Inflammatory Arthritis Uncovered Through Imaging of Osteonecrosis: A Case Series
Divya Pabbisetti, Anantaram Gudipati, Amber Papalkar, Sandeep Ponnaganti, Kiran Kumar Sailagundla

TL;DR
This study shows that imaging for osteonecrosis can reveal hidden inflammatory arthritis, even without typical symptoms or steroid use.
Contribution
The paper introduces a novel observation linking inflammatory arthritis to osteonecrosis through imaging findings in patients without steroid history.
Findings
MRI scans in three patients with osteonecrosis revealed signs of undiagnosed inflammatory arthritis.
Features like synovitis and erosions prompted further evaluation for inflammatory arthritis despite no clinical symptoms.
None of the patients had a history of steroid use, suggesting a possible new pathophysiological link.
Abstract
Osteonecrosis (ON) is typically viewed as an isolated condition stemming from vascular compromise. We present a three-case series demonstrating that MRI, performed to confirm the diagnosis of ON, incidentally revealed features consistent with underlying, previously undiagnosed inflammatory arthritis (IA). Even in the absence of typical clinical features, the presence of imaging findings such as synovitis, tenosynovitis, and erosions should prompt a thorough clinical and serological evaluation for coexisting IA. An interesting point to note is that none of the three patients reported a history of steroid use. This manuscript aims to highlight a possible pathophysiological link between IA and ON.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1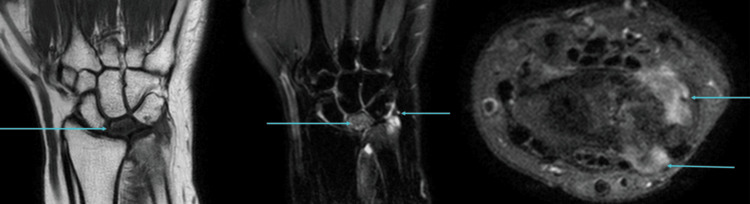 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4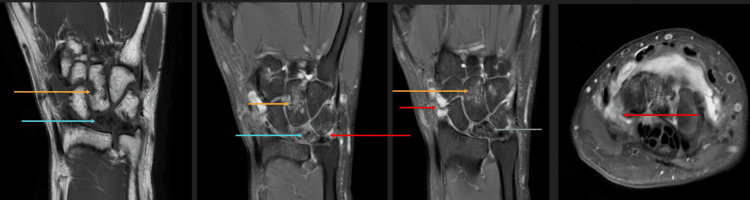 Figure 5
Figure 5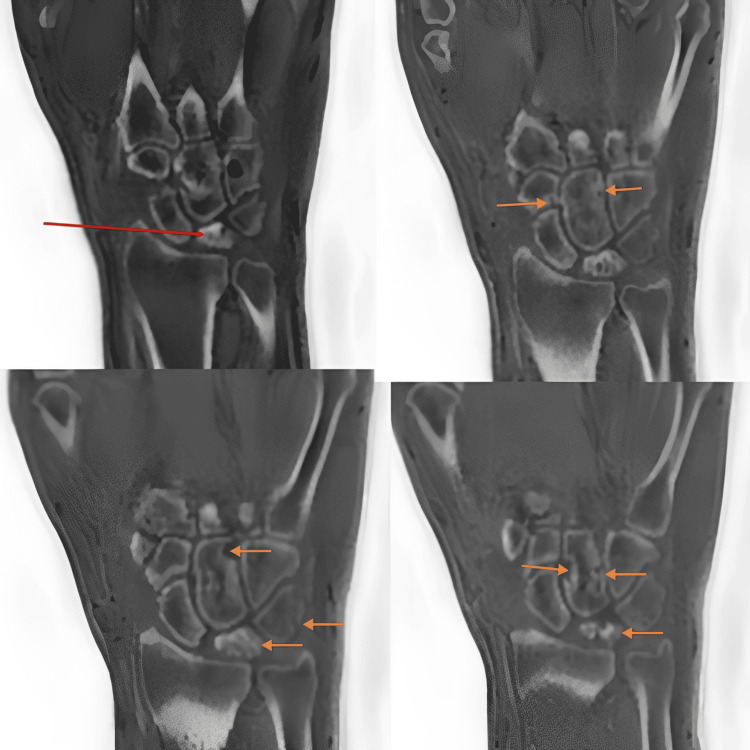 Figure 6
Figure 6 Figure 7
Figure 7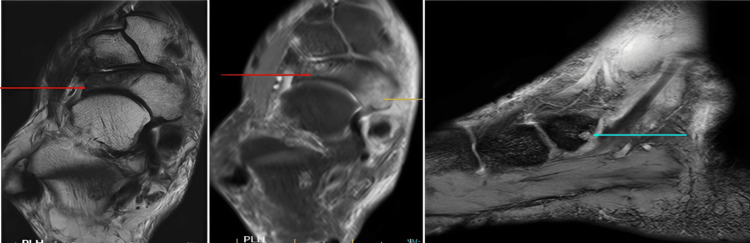 Figure 8
Figure 8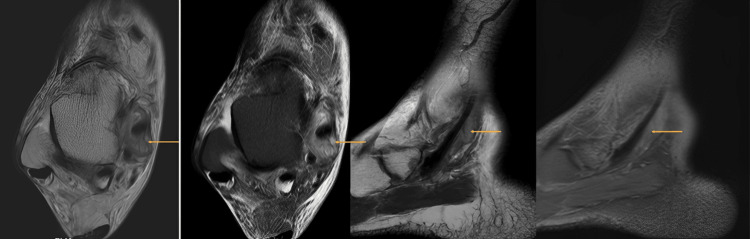 Figure 9
Figure 9| Parameter | Value | Normal range |
| ESR | 45 mm/hr | 0-20 mm/hr |
| CRP | 1.47 mg/dL | <0.5 mg/dL |
| Parameter | Value | Normal range |
| ESR | 38 mm/hr | 0-20 mm/hr |
| RA factor | 125 IU/ml | <14 IU/ml |
| Parameter | Value | Normal range |
| ESR | 31 mm/hr | 0-20 mm/hr |
| CRP | 0.63 mg/dL | <0.5 mg/dL |
| RA factor | 136.58 IU/ml | <14 IU/ml |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone and Joint Diseases · Spondyloarthritis Studies and Treatments · Osteomyelitis and Bone Disorders Research
Introduction
Osteonecrosis (ON) is the death of bone tissue resulting from impaired blood supply [1] and is typically identified using imaging modalities such as radiographs and MRI. In some cases, imaging may also reveal features suggestive of inflammatory arthritis, including synovitis, bone marrow edema (BME), and erosions, prompting reconsideration of the underlying diagnosis.
