A novel fasting mimetic (Mimio) creates fasting-like benefits to hunger control, oxidative stress, and cardiometabolic health in humans
Azure D. Grant, Marie Crisel B. Erfe, Armenouhi Kazaryan, Paige L. Oliver, Jordan Moos, Veronica Luna, Noah Craft, Christopher H. Rhodes

TL;DR
A new supplement called Mimio mimics fasting benefits, reducing hunger and improving heart and metabolic health in overweight older adults without requiring them to fast.
Contribution
This is the first study to show a fasting mimetic supplement can recreate clinical fasting benefits without lifestyle changes or actual fasting.
Findings
Mimio improved hunger and satiety metrics more than placebo in overweight older adults.
Mimio reduced cholesterol, LDL, oxidized LDL, and fasting glucose compared to placebo.
Mimio caused fewer digestive symptoms and no significant adverse effects compared to placebo.
Abstract
This decentralized, double-blind, randomized, placebo-controlled trial investigated the impact of a novel fasting mimetic “Mimio” on hunger, satiety, digestive symptoms, metabolism, cognition and wellbeing in overweight older adults with elevated HbA1c. Participants collected 2 weeks of baseline subjective data along with a fasted metabolic blood panel. The Mimio fasting mimetic, containing spermidine, nicotinamide, palmitoylethanolamide (PEA) and oleoethanolamide (OEA), or a placebo capsule was then taken before the first meal of the day for 8 weeks. Subjective measures were repeatedly collected throughout the study and metabolic bloodwork was repeated at the end of 8 weeks. 42 Participants were evaluated (47.6% female, BMI 27.6 (0.2) kg/m2, aged 62 ± 4, HbA1c 6.0 ± 0.1, n = 23 intervention and n = 19 placebo). Mimio improved more over time in all hunger and satiety metrics than…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
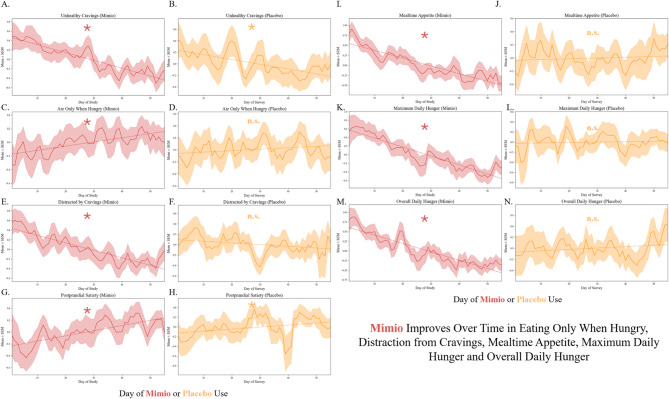 Figure 1
Figure 1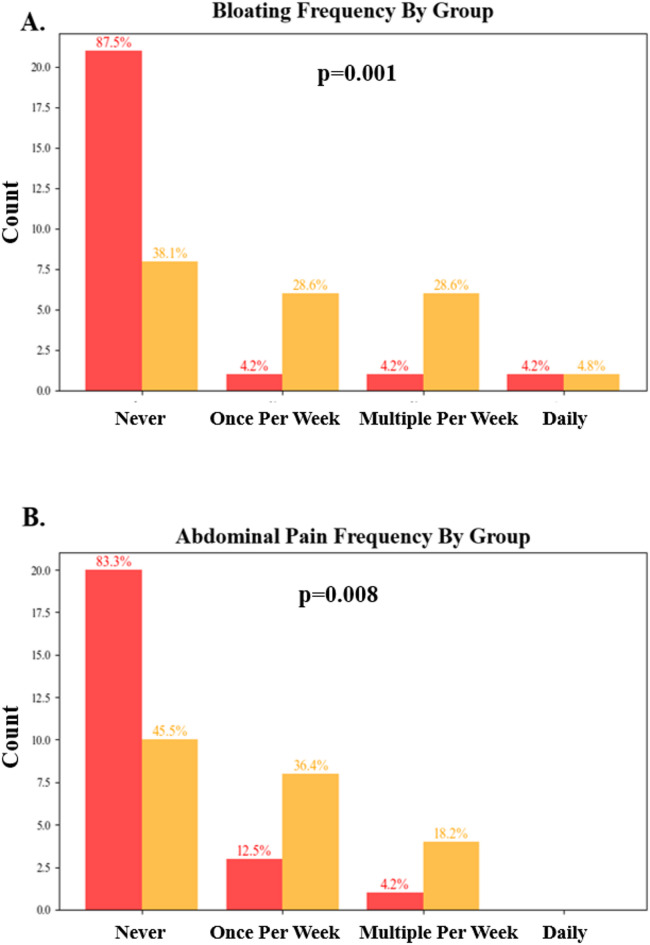 Figure 2
Figure 2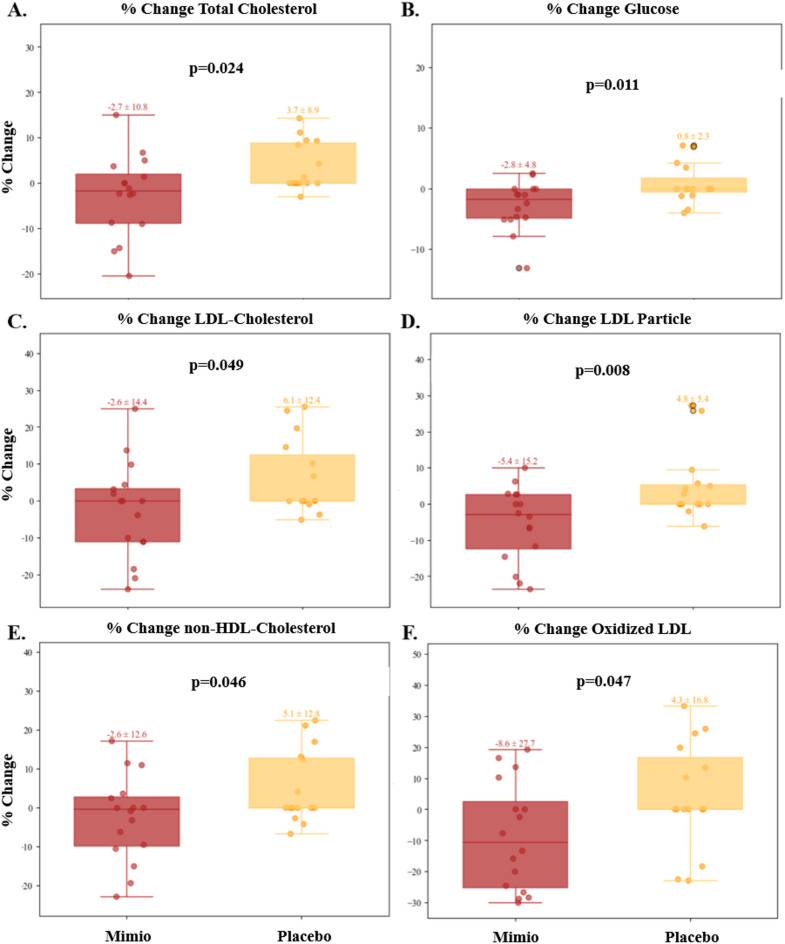 Figure 3
Figure 3- —Mimio Health, LLC
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDietary Effects on Health · Diet and metabolism studies · Genetics, Aging, and Longevity in Model Organisms
Introduction
Intermittent fasting has gained significant scientific and clinical interest in recent years due to its well-documented beneficial effects on conditions ranging from cardiovascular disease to metabolic disorders, neurodegenerative conditions, cancer and autoimmune disease^1–10^. Moreover, prolonged periods of fasting remain one of the only reliable methods of extending lifespan in model organisms due their direct modulation of the cellular aging process^1–4^. Unfortunately, fasting’s long term impracticality and safety concerns limit its widespread adoption. Despite its potential to significantly improve human health by helping to treat, prevent, or delay disease and enhance