Embolization therapy for pelvic arteriovenous malformations: a systematic review
Chiara Brechbühl, Nicolas Diehm, Hanno Hoppe

TL;DR
This paper reviews embolization therapy for pelvic arteriovenous malformations, showing it is effective and safe with high success rates.
Contribution
The study provides a systematic review of embolization techniques and outcomes for pelvic AVMs, highlighting the need for standardized treatment strategies.
Findings
Embolization therapy achieved high technical and clinical success rates in treating pelvic AVMs.
Venous approaches, especially direct puncture of a dominant outflow vein, were most commonly used.
Coils were the primary embolic agent, often combined with adjunctive materials.
Abstract
A pelvic arteriovenous malformation (AVM) is a rare congenital vascular anomaly that may cause relevant clinical symptoms. This systematic review synthesizes current evidence on diagnostic approaches, embolization techniques, and clinical outcomes for pelvic AVMs. A PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses)-compliant literature search identified 19 studies comprising 49 patients treated with embolization therapy. Venous approaches, including direct puncture of a dominant outflow vein (DOV), were most commonly performed. Coils were the primary embolic agent, frequently combined with adjunctive materials, reflecting substantial technical heterogeneity. Despite this variability, embolization achieved consistently high technical and clinical success rates with low complication rates over a mean follow-up of 21.1 months. Embolization therapy of DOV may be…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
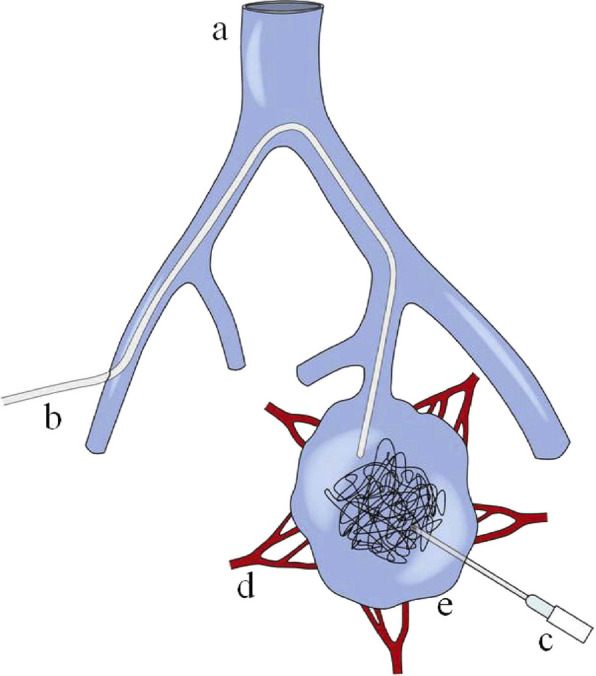 Figure 1
Figure 1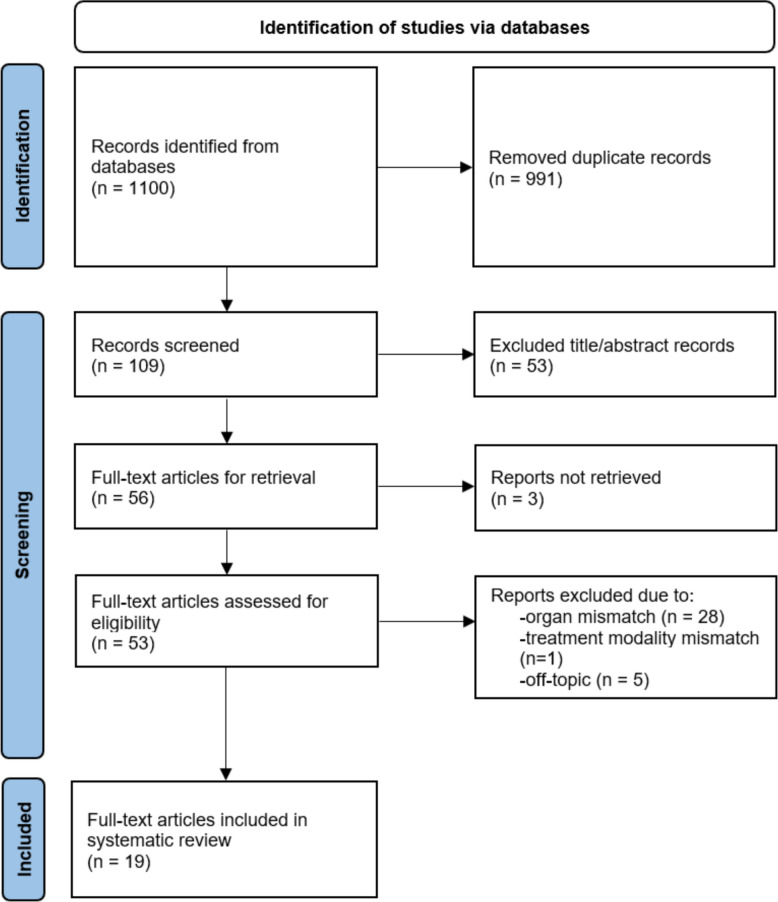 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations and Hemangiomas · Vascular Malformations Diagnosis and Treatment · Vascular Anomalies and Treatments
Background
Pelvic arteriovenous malformations (AVMs) are rare vascular abnormalities characterized by direct, anomalous connections between arteries and veins that bypass normal capillary networks. Although AVMs are more commonly encountered in the brain, lungs, or kidneys, pelvic AVMs present unique diagnostic and therapeutic challenges because of their complex anatomy and diverse clinical manifestations, including pelvic pain, constipation, hematuria, menorrhagia, and hemorrhage [1].