Here, we present two cases of Kienboch’s disease (osteonecrosis of the lunate bone) and one case of Müller-Weiss syndrome (adult-onset osteonecrosis of the navicular bone). In all three patients, plain radiographs initially demonstrated osteonecrosis, and subsequent MRI confirmed the diagnosis while also revealing features consistent with inflammatory arthritis. Laboratory investigations showed elevated inflammatory markers supporting this diagnosis. Notably, none of the patients had a prior diagnosis of inflammatory arthritis or a history of steroid use. This case series explores the potential relationship between osteonecrosis and inflammatory arthritis.
Case presentation
Case 1
A 51-year-old female presented with a six-month history of left wrist pain and restricted movement. She reported temporary relief of pain with nonsteroidal anti-inflammatory drugs. She was initially evaluated with a radiograph, which showed a partially collapsed and sclerotic lunate, suggesting the diagnosis of Kienbock’s disease (Figure 1).
AP radiograph of the left hand showing a partially collapsed and sclerotic lunate (arrow), suggesting Kienbock’s disease
For confirmation, an MRI was performed. MRI revealed partial collapse of the lunate with diffuse T1 hypointense signal and a chronic coronal fracture line, consistent with Kienbock’s disease. Synovitis was noted involving the distal radioulnar joint, pre-styloid recess, and piso-triquetral joint (Figure 2).
T1 coronal, PD-FS coronal, and axial images (left to right) showing partial collapse of the lunate with diffuse T1 hypointense signal and a chronic coronal fracture line (arrows, left and middle images)Synovitis is present in the distal radioulnar joint, pre-styloid recess, and piso-triquetral joint (arrows, middle and right images).PD-FS, proton density fat-saturated
A few erosions were identified in the triquetrum, and small osteophytes were seen arising from the distal radioulnar joint (Figure 3).
GRE coronal, PD-FS coronal, and GRE coronal images (left to right) showing a few erosions in the triquetrum (arrows, left and middle images)Small osteophytes are seen arising from the distal radioulnar joint (arrow, right image).GRE, gradient-recalled echo; PD-FS, proton density fat-saturated
Kienbock’s disease with coexisting IA of the wrist and degenerative changes in the distal radioulnar joint. Laboratory parameters are summarized in Table 1.
The patient received an intramuscular injection of Depo-Medrol 80 mg, following which her pain score decreased from 8/10 to 2/10.
Case 2
A 46-year-old male presented with a three-month history of left wrist pain and restricted movement. He was initially evaluated with a radiograph, which showed a partially collapsed and sclerotic lunate, suggesting the diagnosis of Kienbock’s disease (Figure 4).