longevity, the duration of fasting required to achieve such benefits (typically greater than 24 h)^1^ is a significant burden to quality of life. Moreover, this fasting duration is often infeasible or dangerous for numerous populations, including adolescents^11^, endurance athletes^12^, lean or underweight young people^13^, the elderly, those with a history of eating disorders and pregnant or breast-feeding women^11^. Interventions capable of mimicking the beneficial cellular, metabolic, immune, and longevity-enhancing effects of fasting without the need to abstain from food hold great potential therapeutic value for both the treatment and prevention of chronic health conditions, especially for those for whom fasting may be contraindicated.
Spermidine, nicotinamide, palmitoylethanolamide (PEA) and oleoylethanolamide (OEA) are endogenous human metabolites that appear to improve clinical markers of disease, extend lifespan and possess anti-inflammatory and antioxidant properties^14–17^. Each of these molecules is both an endogenously produced human metabolite and a common food constituent of plant and animal products (fruits, vegetables, meats, grains, etc.)^18–21^. Spermidine’s beneficial effect on longevity is thought to be mediated through multiple mechanisms including the induction of systemic autophagic processes^18–20^, modulation of inflammation, lipid metabolism, cell growth and proliferation^19,21–23^. Once thought to be a mere inert product of B vitamin metabolism, 1-MNA has recently gained attention as a bioactive metabolite with vasoprotective, anti-inflammatory, antioxidant and antithrombotic effects mediated through its role in COX-2 inhibition^24–26^. 1-MNA has also been shown to extend lifespan in C. elegans through the induction of cellular antioxidant mechanisms^27^. Since its discovery in 1957, PEA has been widely used as an anti-inflammatory and analgesic via modulation of the immune system, neuronal cells and the endocannabinoid system^28–33^. PEA is also documented to have potential benefits in treating neurodegenerative and CNS disorders^28^ such as Alzheimer’s disease^34^, depression^35^ and fibromyalgia^36^. Similar to spermidine and 1-MNA, PEA can extend lifespan by combatting inflammation in mouse models^37^. Finally, OEA’s primary action is as a proliferator-activated receptor-α (PPAR-α) agonist^38^ through which it regulates energy intake, energy expenditure and hunger signaling to increase satiety and decrease food intake^38,39^. For this purpose, dietary supplements containing OEA are primarily used for weight loss^40^. However, OEA has also accumulated recent evidence of immunomodulatory activity, inducing systemic anti-inflammatory and antioxidant effects through currently unknown mechanisms^41–43^. Recent experiments by this lab have also shown OEA to be able to significantly extend the lifespan of C. elegans^44^.