Congenital pelvic AVMs arise from embryological vascular malformations, whereas uterine AVMs are mainly considered to be acquired, often secondary to uterine trauma such as curettage or cesarean section. This study focuses on congenital pelvic AVMs, which generally exhibit a complex vascular architecture with multiple feeding arteries and draining veins, whereas acquired AVMs more often manifest as single fistulous communications [2]. Given their distinct anatomical and hemodynamic characteristics, pelvic AVMs are appropriately classified as a separate entity within Cho Type II AVMs [3]. Dysplastic arteries, usually originating from the internal iliac artery, form arteriovenous shunts with dominant outflow veins (DOVs) that typically drain into the internal iliac vein. The arteriovenous shunting of blood flow results in increased venous pressure, enhanced flow, and often marked vascular dilation within the venous system (Fig. 1) [4].Fig. 1. Schematic drawing of access routes to a dominant outflow vein (DOV) during the embolosclerotherapy of the pelvic AVM. A Inferior vena cava, B transvenous catheter, C percutaneous needle, D feeding arterioles, E DOV of a pelvic AVM. From: Do YS, Kim YW, Park KB, Kim DI, Park HS, Cho SK, Shin SW, Park YJ. Endovascular treatment combined with emboloscleorotherapy for pelvic arteriovenous malformations. J Vasc Surg. 2012 Feb;55(2):465–71.https://doi.org/10.1016/j.jvs.2011.08.051. PMID: 22,051,867. Elsevier
Pelvic AVMs frequently involve both the osseous and soft tissues of the pelvic wall. Doppler ultrasound serves as the initial diagnostic modality, often demonstrating turbulent, high-velocity flow. In addition, more specific cross-sectional imaging, such as computed tomography (CT) angiography or magnetic resonance (MR) angiography, should be performed to delineate lesion extent, surrounding structures, and feeding and draining vessels [5, 6]. A hallmark imaging feature of pelvic AVMs is rapid contrast enhancement of draining veins due to high-flow arterial shunting. Nevertheless, digital subtraction angiography (DSA) remains the gold standard, providing precise vascular localization essential for treatment planning [7].
In patients who are asymptomatic, conservative management with close observation and regular follow-up is considered safe and effective [8–10]. Intervention is typically reserved for patients with symptoms or complications, including bleeding or high-output cardiac failure. Surgical resection of pelvic AVMs is challenging because of the intricate vascular network, rapid reperfusion through collaterals, and the risk of complications, including bleeding or organ injury [11–14]. Accordingly, endovascular approaches, particularly embolization therapy, are preferred due to their minimally invasive nature associated with high technical and clinical success rates and low complication rates [15]. However, no consensus currently exists regarding the optimal embolization technique or choice of embolic agent [11].
The purpose of this systematic review was to assess the available evidence from studies on embolization of pelvic AVMs, focusing on procedural techniques, embolic materials, and clinical outcomes, to inform the best clinical practices and guide future research.
Methods
To ensure consistency, transparency, and methodological rigor, a comprehensive and systematic literature review was conducted according to the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) protocol across five electronic databases (PubMed, Embase, Web of Science, Cochrane Library, Scopus, and Google Scholar) covering relevant records published from December 2022 to October 2025 to evaluate the current evidence regarding safety, efficacy, and clinical outcomes of embolization therapy for pelvic AVMs [16]. Keywords included “pelvic”, “pelvic AVM”, “pelvic arterio-venous malformation”, “pelvic AVM embolization” and “pelvic arterio-venous malformation embolization”. Boolean operators (AND, OR) were used to combine search terms. Advanced search strategies were employed to refine the study design and publication type, with a focus on peer-reviewed meta-analyses, case reports, and observational studies. Additionally, filters for publication date and language, limited to English, were applied.