AP radiograph of the left hand showing a partially collapsed and sclerotic lunate (arrow), suggesting Kienbock’s disease
For confirmation, an MRI was performed. MRI revealed partial collapse of the lunate with irregular fragmentation, diffuse sclerosis, and ill-defined marrow edema, consistent with Kienbock’s disease. Synovial thickening and effusion were observed in the wrist, intercarpal and carpometacarpal joints, and pre-styloid recess. Multiple erosions with associated marrow edema were noted in the triquetrum, capitate, and hamate bones (Figure 5, Figure 6).
T1 coronal, PD-FS coronal, and axial images (left to right) showing partial collapse of the lunate with irregular fragmentation, diffuse sclerosis, and ill-defined marrow edema (blue arrows) consistent with Kienbock’s diseaseSynovial thickening and effusion are present in the wrist, intercarpal, and carpometacarpal joints and pre-styloid recess (red arrows). Multiple erosions with associated marrow edema are seen in the triquetrum, capitate, and hamate bones (orange arrows).PD-FS, proton density fat-saturated
ZTE coronal images showing partial collapse of the lunate with irregular fragmentation and diffuse sclerosis (red and orange arrows, top left, bottom left, and right images) consistent with Kienbock’s diseaseMultiple erosions are seen in the triquetrum, capitate, and hamate bones (remaining orange arrows).ZTE, zero echo time
Kienbock’s disease with coexisting IA of the wrist. Laboratory parameters are summarized in Table 2.
The patient is being treated for seropositive erosive rheumatoid arthritis (RA).
Case 3
A 69-year-old female presented with pain in the dorsal aspect of the right midfoot and the medial aspect of the ankle. She was initially evaluated with a radiograph, which showed a partially collapsed and sclerotic lateral half of the navicular bone, along with mild lateral subluxation of the talar head and disruption of the cyma line. Based on these findings, a diagnosis of Müller-Weiss syndrome was made (Figure 7).
AP radiograph of the right foot showing a partially collapsed and sclerotic lateral half of the navicular bone (blue arrow) and mild lateral subluxation of the talar head with disruption of the cyma line (orange arrow), consistent with Müller-Weiss syndrome
For confirmation of the diagnosis and to evaluate medial-sided ankle pain, an MRI of the right ankle was performed. Imaging showed sclerosis with partial collapse and mild short tau inversion recovery (STIR) hyperintense signal changes involving the lateral half of the navicular bone, with no evidence of fragmentation, and mild secondary degenerative changes in the midfoot joints (talonavicular and naviculocuneiform joints) (Figure 8). A small erosion with extensive surrounding marrow edema was noted in the posteromedial aspect of the navicular bone at the site of insertion of the tibialis posterior tendon (Figure 8).
T2, PD-FS axial, and GRE sagittal images (left to right) showing sclerosis with partial collapse and mild STIR hyperintense signal changes involving the lateral half of the navicular bone with no evidence of fragmentation (red arrows)A small erosion with extensive surrounding marrow edema is present in the posteromedial aspect of the navicular bone at the site of insertion of the tibialis posterior tendon (yellow and blue arrows).GRE, gradient-recalled echo; PD-FS, proton density fat-saturated; STIR, short tau inversion recovery
Moderate synovial thickening and effusion were observed along the retro-malleolar tibialis posterior tendon sheath, suggestive of tenosynovitis (Figure 9).
T2 and PD-FS axial and sagittal images showing moderate synovial thickening and effusion along the retro-malleolar tibialis posterior tendon sheath (arrows), suggestive of tenosynovitisPD-FS, proton density fat-saturated
Müller-Weiss syndrome with coexisting inflammatory tibialis posterior tenosynovitis, including bony erosion and marrow edema at its navicular insertion site. Laboratory parameters are summarized in Table 3.
The patient is being treated for seropositive erosive RA by the rheumatology team.
Discussion
The reported cases underscore a compelling, yet often overlooked, intersection between avascular necrosis (ON) and IA. While ON is traditionally associated with well-defined risk factors such as exogenous steroid use, trauma, or alcohol abuse, its co-occurrence with IA, particularly in patients with no prior diagnosis, demands closer examination of the underlying pathomechanisms and the diagnostic utility of advanced imaging.
Pathophysiological link between inflammation and ON
Several mechanistic pathways may explain how systemic inflammation, characteristic of IA, contributes to the development of ON:
Systemic Inflammation and Vascular Dysfunction
The core inflammatory process in diseases such as RA and systemic lupus erythematosus involves the release of pro-inflammatory cytokines, notably tumor necrosis factor-alpha and interleukin-6. These mediators are known to induce endothelial damage and microvascular dysfunction [2]. The resultant vasculitis, or even subclinical endarteritis, can impair circulation to susceptible bone segments, directly causing the ischemic events central to ON [3]. This process is independent of the mechanical effects of joint inflammation.