A previous study conducted by the Zivkovic Lab at the University of California, Davis identified higher plasma concentrations of these metabolites after a 36 h fast compared to a 12 h overnight fast and demonstrated that a combination of spermidine, 1-methlynicotinamide (1-MNA, a cellular derivative of nicotinamide), PEA and OEA could mimic many of the functional benefits of prolonged fasting including significant anti-inflammatory and antioxidant effects in vitro and extending lifespan by 96% in C. elegans^44^. This fasting mimetic formulation has also been shown in a pilot clinical study to be orally bioavailable, well-tolerated, and capable of replicating anti-inflammatory, antioxidant and cardioprotective effects similar to fasting when taken in the postprandial state^45^.
The present study investigated the impacts of this novel fasting mimetic formulation (Mimio Biomimetic Cell Care, “Mimio”) on subjective and objective measures of metabolic and digestive health in overweight adults with elevated hemoglobin A1c (HbA1c) in a randomized, double-blind, placebo-controlled setting. Subjective measures of hunger and satiety, gastrointestinal symptoms, cognitive failures and quality of life were administered. Additionally, blood samples for measurement of NMR lipoprofile, oxidized LDL, hsCRP, HbA1c, insulin and plasma glucose were collected before and after intervention.
Methods
Eligibility
Participants needed to be at least 55 years of age, have a BMI between 25 and 29.9 and an HbA1c level of at least 6.0%. Female participants were required to be menopausal (> 12 months since last menstrual period) and to not use exogenous hormones. If taking any fiber supplements, prescription medication for cholesterol (e.g., statins) or other class of medications for metabolic disorders such as metformin, ACE inhibitors, beta blockers, rapamycin, thiazolidinediones, etc., participants were required to maintain a stable dose for at least 4 weeks prior to randomization and throughout the course of the study.
If taking any other supplement products such as fish oil, resveratrol, alpha-ketoglutarate, berberine, ashwagandha, pre- and probiotics, melatonin, NAD+ precursors (e.g., niacin, nicotinamide riboside (NR), nicotinamide mononucleotide (NMN), NADH), fisetin, astaxanthin, urolithin-A, CoQ-10, green tea extract/EGG, or pterostilbene, participants were required to stop from at least 1 week prior to randomization through the end of the study. Participants were required to abstain from cannabis products and maintain a consistent diet throughout the study.
Participants could not be taking any GLP-1 agonists or incretin mimetics, any investigational therapies, or be regular users of over-the-counter allergy or pain medications (i.e., > 3–4 times per week). Participants could not be diagnosed with diabetes, eating disorders, any substance abuse, anemia, cardiovascular disease (CVD), or cancer. Finally, participants could not have any known hypersensitivity or previous allergic reaction to nicotinamide, PEA, OEA, or spermidine.
Participants needed to be able to read and understand English, use a personal smartphone device and download the mobile application Chloe by People Science, receive shipment of the product at an address within the United States and be willing travel to a local Quest Diagnostics laboratory (Quest Diagnostics, Secaucus, NJ, USA) for fasted blood sample collection twice during the course of the study.
Study design
Participants completed up to a 14-week study consisting of a screening period, randomization and shipping period, a 2-week baseline period and an 8-week product or placebo use period. A schedule of all study activities is provided in Table 1.
Participants were randomized to one of 2 groups by AK: Mimio capsules or matching placebo capsules, with stratification to ensure even balance of male and female participants in each group. The investigators, study team and participants were blinded to the group assignment. Participants received the study product and study supplies after randomization. Demographic, medical history and concomitant medications data were collected during the screening period in Chloe. All assessments and surveys were administered in the Chloe mobile app. Blood sample collection occurred at the participant’s local Quest laboratory. Adverse events were both actively, via a weekly prompt, and passively collected throughout the study.
Recruitment, consent, and compensation
Participants who had never tried Mimio were recruited through the People Science community and social media channels. Virtual electronic informed consent, including a study-specific privacy authorization and the California Experimental Subject’s Bill of Rights (as applicable) were provided through Chloe. A digital copy of the signed consent was accessible by the participant through their Chloe profile. Eligible participants who provided virtual electronic consent were enrolled into the study. Participants received a $150 gift card upon study completion.
