Neonatal Adrenal Hemorrhage Mimicking Suprarenal Tumor in a 12‐Day‐Old With Escherichia coli Urosepsis
Khaled Sawafta, Hani Abu Hijleh, Yousef Samara, Tasbeeh Al-Kharraz

TL;DR
A 12-day-old baby with E. coli infection had an adrenal hemorrhage mistaken for a tumor, but it was managed without surgery.
Contribution
Highlights adrenal hemorrhage as a rare but important differential diagnosis in septic neonates with abdominal masses.
Findings
Adrenal hemorrhage was incidentally found in a neonate with E. coli urosepsis.
Conservative treatment with antibiotics and imaging was sufficient without evidence of malignancy.
The case supports noninvasive management when malignancy is ruled out.
Abstract
Neonatal adrenal hemorrhage is an uncommon finding that may resemble suprarenal tumors. We describe a term male neonate who developed Escherichia coli urosepsis and was incidentally found to have a left suprarenal cystic lesion. Imaging and laboratory workup excluded malignancy, and the infant remained stable under conservative treatment with antibiotics and serial ultrasound follow‐up. This case emphasizes the need to consider adrenal hemorrhage in septic neonates with abdominal masses and supports noninvasive management in the absence of malignant features.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
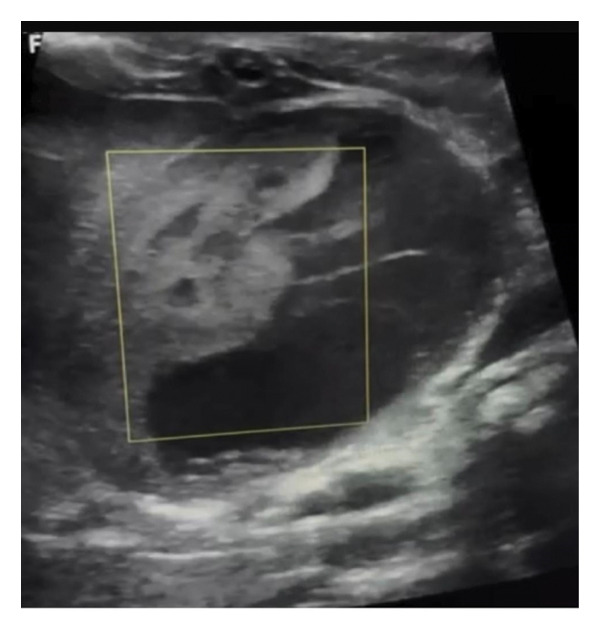 FIGURE 1
FIGURE 1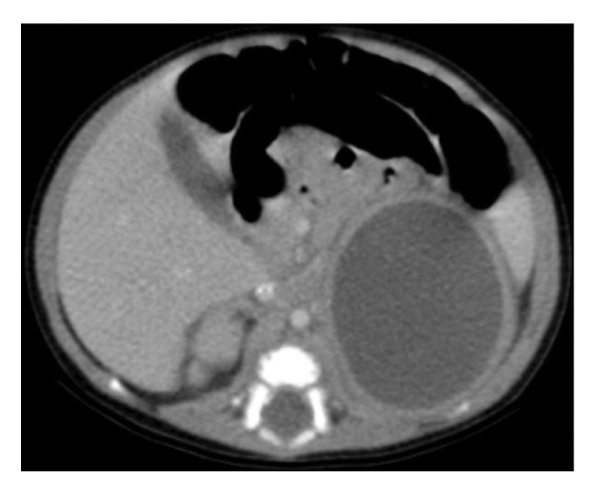 FIGURE 2
FIGURE 2 FIGURE 3
FIGURE 3 FIGURE 4
FIGURE 4| Parameter (reference range) | Day 6 | Day 7 | Days 9–12 | Days 15–20 | Days 24–30 | Day 36 | Day 45 |
|---|---|---|---|---|---|---|---|
| WBC (5.0–21.0 × 109/L) | 22.4 | 20.6 | 24.6–21.3 | 19.8–20.4 | 23.6–13.3 | 12.5 | 9.7 |
| CRP (< 5.0 mg/L) | 30 | + | 44–51 | 55–91 | 36–42 | 21 | 10 |
| Hgb (13.5–19.5 g/dL) | 15.2 | − | − | − | ↓ to ∼9 | 8 | 7.5 |
| Total bilirubin (< 12.0 mg/dL) | 11.7 | − | 10‐11 | 9‐10 | 8‐9 | 7.5 | 6 |
| Random blood glucose (50–90 mg/dL) | 60 | 50/89 | − | − | − | − | 89 |
| Age (days) | Clinical findings | Investigations performed | Results/impressions |
|---|---|---|---|
| 6 | Fever, suspected sepsis | CBC, CRP, blood culture | Leukocytosis, elevated CRP; blood culture negative |
| 12 | Confirmed urosepsis | Urine culture, abdominal ultrasound |
|
| 20 | Endocrine evaluation | Cortisol, 17‐OHP, DHEA | Cortisol and 17‐OHP normal; DHEA elevated (1800 ng/dL; ref: 50–850 ng/dL) |
| 36 | Follow‐up | Repeat US + CT scan | Lesion increased to 5 × 4 cm, heterogeneous; CT: nonenhancing left adrenal cyst, no calcification |
| 40 | Tumor marker assessment | AFP, β‐hCG, CA19‐9 | All within normal limits |
| 45 | Follow‐up | Repeat DHEA | DHEA decreased to 809 ng/dL |