Each full-text article was manually reviewed by two independent readers (CB and HH) to confirm eligibility. Selected studies were graded for evidence level based on adaptations from existing guidelines according to Table 1 [17, 18]. A standardized data extraction form, as depicted in Tables 2 and 3, was developed to collect relevant information from each included study by two independent reviewers. Table 1. Levels of evidence adapted from the american society of plastic surgeons and Johns Hopkins nursing evidence-based practice: models and guidelines [18]LevelDescription1High quality prospective randomized controlled trials, cohort studies with adequate power, or systematic reviews of these studies2Lower quality prospective cohort, retrospective cohort studies, randomized controlled trials with untreated controls, or a systematic review/meta-analysis of these studies3Case–control studies or systematic review/meta-analysis of these studies4Case series, consensus statements, society guidelines, or practice guidelines5Expert opinion: case report, clinical example, or narrative reviewsTable 2Standardized data extraction summarizing relevant information from each included study. Data with focus on level of evidence, GRADE score, and diagnostic criteriaStudyYearLevel of evidenceGrade scorePat. noGender/ageLead symptomsImagingSideArteriesVeinsVein size (mm)AVM typeKwon et al.20254 (case series)E1 moderate (suggest coil embolization)1F/49pelvic painCT and/or MRN/AN/ADOV31IIa2F/30asymptomaticCT and/or MRN/AN/ADOV30N/A3M/49pelvic painCT and/or MRN/AN/ADOV61N/A4M/62asymptomaticCT and/or MRN/AN/ADOV50N/A5M/33asymptomaticCT and/or MRN/AN/ADOV31N/A6F/43asymptomaticCT and/or MRN/AN/ADOV45N/A7M/23pelvic painCT and/or MRN/AN/ADOV38N/A8M/62pelvic painCT and/or MRN/AN/ADOV51N/A9M/42thigh painCT and/or MRN/AN/ADOV28N/A10M/28asymptomaticCT and/or MRN/AN/ADOV15N/A11F/54pelvic painCT and/or MRN/AN/ADOV59N/A12F/53asymptomaticCT and/or MRN/AN/ADOV27N/A13F/20pelvic painCT and/or MRN/AN/ADOV23N/AKu et al.20255 (case report)E4 very low1F/27cardiac symptoms, dyspneaCTLIIADOVN/AN/AAmarneh et al.20254 (case series)E1 moderate (suggest US guidance for direct access)1M/18gastrointestinal bleedingCT, MR, US, DSAbilateralN/ASMV33N/A2M/3gastrointestinal bleedingCT, MR, US, DSARN/AIMV12N/A3M/13gastrointestinal bleedingCT, MR, US, DSALN/ASMV9N/A4F/25portal hypertensionCT, MR, US, DSARN/ASMV45N/A5M/58asymptomaticCT, MR, US, DSALN/AIIV33N/A6F/31cardiac symptomsCT, MR, US, DSAbilateralN/AIIV42N/A7F/23asymptomaticCT, MR, US, DSARN/ADOV9N/A8F/30asymptomaticCT, MR, US, DSAbilateralN/AIIV16N/A9M/23asymptomaticCT, MR, US, DSARN/ADOV45N/AInaguma et al.20255 (case report)E4 very low (suggest preop. embolization)1M/77fatigueCT, DSALIIAsaphenous veinN/AN/ASzmygin et al.20254 (case series)E1 moderate (suggest embolization is safer than surgery)1N/AN/ACT/MR, US, DSAN/AIMAN/AN/AN/A2N/AN/ACT/MR, US, DSAN/AIIAN/AN/AN/A3N/AN/ACT/MR, US, DSAN/Asacral arteryN/AN/AN/AViglione et al. 202420245 (case report)E4 very low (suggest venous access)1M/42pelvic painCT, USbilateralIIA, IMAIIV38N/ASitharthan et al.20245 (case report)E4 very low (suggest preop. embolization)1M/82urinary symptoms, enlarged prostateCT, DSARIIAIIVN/AN/AIzumi et al.20245 (case report)E4 very low (suggest embolization)1M/58varices L lower extremityCT, DSALIIADOVN/AIIGao et al.20245 (case report)E4 very low (suggest embolization)1F/17gastrointestinal bleedingCT, MR, DSARIIA, IMA, sacral arteryN/AN/AN/AOsuga et al.20245 (case report)E4 very low (suggest ethanol embolization via balloon)1M/40gastrointestinal symptoms, headacheCT, DSARIIA, inferior epigastric arteryDOVN/AIIYang et al.20245 (case report)E4 very low (suggest embolization)1F/40abdominal pain, lower back painN/ALuterine arteryDOV52N/AChan et al.20235 (case report)E4 very low (suggest embolization)1M/69cardiac symptomsCT, US, DSARIIA, lumbar arteriesIIV100IINazari et al.20235 (case report)E4 very low (suggest embolization)1F/36urinary symptoms (hematuria)CTbilateralIIAIIV, femoral veinN/AN/AHuang et al.20235 (case report)E4 very low (suggest US for diagnosis)1M/30abdominal pain, lumbar symptomsCT, USRIIAN/AN/AN/AAhmad et al.20235 (case report)E4 very low (suggest embolization with Squid)1M/29N/ACT, MR, DSALIIAN/AN/AN/ASagayanathan et al.20235 (case report)E4 very