Mimio supplement and placebo dosing and adherence
Each dose of Mimio, to be taken 30–60 min before the first major meal of the day, contained Nicotinamide (250 mg), Ultra-Micronized Palmitoylethanolamide (600 mg), Oleoylethanolamide (400 mg), Spermidine (8 mg); Hydroxypropyl-Methylcellulose (capsule), Silicon Dioxide and Magnesium Stearate. The placebo capsules contained Micro Crystalline Cellulose (250 mg), Hypromellose and Titanium Dioxide. Participants were asked to confirm the time and number of capsules taken daily in the Chloe mobile application.
Study platform
All study tasks, communication and data were collected and assembled via the web and mobile-app based data collection platform, the Consumer Health Learning and Organizing Ecosystem (Chloe) by People Science (People Science Inc., Los Angeles, CA, USA). Hence, participants were able to collect data from their homes or on the go. All data was securely stored on People Science Amazon Web Services HIPAA-compliant servers. The Chloe platform contains modules for building and managing surveys, landing pages, marketing outreach with tracking tools for recruitment, audited electronic consent forms and electronic case report forms (eCRF), data management and analytics using an integrated relational database. Data from completed assessments was automatically collected for analysis. Study monitoring was conducted using reporting features.
Subjective measures
The study’s primary outcome was a daily Hunger, Satiety and Cravings Scale consisting of 7 items on a 0–5 scale (strongly disagree to strongly agree). Questions pertained to hunger, appetite, cravings and satiety in the past 24 h (e.g., “yesterday I craved foods I think of as unhealthy,” “yesterday I felt satisfied after my meals, neither too full nor hungry”). This daily survey began at baseline and was administered throughout the product/placebo use period. Digestive symptoms and quality of life were evaluated using a weekly survey. The weekly survey consisted of a 13-item set of Likert scales relating to sleep, stress, mood, energy, food noise and gastrointestinal symptoms (i.e., flatulence, bloating, abdominal discomfort, nausea and bowel movement regularity). The cognitive aspect of eating behavior was evaluated using weekly repetitions of the Three-Factor Eating Questionnaire (TFEQ-18). The TFEQ-18 is a validated, 18-item questionnaire representing the derived factors of Cognitive Restraint, Uncontrolled Eating and Emotional Eating^46^. See Supplemental Table 1 for schedule of assessments.
As fasting may be associated with cognitive function^47^, The Cognitive Failures Questionnaire (CFQ) was administered at baseline and weekly across the product and placebo use period. The CFQ is designed to assess a person’s self-rated proneness to committing cognitive slips and errors of perception, memory, motor functioning and absent-mindedness in the completion of everyday tasks^48,49^. Finally, to further evaluate product safety, participants were asked about any negative experiences at the end of each week and filled out a study experience survey after protocol completion.
Blood measures
Blood was drawn after at least an 8 h overnight fast at baseline and end of study for evaluation of the following markers: plasma glucose (mg/dL), insulin (uIU/mL), hemoglobin A1c (HbA1c, % of total hemoglobin), hs-CRP (mg/L), triglycerides (mg/dL), total cholesterol (mg/dL), HDL cholesterol (HDL-c, mg/dL), calculated LDL cholesterol (LDL-c, mg/dL), total cholesterol/HDL-c ratio, calculated non-HDL Cholesterol (mg/dL) and triglyceride/HDL-c ratio. An NMR lipid profile provided the following additional lipid markers: LDL particle concentration (LDL-p, nmol/L), small LDL-p concentration (nmol/L), LDL size (nm), HDL particle concentration (HDL-p, µmol/L), large HDL-p concentration (µmol/L), HDL size (nm), large VLDL particle concentration (VLDL-p, nmol/L), VLDL size (nm) and oxidized LDL (OxLDL, U/L). Samples were collected and analyzed by Quest Diagnostics. Participants were asked directly if they fasted at each blood sample. Data from participants who replied “no” were excluded. Additionally, participants were asked to complete their end of study blood draws within one week of study completion. Data points from participants who completed blood collection outside this window (e.g., 9 days after study completion) were omitted.
Sample, data evaluability and statistics
Sample size was determined based on estimated change in the Hunger and Satiety scale. Data analysis was conducted in Python (version 3.9.13) Jupyter Notebooks (Jupyter LLC, NYC, NY, USA). Participants were considered evaluable for analysis if they completed 8 weeks of Mimio/placebo use, baseline measurements and at least 70% of their questionnaires. Missing data in daily surveys were linearly interpolated and individual days in which a dose of Mimio was missed were omitted. Data were tested for normality using the Shapiro-Wilk test.
The primary objective of this study was to evaluate the impact of Mimio on a daily scale of hunger & satiety. We aggregated individual changes in the survey from the baseline period to week 8 and compared placebo and Mimio groups using parametric statistics (t-tests or repeated measures ANOVA (rmANOVA). Mixed effects models were used to evaluate impact of demographic factors. Daily data were evaluated both on change in absolute scores and by within-individual change in scores via Mann-Kendall (MK) trend over time. Difference in percentage improvers assessed by Fisher’s Exact Tests (FET).