| Reference (year) | Age at dx | Context of presentation | Imaging findings | Management | Outcome |
|---|---|---|---|---|---|
| Habeb et al. (2014) | 4 weeks | UTI workup; incidental adrenal hematoma | Large unilateral adrenal hematoma (left) | Conservative (antibiotics only) | Spontaneous resolution |
| Rumińska et al. (2015) | 3‐4 weeks | Sepsis; presumed adrenal abscess | Complex adrenal cyst/abscess (side NR) | Surgical drainage/exploration | Resolved after surgery |
| Mandelia et al. (2017) | 1‐2 weeks | Perinatal distress; bilateral adrenal abscesses | Bilateral suprarenal cystic masses with debris | US‐guided percutaneous drainage + IV antibiotics | Full recovery |
| Present case (2025) | 6 days |
| Left adrenal 4.0 × 4.5 cm cyst with septations, no flow | Antibiotics, watchful waiting | Clinical stability; follow‐up |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroblastoma Research and Treatments · Adrenal and Paraganglionic Tumors · Hormonal Regulation and Hypertension
1. Introduction
Neonatal adrenal hemorrhage (NAH) is a rare clinical occurrence, with an estimated incidence between 0.2% and 0.55% of live births. It is typically seen in full‐term male infants and is often associated with perinatal stress, sepsis, or hypoxia [1, 2]. Many cases are asymptomatic and detected incidentally, though some may present with an abdominal mass, jaundice, or anemia. Ultrasound is the imaging modality of choice for evaluation [3, 4].
A significant diagnostic challenge is differentiating hemorrhagic adrenal lesions from other suprarenal pathologies, such as adrenal abscess or neonatal neuroblastoma. The imaging similarities between neuroblastoma and NAH—particularly cystic or heterogeneous appearances—necessitate advanced imaging techniques and careful interpretation [5, 6].
This report describes a term male neonate with E. coli urosepsis and a left suprarenal cystic lesion, illustrating the diagnostic dilemma between hemorrhagic cyst, abscess, and tumor. The case underscores the importance of a systematic diagnostic approach, multidisciplinary collaboration, and vigilant follow‐up in managing neonatal suprarenal masses.
2. Case Presentation
A male neonate was delivered at 38 weeks of gestation via spontaneous vaginal delivery, with a birth weight of 3200 g. The perinatal course was uneventful. At 6 days of age, he presented with fever (38.5°C), poor feeding, and irritability. Laboratory investigations revealed leukocytosis and elevated C‐reactive protein (CRP), consistent with neonatal sepsis. Empirical intravenous antibiotics (ampicillin and cefotaxime) were initiated. Urine culture at 12 days of life yielded Escherichia coli, confirming urosepsis.