low (suggest embolization)1M/60pelvic painCT, MR, USRIIAN/AN/AN/ANguyen et al.20235 (case report)E4 very low (suggest embolization)1M/70urinary symptoms, enlarged prostateCT, US, DSARIIAN/AN/AN/AGrill et al.20234 (case series)E4 very low (suggest embolization)1N/Apelvic painMRN/AN/AN/AN/AN/A2N/Apelvic painMRN/AN/AN/AN/AN/A3N/Apelvic painMRN/AN/AN/AN/AN/AKim et al.20224 (case series)E1 moderate (suggest preop. embolization)1F/52cardiac symptoms, dypneaCTRlumbar artery, ovarian artery, IMAIIVN/AIIb2F/49vaginal bleedingCTRIAAIIVN/AIIb3F/61asymptomaticCTRIAAIIVN/AIIb4F/58abdominal painCTRIAAIIVN/AIIb5F/58abdominal painCTLIAAIIVN/AIIb6F/32asymptomaticCTRIAAIIVN/AIIb7F/52abdominal painCTLlumbar artery, ovarian artery, IMAIIVN/AIIbAbbreviations: L left, R right, CT computed tomography, MR magnetic resonance imaging, N/A not applicable, F female, M male, DOV dominant outflow vein, IIA internal iliac artery, IIV internal iliac vein, IMA inferior mesenteric artery, E evidence levelTable 3Standardized data extraction summarizing relevant information from each included study. Data with focus on therapeutic criteriaStudyYearPat. noGender/ageAccessEmbolic materialTechnical successClinical successComplicationsFollow-up (months)Kwon et al.20251F/49venouscoils (54)yesyesno10.52F/30directcoils (19)yesyesno12.73M/49venouscoils (59)yesyesmildN/A4M/62venouscoils (53)yesyesno23.55M/33venouscoils (27)yesyesnoN/A6F/43directcoils (30)yesyesno21.87M/23directcoils (21)yesyesnoN/A8M/62directcoils (238)yesyesno9.19M/42venouscoils (7)yesyesno24.310M/28venouscoils (74)yesyesno3911F/54venouscoils (57)yesyesno4.512F/53venouscoils (23)yesyesno14.213F/20venouscoils (62)yesyesno1Ku et al.20251F/27arterialN/AN/AN/AN/AN/AAmarneh et al.20251M/18directN/AyesN/Aminor venous access complicationN/A2M/3directN/AyesN/Aminor venous access complicationN/A3M/13directN/AyesN/Aminor venous access complicationN/A4F/25directcoilsyesN/AhemoperitoneumN/A5M/58directcoils, glueyesN/Aminor venous access complicationN/A6F/31directcoilsyesN/Aminor venous access complicationN/A7F/23directcoils, glueyesyespuncture renal arteryN/A8F/30directcoils, glueyesN/Aminor venous access complicationN/A9M/23directcoils, glueyesN/Aminor venous access complicationN/AInaguma et al.20251M/77arterial, directcoils, glueyesyesno3 weeksSzmygin et al.20251N/AarterialN/AN/AN/AN/AN/A2N/AarterialN/AN/AN/AN/AN/A3N/AarterialN/AN/AN/AN/AN/AViglione et al. 202420241M/42directcoils, glueyesyesnoN/ASitharthan et al.20241M/82arterialcoils, plugyesyesnoN/AIzumi et al.20241M/58arterialcoils, glue, ethanolyesyesno12Gao et al.20241F/17arterialglueyesN/AN/A1Osuga et al.20241M/40arterialcoils, ethanolyesN/Ano12Yang et al.20241F/40venouscoils, particlesyesyesfever12Chan et al.20231M/69arterial, venouscoils, glueyesyesmild postembolization syndrome3Nazari et al.20231F/36arterial, venouscoils, gelfoam, ethanol, sclerosant, particlesN/AN/AhematuriaN/AHuang et al.20231M/30arterialcoilsnonono19Ahmad et al.20231M/29arterialSquidpartial (50%)yesno24Sagayanathan et al.20231M/60arterialOnyxyesyesnoN/ANguyen et al.20231M/70arterialglueyesyesno2Grill et al.20231N/AN/AN/AN/AN/AN/AN/A2N/AN/AN/AN/AN/AN/AN/A3N/AN/AN/AN/AN/AN/AN/AKim et al.20221F/52arterial, venouscoils (84), ethanolpartial (> 80%)N/AN/A1862F/49arterial, venouscoils (233), ethanolyesN/AN/A363F/61venouscoils (69), ethanolyesNIAN/A244F/58venouscoils (53), ethanolyesN/AN/A185F/58venouscoils (183), ethanolyesN/AN/A186F/32venouscoils (89)yesN/AN/A137F/52venouscoils (266)yesN/AN/A6Abbreviations: L left, R right, CT computed tomography, MR magnetic resonance imaging, N/A not applicable, F female, M male, DOV dominant outflow vein, IIA internal iliac artery, IIV internal iliac vein, IMA inferior mesenteric artery, E evidence level
Studies were graded according to their relevance or importance to the field using the best-practice GRADE score [19]. This score is implemented for the rating of evidence certainty using the GRADE system, which categorizes the reliability of evidence into four levels: “High, moderate, low, and very low”. This score is developed to help users understand how much they can trust the results of a study or guideline, with “high” indicating high confidence that the true effect is similar to the estimated effect and “very low” indicating very little confidence.