Secondary objectives, including change in bloodwork, cognitive failures questionnaire (CFQ), cognitive and behavioral components of eating (TFEQ-18) and change in self-reported sleep, stress, mood, energy, pain and gastrointestinal symptoms (i.e., flatulence, bloating, abdominal discomfort, stool consistency/ regularity, constipation), were evaluated using absolute before and after scores, by comparing within-individual magnitude and direction of change and proportion of individuals who improved in each group. FET was used to evaluate differences in the occurrence of categorical variables in the weekly wellness and digestive health surveys.
AEs were summarized by group, displaying number of participants in each group, severity, possible relation to the study intervention and resolution.
Results
Recruitment and conduct
This study was approved by the Advarra Institutional Review Board (Pro00080269) and registered with clinicaltrials.gov (NCT06790407, 4/25/2024). All participants gave informed consent. All study procedures were conducted by People Science following Good Clinical Practice (GCP) guidelines and in accordance with the ethical principles of the Declaration of Helsinki and its amendments. Recruitment occurred 7/29/2024-10/7/2024. The trial concluded after recruited participants completed study activities. The full protocol can be accessed at clinicaltrials.gov.
Demographics
A total of 42 individuals were included (Mimio n = 23, Placebo n = 19) for all primary and secondary outcomes except blood work, with an intervention adherence rate of 94%. A total of 33 participants were evaluated for blood markers with 9 participants being excluded based on violations to protocol compliance including failure to fast during blood draws or to complete bloodwork within a week of study completion. The mean age (SEM) was 62 ± 4 years. BMI mean (SEM) was overweight but not obese, 27.7 ± 0.16. The mean HbA1c level was 6.0 ± 0.1%. Sex, age, ethnicity, and BMI did not differ by group. Fasting bloodwork values did not differ statistically for any metric at baseline between the Mimio and placebo groups. Demographics are described in Table 1. Laboratory values at baseline are presented in Table 2 and Supplemental Figure 1.
Table 1. Demographics.CategoryTotal % (count)Mimio % (count)Placebo % (count)P-value Sex Female47.6 (20)47.8 (11)47.4 (9)p > 0.05Male52.4 (22)52.2 (12)52.6 (10)p > 0.05 Mean age (STD) in years 62 (4)62 (4)63 (4)p > 0.05 Ethnicity Caucasian81 (34)87.0 (20)73.7 (14)p > 0.05Hispanic4.8 (2)0 (0)10.5 (2)p > 0.05Asian7.1 (3)8.7 (2)5.3 (1)p > 0.05African American4.8 (2)0 (0)10.5 (2)p > 0.05Other2.3 (1)4.3 (1)0 (0)p > 0.05Body mass index (BMI,** kg/m²)**27.6 (0.24)27.7 (0.32)27.5 (0.38)p > 0.05
Table 2. Baseline metabolic values.Blood metric (units)Laboratory value mimio mean (SEM)Laboratory value placebo mean (SEM)P-valueCholesterol/HDL-c (ratio)3.50 ± 0.203.90 ± 0.20p > 0.05Cholesterol, total (mg/dL)187.2 ± 11.3191.6 ± 9.50p > 0.05Glucose, plasma (mg/dL)90.7 ± 2.2087.5 ± 1.50p > 0.05HDL-c (mg/dL)55.1 ± 3.2051.6 ± 3.60p > 0.05HDL-p (µmol/L)36.4 ± 1.3036.7 ± 1.60p > 0.05HDL size (nm)8.70 ± 0.108.60 ± 0.10p > 0.05HbA1c (%)6.10 ± 0.105.90 ± 0.10p > 0.05Hs-CRP2.60 ± 0.704.40 ± 1.40p > 0.05Insulin12.5 ± 1.707.80 ± 0.90p > 0.05LDL-c (calculated, mg/dL)110.0 ± 9.50120 ± 7.10p > 0.05LDL-p (nmol/L)1650 ± 1011772 ± 64.0p > 0.05LDL Size (nm)20.9 ± 0.1020.9 ± 0.2p > 0.05Large HDL-p (µmol/L)4.90 ± 0.703.70 ± 0.40p > 0.05VLDL-p (nmol/L)3.00 ± 0.402.60 ± 0.60p > 0.05Non-HDL-c (calculated, mg/dL)132 ± 10.2149 ± 5.60p > 0.05Ox-LDL (U/L)48.1 ± 3.9048.4 ± 5.20p > 0.05Small LDL-p (nmol/L)655 ± 48.8687 ± 55.0p > 0.05TG/HDL-c (ratio)2.40 ± 0.302.10 ± 0.20p > 0.05Triglycerides (mg/dL)121 ± 11.2112 ± 7.50p > 0.05VLDL Size (nm)47.6 ± 0.6046.4 ± 0.70p > 0.05
Daily hunger and satiety survey
The composite metric of the daily hunger and satiety survey decreased (improved) uniquely in Mimio (MK p = 2.210^− 16^), MK p > 0.05 in placebo indicating no trend (Fig. 1, Supplemental Table 2). No monotonic trends were observed in placebo in any marker but unhealthy cravings, whereas Mimio exhibited a statistically significant monotonic trend in the direction of subjective improvement in all other aspects of hunger and satiety (MK p < 810^− 3^ for all) (Fig. 1, Supplemental Table 2). More participants in the Mimio group improved daily ratings of hunger and appetite compared to placebo, including 91% vs. 47% of participants improving mealtime appetite across the study (Fisher’s Exact Test p = 0.003). For percent improvers by subcomponent of the Hunger & Satiety scale see Supplemental Table 3.
