pubmed ↗
- 4Infective endocarditis complicated by brain embolism: a case report Cor Vasa Snopek P Hasilla J PatrovičL JuskaničD Benko J SamošM 545549652023
- 5Mitral valve endocarditis presenting as a stroke in a young lady: a case report J Clin Images Med Case Rep Kumari Perera MNS 270942023 http://www.doi.org/10.52768/2766-7820/2709
- 6An infective endocarditis complicated by multiple septic emboli: case report Egypt Heart J Amri M Tamir EM Drighil A Habbal R 19762024 https://doi.org/10.1186/s 43044-024-00451-z 3834017910.1186/s 43044-024-00451-z PMC 10858854 · doi ↗ · pubmed ↗
- 7Successful treatment of infectious endocarditis associated glomerulonephritis mimicking c 3 glomerulonephritis in a case with no previous cardiac disease Case Rep Nephrol Kawamorita Y Fujigaki Y Imase A 56904720142014 https://doi.org/10.1155/2014/5690472550644510.1155/2014/569047 PMC 4259083 · doi ↗ · pubmed ↗