Exclusion criteria included primarily duplicates, recurrent articles by the same authors, abstracts, inaccessible full-text articles, unpublished data, article languages other than English, and reviews or case reports published before December 2022, because these had already been included in a previous review [11]. Furthermore, studies focusing on AVMs in anatomical locations other than the pelvis, notably uterine AVMs, were excluded. Moreover, records investigating solely treatment modalities other than embolization therapy (e.g., surgery or conservative therapy) and publications not consistent with the objectives and topic of our research, were ruled out.
The review protocol was registered in the PROSPERO database (International Prospective Register of Systematic Reviews) prior to the initiation of the study to avoid duplication and ensure accountability (CRD420251207131).
Results
The PRISMA flow diagram depicted in Fig. 2 elucidates the study selection process, which consists of the following four stages: identification, screening, eligibility, and inclusion:
- Identification: A total of 1,100 records were initially identified from the six databases, all of which were imported into a reference management software (EndNote).
- Screening: After exclusion of 991 duplicates and repeated articles, 109 unique titles and abstracts were screened independently by two reviewers to identify potentially relevant studies. Discrepancies were resolved by consensus.
- Eligibility: Fifty-three full-text articles were retrieved and subsequently assessed for eligibility based on predefined exclusion criteria. The reasons for exclusion at each stage were documented.
- Inclusion: Nineteen studies met all eligibility criteria and were included in the final systematic review. Fig. 2. Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram demonstrating the study selection process, which consists of the following four stages: identification, screening, eligibility, and inclusion
A total of 49 patients who underwent endovascular embolization for congenital pelvic AVMs from nineteen studies authored by Kwon, Ku, Amarneh, Inaguma, Szmygin, Viglione, Sitharthan, Izumi, Gao, Osuga, Yang, Chan, Nazari, Huang, Ahmad, Sagayanathan, Nguyen, Grill, and Kim were included in this systematic review [11, 20–37]. Of these, 22 patients were male, 21 were female, and six patients were not specified in terms of sex. The average patient age was 43.5 years (range 3 to 82 years).
Clinically, the predominant presenting symptom was abdominal and/or pelvic pain, which was reported in 17 patients. Additional clinical manifestations, including gastrointestinal bleeding (n = 4), cardiac symptoms (n = 4), urinary symptoms (n = 3), thigh pain, gastrointestinal symptoms, and individual cases of fatigue, vaginal bleeding, and lower extremity varicose veins, were recorded. Twelve patients were asymptomatic. In four patients, symptoms were not specified.
Diagnostic imaging modalities across the cohort varied, reflecting heterogeneity in clinical practice. CT alone was performed in 10 patients, while three patients underwent magnetic resonance imaging (MR) only, and 13 patients received either CT or MR. A trimodality approach was used, where three patients were assessed with a combination of CT, MR and DSA or CT or MR, sonography and DSA (n = 3). Nine patients underwent comprehensive multimodality imaging comprising CT, MR, sonography and DSA. Moreover, one patient had CT, MR and sonography, whereas three patients received CT, DSA and sonography, and four patients underwent CT followed by DSA. CT and sonography were performed in two patients. In one patient, imaging modalities were not reported.
Pelvic AVMs were predominantly localized to the right side in 16 patients, whereas left-sided AVMs were identified in nine patients, and bilateral involvement was observed in five patients. In 19 cases, anatomical identification was not further specified.