Fig. 1. Mimio is uniquely associated with eating when hungry, reduced cravings, lower mealtime appetite and less hunger. People taking Mimio (red, left columns) exhibited a statistically significant Mann-Kendall trend over time to improvement unhealthy cravings (A,B), eating only when hungry (C,D), distraction from cravings (E,F), postprandial satiety (G,H), mealtime appetite (I,J), maximum daily hunger (K,L) and overall daily hunger (M,N) (MK trend over time p < 0.05). The placebo group (yellow, right columns) statistically improved only unhealthy cravings (B) and postprandial satiety (H) (MK trend over time p < 0.05).
Weekly digestive symptom and wellness survey
Weekly measures did not differ statistically at baseline (Student’s t-tests p > 0.05). Frequency of bloating was reduced by the final week of the study (Student’s t-test p = 0.001), with 87.5.6% vs. 38.1% of participants reporting no bloating in the final week (Fig. 2A). Additionally, abdominal pain frequency was reduced (Student’s t-test p = 0.008), with 83.3% vs. 45.5% of participants reporting never (Fig. 2B). Other digestive metrics trended toward improvement with Mimio (Supplemental Fig. 2). Weekly metrics of self-reported sleep duration, quality, anxiety, contentedness, low mood, food noise, stress and energy did not differ by group (Supplemental Fig. 3).
Fig. 2. Mimio reduced frequency of bloating and abdominal pain compared to placebo. Mimio (red) reduced the frequency of bloating (A) and abdominal pain (B) compared to placebo (yellow). Data represent the final week of the study. Percentages indicate the proportion of that cohort that gave a given answer (e.g., 87.5% of Mimio participants “Never” experienced bloating in the final week of the study, vs. 38.1% of placebo participants). The y-axis of the histogram represents the count of individuals.
Metabolic bloodwork
Blood work analysis revealed several significant improvements in cardiometabolic risk factors and oxidative stress markers in the Mimio group compared to the placebo, including reductions in total cholesterol, fasting glucose, LDL cholesterol, LDL particle number, non-HDL cholesterol, and Oxidized LDL (Fig. 3). Of these, the most substantial were a 5.4% drop in LDL-p with Mimio vs. a 4.8% rise in placebo (student’s t-test p = 0.008; net change vs. placebo 10.2%) and an 8.6% drop in Oxidized LDL with Mimio vs. a 4.3% rise in placebo (student’s t-test p = 0.047; net change vs. placebo 12.9%). Statistical trends evaluated by raw change per metric and % within-individual change per metric were consistent across all metrics. There was no statistically significant change across other blood measures between the placebo and Mimio groups including insulin, CRP, HDL-c, HbA1c, or triglycerides. Complete values for each blood metric can be found before and after in Supplemental Fig. 1. Groups did not differ at baseline in values (Table 2) or proportion of cohorts “In Range” (data not shown).
Fig. 3. Mimio improved cardiometabolic and oxidative stress markers compared to placebo. Mimio was associated with a reduction in total cholesterol (A), glucose (B), LDL-c (C ), LDL-p (D), Non-HDL-c (E), and oxidized LDL (F). Mimio is shown in red, placebo in yellow. Values above box and whisker plots represent mean ± SEM of % change from baseline to end of study. Scattered dots represent individual participants’ values. P-values are displayed on each plot.
Adverse events
Adverse event rates did not differ statistically between the Mimio and placebo groups. Only 1 AE, a case of mild diarrhea, occurred during product use in the Mimio group and was considered possibly attributable to the intervention. By comparison, 5 digestive AEs occurred in the Placebo group. See Supplemental Table 4.
Three factor eating questionnaire (TFEQ-18)
Mimio and Placebo groups did not differ in any TFEQ sub score: Cognitive Restraint, Uncontrolled Eating or Emotional Eating. Starting and ending values for each sub score are shown by group in Table 3 and graphed in Supplemental Fig. 4–5. Within-individual change from baseline to end of product use and did not vary by group (Mann-Kendall and rm-ANOVA p > 0.05 for all subscales). Percent improvers did not vary by group (FET p > 0.05 for all subscales, data not shown).