Abdominal ultrasound at presentation revealed a well‐defined, heterogeneous, anechoic left suprarenal lesion measuring 4.0 × 4.5 cm, with internal septations and mild bilateral hydronephrosis (Figure 1), suggestive of adrenal hemorrhage. A contrast‐enhanced CT scan on Day 20 demonstrated a nonenhancing left suprarenal cystic mass with homogeneous low attenuation, without calcifications or vascular invasion (Figure 2), consistent with a hemorrhagic adrenal cyst. Follow‐up ultrasound on Day 36 showed persistence of the lesion with mild enlargement (≈5 × 4 cm) and increased internal heterogeneity (Figure 3). Repeat CT confirmed a cystic suprarenal lesion with heterogeneous contents but no enhancement or calcifications (Figure 4), raising suspicion of infected hematoma versus adrenal abscess.
Initial abdominal ultrasound (Day 12) showing a heterogeneous left suprarenal cystic lesion with internal septations, suggestive of adrenal hemorrhage.
Contrast‐enhanced CT scan (Day 20) showing a left adrenal rim‐enhancing cystic mass without calcification or solid component, consistent with adrenal hemorrhage.
Follow‐up ultrasound (Day 36) showing enlargement and increased heterogeneity of the suprarenal cystic lesion.
Contrast‐enhanced CT scan (Day 36) showing a cystic suprarenal lesion with heterogeneous internal contents, without enhancement or calcifications, raising suspicion of infected hematoma versus adrenal abscess.
A second CT scan was performed due to the increase in size and internal heterogeneity observed on ultrasound, aiming to better characterize the lesion and exclude an evolving abscess or necrotic tumor, given the ongoing sepsis.
Serial laboratory follow‐up (Table 1) demonstrated persistent leukocytosis and markedly elevated CRP during the first 3 weeks, with a gradual subsequent decline. The infant developed progressive anemia (hemoglobin decreased from 15.2 to 7.5 g/dL), transient hyperbilirubinemia (peak 11.7 mg/dL), and episodic hypoglycemia (random glucose as low as 50 mg/dL), all of which improved over time. Endocrine evaluation showed normal cortisol and 17‐hydroxyprogesterone levels, with transient elevation of dehydroepiandrosterone (DHEA) that later decreased. Tumor markers (alpha‐fetoprotein [AFP], beta‐human chorionic gonadotropin [β‐hCG], and carbohydrate antigen 19‐9 [CA19‐9]) were within normal limits.
By 45 days of life, laboratory parameters had nearly normalized. Follow‐up ultrasound at the same age showed a decrease in lesion size and internal heterogeneity, consistent with resolving adrenal hemorrhage. The infant remained clinically stable. A multidisciplinary team including pediatric surgery and infectious disease specialists recommended conservative management with close monitoring, given the absence of malignant features, improving laboratory trends, and overall clinical stability. The clinical timeline is summarized in Table 2.
3. Discussion
This case describes a rare presentation of E. coli urosepsis with an associated left adrenal hemorrhagic cyst. NAH occurs more frequently on the right side (≈70% of cases) due to vascular anatomy, with bilateral involvement in about 10% and left‐sided cases in only 10%–15% [7, 8]. Risk factors include birth asphyxia, coagulopathies, traumatic delivery, and systemic infection [7, 8]. In our patient, the adrenal lesion was left‐sided and associated with E. coli sepsis without other perinatal insults. Sepsis is a known precipitant of adrenal hemorrhage; though most reported cases are linked to meningococcemia or generalized sepsis rather than urinary sources [8]. A comparison with representative cases is provided in Table 3. Clinical presentation varies: Many cases are asymptomatic, while others manifest as an abdominal mass, jaundice, anemia, or, rarely, adrenal insufficiency [9]. The male predilection observed in this case aligns with previous literature, where NAH is more commonly reported in male neonates, possibly due to hormonal influences or higher birth trauma rates [1, 7].
The diagnostic approach in this case was thorough, utilizing serial ultrasound, CT, and comprehensive laboratory testing to exclude malignancy and endocrine abnormalities. Although color Doppler ultrasound—a valuable noninvasive tool for distinguishing avascular hematomas from vascularized tumors—was not employed, CT provided detailed anatomical and enhancement characteristics crucial for differentiation in this clinically complex scenario.
Management of neonatal adrenal lesions remains variable. While some cases, particularly abscesses, may require drainage or surgery [10, 11], conservative management with antibiotics and monitoring is appropriate in the absence of liquefied abscess, hemodynamic instability, or malignant features [7, 12]. In our patient, the decision to avoid invasive intervention was supported by clinical improvement, stable imaging findings, and the absence of adrenal insufficiency.