Arterial feeders comprised the internal iliac artery in 19 patients. Other arteries included the inferior mesenteric artery (n = 5), lumbar arteries (n = 3), ovarian arteries (n = 2), sacral arteries (n = 2), obturator arteries (n = 1), inferior epigastric arteries (n = 1), and uterine arteries (n = 1). In 25 patients, arterial AVM feeders were not specified.
Venous drainage characterized by a DOV was specified in 19 patients. Venous drainage sites included the internal iliac vein (n = 14), superior mesenteric vein (n = 3), inferior mesenteric vein (n = 1), greater saphenous vein (n = 1), and concurrent right femoral vein in one patient. Venous drainage was not specified in 11 patients. The average diameter of these draining veins was 37 mm, with a range of 9 to 100 mm.
With respect to the AVM classification, seven patients presented with a type IIb lesion, one exhibited a type IIa lesion, three showed a type II lesion, and the majority (n = 38) were not further classified, highlighting a frequent lack of standardized reporting.
The average number of treatment sessions per patient was 2.4 (range of 1 to 13). The number of treatment sessions was not specified for 14 patients.
The access routes for endovascular AVM treatment were transvenous access in 15 patients, direct AVM puncture in 14 patients, transarterial access in 12 patients, both transarterial and transvenous access in four patients (one patient with covered endovascular reconstruction of the aortic bifurcation), both the arterial and direct approaches were used in one patient and were not further specified in three patients.
Embolic materials used were frequently coils (n = 18), coils in combination with glue (n = 7), coils with ethanol (n = 6), coils with glue and ethanol (n = 1), coils in combination with a vascular plug (n = 1), coils and particles (n = 1), glue alone (n = 2), Squid (n = 1), Onyx (n = 1), and coils in combination with gelfoam, particles, ethanol, and sclerosant (n = 1). The number of coils used per patient ranged from 7 to 266. These findings indicate high variability in embolic material selection. In 10 patients, embolic materials were not specified.
Technical success of endovascular treatment was reported positive in 38 patients, with technical failure in four patients and partial technical success in two patients. Technical outcome data were not reported for the remaining five patients. Clinical success, reflecting complete symptom improvement or lesion resolution, was recorded in 23 patients. Additionally, one patient experienced clinical failure, whereas clinical success was not reported in 25 patients.
Complication rates, including minor adverse events, were low. Minor adverse events, such as hematoma and postembolization syndrome with febrile response, occurred in 11 patients, and only one patient experienced iatrogenic right renal artery puncture due to the high complexity of the overall intervention. In contrast, 21 patients had no significant complications, while the complication status was not further outlined in 16 cases.
Moreover, wide variability across all the studies regarding follow-up duration, with an average interval of 21.1 months, ranging broadly from 0.8 to 186 months, complicates a structural and comprehensive assessment of both short- and long-term outcomes.
Among the 19 included studies, 14 were classified as level 5 evidence (case reports), and five were graded as level 4 evidence (case series). In accordance with the best-practice GRADE score, 15 studies were graded E4 (very low), while four studies were graded E1 (moderate).
Discussion
Previous studies have reported favorable outcomes for embolization therapy in patients with pelvic AVMs [20, 22, 37]. In the present review, most patients were classified as having Cho Type II AVMs [3], characterized by a distinct DOV draining into the internal iliac vein and primarily supplied by dysplastic branches of the internal iliac artery. In these patients, embolization targeting the DOV is considered the recommended treatment strategy [1]. Consistently, 71% (14/49) of the patients in the included studies underwent embolization of the draining veins, either using a transvenous approach or direct puncture at the shunt point where the feeding arteries converge into the DOV, which is critical for achieving successful outcomes [20, 22, 23, 29–31, 37].
Embolization therapy
The selection of embolic agents is key to treatment effectiveness. Coils were the most frequently used material, employed either alone or in combination with liquid embolics such as glue (n-butyl cyanoacrylate) or gelfoam and Onyx [31]. Emerging agents such as PHIL (precipitating hydrophobic injectable liquids) may enhance procedural safety and efficacy in complex cases [38]. However, no standardized protocols for embolic agent selection are currently available [11]. In the present study, coils were the preferred embolic material for treating pelvic AVMs in more than 87% (34/39) of patients. Recently, Kwon et al. reported the outcome of embolization therapy in 13 patients with Type IIa pelvic AVMs (DOV) using transvenous access (n = 10) or direct puncture (n = 4) [20]. In their study, DOV embolization was performed exclusively using coils. Their technical success rate was 92.9% (94% in the present study), and symptoms improved in all patients. Only one minor complication, namely a retroperitoneal hematoma that spontaneously resolved, occurred. Therefore, coil embolization of pelvic AVMs was demonstrated to be safe and effective within a median follow-up period of 13 months, ranging from 1 to 39 months. This method may be advantageous when liquid embolic agents pose additional risks or are contraindicated.