Table 3TFEQ-18 scores.Sub scoreMimio startMimio endPlacebo startPlacebo endCognitive restraint2.47 ± 0.122.22 ± 0.132.56 ± 0.132.41 ± 0.15Uncontrolled eating2.65 ± 0.082.70 ± 0.102.63 ± 0.122.63 ± 0.15Emotional eating2.38 ± 0.112.00 ± 0.102.33 ± 0.142.01 ± 0.13
Cognitive failures questionnaire
CFQ scores did not differ at any time point for the two groups and did not differ between males and females (p > 0.05). CFQ score trended downward significantly in both groups, from 33.4 ± 3.13 to 23.5 ± 2.71 (Mann-Kendall p = 910^− 4^) in Mimio and from 34.7 ± 2.56 to 23.75 ± 2.84 (Mann-Kendall p = 9.5010^− 3^) in placebo (See Supplemental Fig. 6).
Discussion and conclusions
Prolonged fasting is one of the few interventions consistently shown to extend lifespan and healthspan in model organisms. Despite its robust potential in clinical applications to treat, prevent, or delay most major diseases, the safety concerns, impracticality and patient burden associated with fasting limit widespread adoption. As such, interventions that mimic the beneficial effects of fasting could provide a safe and accessible alternative, especially for those unable to regularly fast. In this randomized, double-blind, placebo-controlled trial we investigated the impact of a novel fasting mimetic (Mimio) on hunger, satiety, digestive symptoms, cardiometabolic health, cognition and wellbeing in overweight older adults with elevated HbA1c. Mimio induced changes in both the subjective experience of hunger, satiety and digestion as well as the cardiometabolic blood profile over 8 weeks of supplementation. Daily hunger and satiety metrics improved substantially compared to placebo, with 91% vs. 47% of participants improving appetite across the study and all metrics exhibiting a statistical trend in the direction of improvement. Supplementation with Mimio also resulted in significant reductions in self-reported abdominal pain and bloating compared to placebo. Most strikingly, Mimio also induced fasting-like improvements to cardiometabolic blood markers with LDL particle number, total cholesterol, oxidized LDL-c, LDL-c, nonHDL-c and glucose concentrations improved significantly compared to placebo. Together, daily use of Mimio appears safe and tolerable and improved multiple metrics of hunger control, indigestion, lipid composition, cholesterol metabolism, oxidative stress and glycemia. These effects successfully “mimic” the metabolic changes observed during prolonged fasting without changes to diet or lifestyle.
Elevated levels of LDL particles are associated with an increased risk of CVD^50,51^. Among these, the small dense particles are more prone to penetrate the arterial wall, become oxidized and contribute to atherosclerosis^52–54^. In some studies, reduction in small dense LDL particle concentration has been linked to decreased CVD risk, especially when accompanied by improvements in other lipid parameters. For instance, therapies that lower LDL particle number and increase particle size have been associated with reduced progression of coronary artery disease^53–55^. Similarly, the change in fasted glucose here corresponds to a few mg/dL on average or 5–6 mg/dL in the most responsive quartile. However, these changes occurred over a short period of time with no recommended changes to diet or exercise. Given the linear progress over time in subjective sensations of hunger and satiety in the Mimio cohort, with no evidence of a tolerance effect, it is possible that blood metrics would also improve further with prolonged usage of the fasting mimetic.
Together, as the present study provided only 8 weeks of intervention, did not measure plasma levels of Mimio’s components to assess compliance and absorption variability, and did not strictly control for dietary intake, it is encouraging to see even modest improvements in lipid composition and fasting glucose. Longer duration studies including direct measurement of Mimio components in plasma will be necessary to clarify Mimio’s the full extent and variability of Mimio’s impact. Moreover, the addition of frequent lipid monitoring via point of care devices, weight reporting, continuous glucose monitoring or dietary standardization will elucidate how changes in metabolic markers relate to weight loss. Notably, unlike previous studies utilizing nicotinamide, spermidine, PEA and OEA individually, this study of the Mimio combination was performed in a population with no diagnosed metabolic, immune, cardiovascular or cognitive conditions or diseases, which may also account for a more modest effect size than observed in previous studies on similar biomarkers. However, the ability for a combination of natural molecules to significantly improve multiple relevant cardiometabolic risk factors and robustly improve multiple measures of hunger control in an already healthy population in just 8 weeks without the need to change diet or lifestyle presents a promising new approach for health optimization and disease prevention.