Hypercoagulable State
Chronic inflammation drives a pro-thrombotic state. The upregulation of tissue factor and suppression of fibrinolysis contribute to hypercoagulability [4]. In the context of the small, end-arterial circulation supplying bones (especially the hip, lunate, and navicular), even minute thrombi can lead to arterial occlusion and subsequent bone infarction [5]. This is particularly relevant in Cases 2 and 3, where seropositivity (suggestive of RA) is strongly associated with an increased risk of thrombotic events.
Local Joint Environment and Pressure Effects (Specific to Epiphyseal ON)
While less relevant for the carpal and tarsal ON observed here, significant synovial inflammation and effusion can acutely elevate intra-articular pressure, compromising intraosseous blood flow, particularly in the femoral head ON [6]. The chronic, erosive nature of RA also locally impacts subchondral bone integrity.
Genetic Susceptibility and Lipid Metabolism
Beyond inflammation, IA may intersect with genetic predispositions for ON. Polymorphisms affecting lipid metabolism (e.g., lipoprotein lipase) or the coagulation cascade (e.g., Factor V Leiden) are known risk factors for idiopathic ON [7]. It is plausible that the added stress of systemic IA triggers ON in genetically predisposed individuals.
Diagnostic significance of advanced imaging
The incidental detection of inflammatory features on MRI in all three patients, initially evaluated solely for suspected ON, highlights the superior sensitivity of MRI in characterizing both bone viability and soft-tissue pathology compared to conventional radiography [8].
Synovitis and Tenosynovitis
The identification of synovial thickening and enhancement (as seen in Cases 1 and 2) or tenosynovitis (as in Case 3) provides direct evidence of an active inflammatory process not detectable on plain films. This finding is a critical diagnostic red flag in the workup of presumed isolated ON.
BME
BME, characterized by T2/STIR hyperintensity, is a non-specific but highly sensitive indicator of an active inflammatory or stress process. While BME is often seen adjacent to necrotic bone, the presence of extensive BME surrounding non-necrotic areas or associated with erosions (as noted in Case 3) strongly suggests active IA or associated mechanical stress [9].
Erosions
The presence of marginal bone erosions in the carpal bones (Cases 1 and 2) or at tendon insertions (Case 3, suggesting enthesitis or erosive tenosynovitis) is pathognomonic for an erosive arthropathy and necessitates immediate rheumatologic referral [10].
Conclusions
This case series highlights the need for a high index of suspicion for underlying IA when MRI performed for Kienböck’s disease (Cases 1 and 2) or Müller-Weiss syndrome (Case 3) reveals concomitant synovitis, BME, or erosions. The absence of a prior IA diagnosis or history of steroid use underscores the pivotal role of MRI in redefining the diagnosis. Early detection of seropositive erosive arthropathy (as confirmed in Cases 2 and 3) is crucial, as delayed treatment increases the risk of irreversible joint destruction.
The integrated radiological and clinical approach demonstrated here is essential: radiographs identify the classic ON pattern, but MRI provides the critical pathological context that guides systemic management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Osteonecrosis imaging Stat Pearls [Internet] Stroie OM Vu VH Treasure Island (FL)Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/38861639/38861639 · pubmed ↗
- 2The role of inflammation in venous thromboembolism Front Pediatr Branchford BR Carpenter SL 142620182987633710.3389/fped.2018.00142 PMC 5974100 · doi ↗ · pubmed ↗
- 3Osteonecrosis Kelley's Textbook of Rheumatology (Ninth Edition) Chang C Greenspan A Gershwin ME 169217112013
- 4Tissue factor, blood coagulation, and beyond: an overview Int J Inflam Chu AJ 367284201120112194167510.4061/2011/367284 PMC 3176495 · doi ↗ · pubmed ↗
- 5Nontraumatic osteonecrosis of the femoral head: ten years later J Bone Joint Surg Am Mont MA Jones LC Hungerford DS 111711328820061665158910.2106/JBJS.E.01041 · doi ↗ · pubmed ↗
- 6Imaging of synovial inflammation in osteoarthritis, from the AJR Special Series on Inflammation AJR Am J Roentgenol Thoenen J Mac Kay JW Sandford HJ Gold GE Kogan F 40541721820223428659510.2214/AJR.21.26170 PMC 8863650 · doi ↗ · pubmed ↗
- 7Integrative analyses of genes related to femoral head osteonecrosis: an umbrella review of systematic reviews and meta-analyses of observational studies J Orthop Surg Res Lee S Yoo JI Kang YJ 1821720223534628310.1186/s 13018-022-03079-4PMC 8961967 · doi ↗ · pubmed ↗
- 8Progression of knee osteonecrosis on MRI Radiol Case Rep Yong KL El-Haddad C Pillay S 6786831620213348889810.1016/j.radcr.2021.01.010PMC 7809248 · doi ↗ · pubmed ↗