Liquid embolic agents, such as glue and Onyx, provide deep nidus penetration and durable occlusion (94% technical success) but demand high operator precision to avoid nontargeted embolization [39]. Improvements in microcatheter technology have further enhanced safety profiles [40]. Bioresorbable microspheres and agents such as PHIL contribute to tailoring embolization with controlled release and a reduced risk of ischemia. Huang et al. reported an 89% success rate without major complications, warranting larger trials [32, 41].
In the present study, the combination of coils and liquid embolic agents was used in 36% (14/39) of patients [11, 22, 23, 30, 31, 37]. When a combined approach using coils and liquid embolic agents is employed, coil packing should be performed first, followed by the administration of liquid embolic agents such as glue or Onyx. Larger detachable coils should be used to ensure a stable framework, followed by pushable coils for packing. Liquid embolic or sclerosing agents such as ethanol or polidocanol may subsequently be delivered directly into the shunt point to achieve complete stasis. This stepwise strategy improves controlled distribution of liquid embolic agent, promotes endothelial reaction, and minimizes the risk of nontargeted embolization [10]. Only if complete occlusion cannot be achieved via transvenous access or direct puncture alone, adjunctive transarterial embolization may be required to accomplish definitive AVM closure [30, 42]. Using this approach, Ghanaati et al. reported a 100% technical success rate with no recurrences across a 24-month median follow-up period, underscoring its utility despite higher technical demand [43].
While a diagnostic pelvic arteriogram is advised prior to DOV embolization, transarterial AVM embolization is generally not recommended since this approach typically does not facilitate enduring AVM obstruction because new feeding vessels develop and may necessitate multiple embolization treatments for clinical success [21, 24–28, 32–35]. However, transarterial embolization may be useful for reducing arterial inflow prior to DOV embolization to create more favorable conditions for positioning and polymerization of embolic agents [42].
Interestingly, Kim et al. performed transvenous embolization with coils and ethanol in seven patients with pelvic AVM, with a technical success rate of 86% [37]. However, no data on clinical success or complications have been reported. The median follow-up period was 43 months, ranging from 6 to 186 months (in this systematic review, the average follow-up period was 21.1 months [range 0.8 to 186 months]). Park and colleagues treated 84 patients with Type II pelvic AVMs with coils and ethanol and reported a clinical success rate of 64%, despite almost 90% of patients achieved full recovery or significant improvement [43].
Follow-up studies have consistently reported substantial symptom relief and improved quality of life after embolization. However, recurrence remains a concern, particularly in high-flow or incompletely occluded AVMs, with rates of up to 15% reported, highlighting the need for careful procedural planning, vigilant follow-up, and multidisciplinary management [24, 44].
Complications
Amarneh et al. evaluated embolization therapy for pelvic AVMs using direct puncture and coils and glue as embolic agents in nine patients who underwent a total of 25 procedures [22]. Their technical success rate was 100%. However, no follow-up data were available. Complications reported in their study included seven minor access complications, one case of hemoperitoneum, and one case of inadvertent right renal artery puncture. Other complications include mild postembolization syndrome, including fever (n = 3) and hematuria (n = 1) [20, 29–31]. Hence, the complication rate of the present study, as reported, was 39% (13/33).
Previously, Bae et al. treated three female patients with pelvic AVM using ethanol embolization (sclerotherapy), which had high complication rates (up to 25%), including bladder necrosis and ovarian insufficiency [45]. This emphasizes the high risk of ethanol-related complications such as pulmonary vasospasm, cardiovascular collapse, nerve injury, and skin necrosis. Similarly, Mallios et al. reported a complication rate of almost 30%, including major complications such as pulmonary embolism and femoral paresis, when liquid embolics were used via a transarterial approach [46].
Compared with liquid embolic agents, coil embolization appears to have a superior safety profile, and liquid embolic agents may carry increased risks of serious complications, including tissue necrosis and nontargeted embolization [45, 46]. Compared with transvenous or direct puncture, transarterial approaches are associated with higher complication rates [43].
The aforementioned risk of nontargeted embolization may be reduced by the use of proximal balloon occlusion or the placement of an optional IVC filter [1, 28, 47–49]. However, this approach may be somewhat limited in case of large-caliber DOVs. In the present study, the average DOV diameter was 42 mm, and the maximum DOV diameter was 100 mm [30]. Of interest is the so-called “push-through” method, which uses a vascular plug in the DOV for protection in combination with a previously placed detachable-tip microcatheter for retrograde AVM embolization [50].