The present study results are consistent with the known mechanisms of action, pre-clinical and clinical impacts of nicotinamide/1-MNA, spermidine, PEA and OEA. 1-MNA extends lifespan in C. elegans through the induction of cellular antioxidant mechanisms^56^. Although there is no current recommendation for 1-MNA intake, its elevation through nicotinamide supplementation may treat or delay cardiac events and reduce inflammation^15,57^. Spermidine declines with age^14^ and its replacement extends lifespan in yeast, nematodes, flies and mice^58^. These benefits likely occur through multiple mechanisms, including stimulating autophagy^14^, reducing cardiac hypertrophy, improving mitochondrial respiration^59^ and reducing the inflammatory response^60^. Similar to spermidine and 1-MNA, PEA extends lifespan and increases survival through anti-inflammatory effects in mouse models^61,62^. PEA also has potential benefits in treating neurodegenerative and CNS disorders^16,63–65^, reducing intracellular lipid accumulation and oxidative stress in mice^66^. Finally, OEA has shown promising results in obesity both in animal models^17,67^ and humans^68,69^. Recent trials found that 8 weeks of OEA supplementation reduces inflammation (IL-6 and TNF-α) and oxidative stress in obese people^69^. The supplement also reduces weight, BMI, waist circumference, body fat percentage, hunger and cravings^68^. Like PEA, OEA increases the expression of fatty acid oxidation modulator PPAR-α and AMPK, promoting cellular lipid metabolism, downregulating glucose metabolism^68^ and potentially explaining the improved glucose and lipid markers in the present study. Moreover, OEA is a Nrf-2 activator^70^, enhancing cellular antioxidant production and potentially accounting for the decrease in oxidized LDL observed here.
Together, our results support and extend previous animal and human research into the impacts of 1-MNA, spermidine, PEA and OEA on subjective hunger and satiety, oxidative stress and cardiometabolic factors. Importantly, as mentioned above, the data from this study shows that these effects are not limited to diseased populations and that Mimio can exert similar benefits in healthy people, underscoring its potential for health optimization beyond the resolution of disease symptoms.
The present study was the first randomized, double-blind, placebo-controlled clinical trial to evaluate a fasting mimetic formulation containing nicotinamide, spermidine, PEA, and OEA. Mimio appears safe and well-tolerated and provides benefits to both the subjective experience of hunger and satiety, digestive comfort and objective cardiometabolic blood markers. Importantly, this is also the first study of its kind to show that a portion of the metabolic benefits of prolonged fasting can be phenocopied via simple supplementation with bioactive molecules elevated in the body during prolonged fasting (Mimio). This paves the way for the research and discovery of additional novel fasting mimetic compounds and the development of other biomimetic formulations that may be used to replicate the effects of similar beneficial biochemical states such as exercise. Future study is warranted to establish the longer term impacts of Mimio and evaluation of a larger population of both men and women is necessary to describe potential sex-specific effects. Additionally, given the beneficial impacts on hunger, satiety and digestive comfort, we hypothesize that Mimio may aid in weight loss over a longer period of time and may trigger a new homeostatic setpoint to lipid metabolism. Finally, given the lifespan extending effects demonstrated by Mimio and its constitutive ingredients in previous studies, future studies of Mimio should focus on its hypothesized ability to reduce markers and metrics of biological aging in humans, particularly elderly cohorts for whom fasting would otherwise be unsafe.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee, C. & Longo, V. Dietary restriction with and without caloric restriction for healthy aging. F 1000 Research 5, F 1000 Faculty Rev-117 (2016).10.12688/f 1000 research.7136.1PMC 475541226918181 · doi ↗ · pubmed ↗
- 2Gabandé-Rodríguez, E., Gómez de las Heras, M. & Mittelbrunn, M. M. Control of inflammation by calorie restriction mimetics: On the crossroad of autophagy and mitochondria. Cells. 10.3390/cells 9010082 (2019). .10.3390/cells 9010082 PMC 701732131905682 · doi ↗ · pubmed ↗
- 3Gebicki, J. et al. 1-Methylnicotinamide: A potent anti-inflammatory agent of vitamin origin. Pol J. Pharmacol (2003).12856834 · pubmed ↗
- 4Watała, C. et al. Anti-diabetic effects of 1-methylnicotinamide (MNA) in streptozocin-induced diabetes in rats. In Pharmacological Reports. 10.1016/S 1734-1140(09)70010-6 (2009). 10.1016/s 1734-1140(09)70010-619307696 · doi ↗ · pubmed ↗
- 5Alhouayek, M. & Muccioli, G. G. Harnessing the anti-inflammatory potential of palmitoylethanolamide. Drug Discov. Today. 10.1016/j.drudis.2014.06.007 (2014) (preprint). 10.1016/j.drudis.2014.06.00724952959 · doi ↗ · pubmed ↗
- 6Artukoglu, B. B., Beyer, C., Zuloff-Shani, A., Brener, E. & Bloch, M. H. Efficacy of palmitoylethanolamide for pain: A meta-analysis. Pain Phys. (2017) (preprint).28727699 · pubmed ↗
- 7Thabuis, C. et al. Biological functions and metabolism of oleoylethanolamide. Lipids. 10.1007/s 11745-008-3217-y (2008) (preprint). 10.1007/s 11745-008-3217-y 18704536 · doi ↗ · pubmed ↗
- 8Brown, J. D., Azari, K. & Ayala, J. E. Oleoylethanolamide: A fat ally in the fight against obesity. Physiol. Behav.10.1016/j.physbeh.2017.02.034 (2017) (preprint). 10.1016/j.physbeh.2017.02.03428254531 · doi ↗ · pubmed ↗