The patient was followed until 45 days of age, by which time significant clinical and radiological improvement was evident. Long‐term follow‐up data are not available due to the family’s relocation; however, the observed trend toward resolution supports a favorable outcome, consistent with the natural history of uncomplicated adrenal hemorrhage.
This case highlights the importance of considering adrenal pathology in septic neonates with abdominal masses and demonstrates the value of a stepwise, multidisciplinary approach. By reporting this case in accordance with SCARE guidelines, we provide a detailed account that may assist clinicians in similar scenarios.
4. Conclusion
This case illustrates a rare presentation of NAH associated with Escherichia coli urosepsis, initially mimicking a suprarenal tumor. Differentiating benign hemorrhagic lesions from infectious or malignant masses requires a comprehensive, stepwise approach including imaging, endocrine evaluation, tumor markers, and close clinical monitoring. Conservative management with antibiotics and serial imaging successfully averted unnecessary surgical intervention. This report underscores the importance of including adrenal hemorrhage in the differential diagnosis of abdominal masses in septic neonates and supports a noninvasive strategy when malignancy is excluded and the clinical course remains stable [13, 14].
Author Contributions
Khaled Sawafta collected the clinical data, organized the laboratory and imaging findings, and drafted the initial manuscript.
Hani Abu Hijleh supervised the overall patient management, provided critical input regarding the surgical aspects, and contributed to revising the manuscript.
Yousef Samara assisted in the literature review, interpretation of clinical data, and editing of the manuscript.
Tasbeeh Al‐Kharraz reviewed and interpreted the ultrasound and CT images, prepared the radiological descriptions, and contributed to figure preparation.
Funding
No specific grant from funding agencies was received for this work.
Disclosure
All authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Ethics Statement
Our institution does not require ethical approval for reporting individual case reports or case series.
Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Toti M. S. et al., Neonatal Adrenal Hemorrhage: Clinical and Ultrasonographic Characteristics, Italian Journal of Pediatrics. (2019) 45, no. 1.10.1186/s 13052-019-0651-9PMC 650704431068206 · doi ↗ · pubmed ↗
- 2Esslami R. et al., Adrenal Hemorrhage in Newborn: How, when and Why—Case Report, BMC Pediatrics. (2022) 22.10.1186/s 12887-022-03314-1PMC 906972135513814 · doi ↗ · pubmed ↗
- 3Tognato E. et al., Neonatal Adrenal Hemorrhage: Clinical and Diagnostic Challenges, Journal of Ultrasound. (2020) 23, no. 4, 507–514.
- 4Tolson J. , Neonatal Adrenal Hemorrhage: Imaging Findings and Evolution, Applied Radiology. (2019) 48, no. 5, 20–25.
- 5Eo H. , Kim J. H. , Jang K. M. et al., Imaging Findings of Neonatal Adrenal Hemorrhage and Neuroblastoma: a Diagnostic Dilemma, Korean Journal of Radiology. (2011) 12, no. 1, 52–58, 10.3348/kjr.2011.12.1.52, 2-s 2.0-78651504549.21228940 PMC 3017884 · doi ↗ · pubmed ↗
- 6Kaba M. et al., Differentiation of Adrenal Hemorrhage from Adrenal Malignancies in a Neonatal Case by Superb Microvascular Imaging, Pediatric Urology Case Reports. (2020) 7, no. 5, 125–130.
- 7Toti M. S. , Ghirri P. , Bartoli A. et al., Adrenal Hemorrhage in Newborn: How, when and why–from Case Report to Literature Review, Italian Journal of Pediatrics. (2019) 45, no. 1, 10.1186/s 13052-019-0651-9, 2-s 2.0-85065485264.PMC 650704431068206 · doi ↗ · pubmed ↗
- 8Galal M. A. , Hafeez M. , Khan A. , Bolkini M. , and Ambadi N. P. , Neonatal Adrenal Haemorrhage Caused by Escherichia coli Sepsis, Hamdan Medical Journal. (2023) 16, no. 3, 322–325, 10.4103/hmj.hmj_41_23. · doi ↗