Imaging
In the present study, predominantly sonography, CT-angiography, and/or MR-angiography were employed for pre-interventional imaging and treatment planning. Sonography, including color Doppler, is most frequently the initial examination used to demonstrate a mass with prominent periuterine vessels demonstrating intense color signals, aliasing, and potential reversal of flow [32]. These are indicators of turbulent high-velocity blood flow. A peak systolic velocity of less than 40 cm/s is associated with conservative therapy, whereas peak systolic velocities of more than 60 cm/s usually require timely treatment [51].
Cross-sectional imaging with CT and MR is advantageous for delineating AVMs, including adjacent anatomical structures and vessels. Most importantly, fast contrast uptake of dilated draining veins caused by arterial shunting is demonstrated on CT-angiography and, even more accurately, on MR-angiography [6, 52]. Although MR-angiography is proposed to be the imaging modality of choice, owing to its high spatial resolution, CT angiography may be superior for depicting small-sized arteriovenous shunt points where feeding arteries coalesce into the DOV. However, DSA remains the gold standard for pelvic AVM diagnosis and treatment planning and may be performed as an antecedent outpatient procedure or on the same day of treatment as an inpatient procedure [7].
Limitations
The data of this systematic review demonstrate heterogeneity concerning clinical presentation, imaging strategies, and embolization techniques in pelvic AVM management, with predominantly low levels of evidence. Furthermore, the data reported in the studies reviewed appear to be inconsistent, and data on long-term efficacy, recurrence predictors, and the impact on quality of life are lacking.
Practical recommendations
- MRA and/or CTA should be used for treatment planning.
- Pelvic angiography (DSA) should be performed within the treatment session to demonstrate both arterial supply and the DOV before embolization and to monitor treatment progress.
- Proximal feeding artery embolization should be avoided.
- For DOV embolization using a direct or transvenous approach, larger detachable coils should be placed first to create a framework, followed by the use of pushable coils for packing.
- Liquid embolic and/or sclerosing agents may be delivered to the AVM shunt point for complete stasis.
- Balloon occlusion or temporary inferior vena cava (IVC) filter placement should be considered to minimize the risk of pulmonary embolism.
- Additional transarterial embolization should be performed only if complete stasis is not achieved after using transvenous access and/or direct puncture.
Outlook
Ongoing technological advancements in imaging, embolic materials, and artificial intelligence-supported planning are expected to further refine treatment. Multidisciplinary care and expanded research focusing on standardized protocols in terms of procedural techniques andembolic agent selection, long-term outcomes, and equitable access are essential to meet current challenges to ultimately establish evidence-based guidelines. Moreover, current angiographic and cross-sectional imaging limitations prompt the exploration of three-dimensional printing and virtual reality for preprocedural simulation, although expertise and costs currently limit widespread use. The incorporation of psychosocial support and patient-reported outcome measures in clinical practice warrants consideration. Furthermore, robotic-assisted embolization and artificial intelligence–based tools may hold promise and offer future benefits for enhancing procedural precision, treatment planning, and outcome prediction.
Conclusion
The consistently high technical and clinical success rates, coupled with low complication rates, support embolization therapy, especially of DOV, as first-line treatment for complex pelvic arteriovenous malformations, offering durable outcomes and clear advantages in the majority of patients compared with surgical resection. However, the notable proportion of cases lacking detailed classification and comprehensive outcome reporting highlights the need for comparative research on embolization techniques, the establishment of standardized study protocols, and the development of evidence-based clinical guidelines supported by rigorous and robust data analysis in future investigations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Viglione M, Discalzi A, Mistretta F, Mancini A, Nardelli F, Bergui M. Bilateral congenital pelvic arteriovenous malformation: a case report and review of literature. J Endovasc Ther. 2024. 10.1177/15266028241267747. Epub ahead of print. PMID: 3910803510.1177/1526602824126774739108035 · doi ↗ · pubmed ↗
- 2Huang Y, Liu X, Qian H. A male congenital pelvic arteriovenous malformation diagnosed by abdominal ultrasound: a case report and literature review. Front Surg. 2023;9:2022.10.3389/fsurg.2022.907234 PMC 986967936700008 · doi ↗ · pubmed ↗
- 3Anton Sagayanathan P, Goai XY, Stephens D, Pridgeon S. Congenital periprostatic pelvic arteriovenous malformation presenting as isolated pelvic pain and requiring endovascular embolization. ANZ J Surg. 2023;93(6):1709–11. 10.1111/ans.18308. Epub 2023 Feb 2. PMID: 36732894.10.1111/ans.1830836732894 · doi ↗ · pubmed ↗
- 4Wang CY, Hu J, Sheth RA, Oklu R. Emerging embolic agents in endovascular embolization: an overview. Prog Biomed Eng (Bristol). 2020;2(1):012003.10.1088/2516-1091/ab 6c 7d PMC 845511234553126 · doi ↗ · pubmed ↗