Participant perspectives on a multimodal program for neuropathic pain after spinal cord injury
Meredith Pinkerton, Roberta Vastano, Kim D. Anderson, Marlon Wong, Gabriel Fernandez, Eva Widerström-Noga

TL;DR
A 12-week multimodal program for neuropathic pain after spinal cord injury reduced pain and improved participants' well-being, though some found effects short-lived.
Contribution
This study introduces a novel multimodal program combining education, exercise, and walking illusions to address neuropathic pain after SCI.
Findings
Participants reported reduced pain and pain interference after the program.
Pain assessment scores showed significant reductions in neuropathic pain severity and impact.
Some participants noted fatigue and minimal long-term pain relief.
Abstract
Spinal cord injury (SCI) results in several medical consequences. While some of these are immediate, others, like chronic pain, may emerge after weeks or months. Roughly 60% of individuals develop persistent neuropathic pain within the first year after injury. Due to the limited efficacy and negative side-effects of current pharmacological agents, many patients seek non-pharmacological options. The present mixed-method study explored individual perspectives of 35 participants with neuropathic pain and SCI on a multimodal 12-week pain program including pain education, exercise, and walking illusions. After completion of the program participants reported reduced pain and pain interference, better understanding of pain and pain management, and lower medication use. Other reported benefits included an expanded mindset, useful community and interpersonal connections, positive health…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
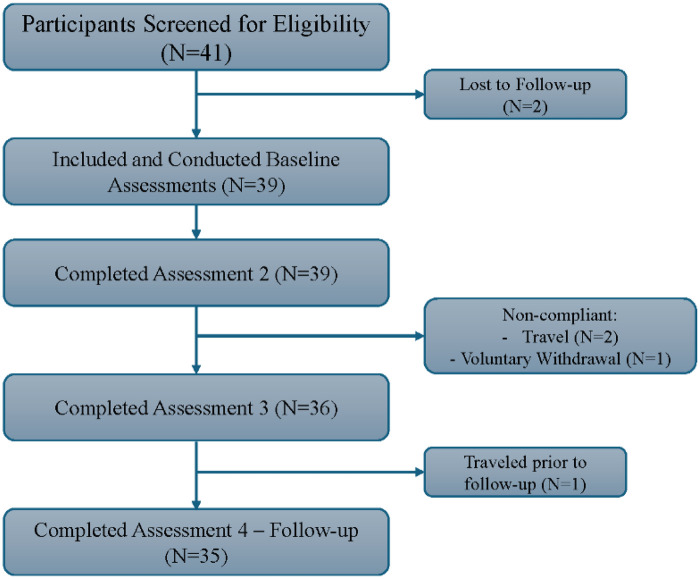 Figure 1
Figure 1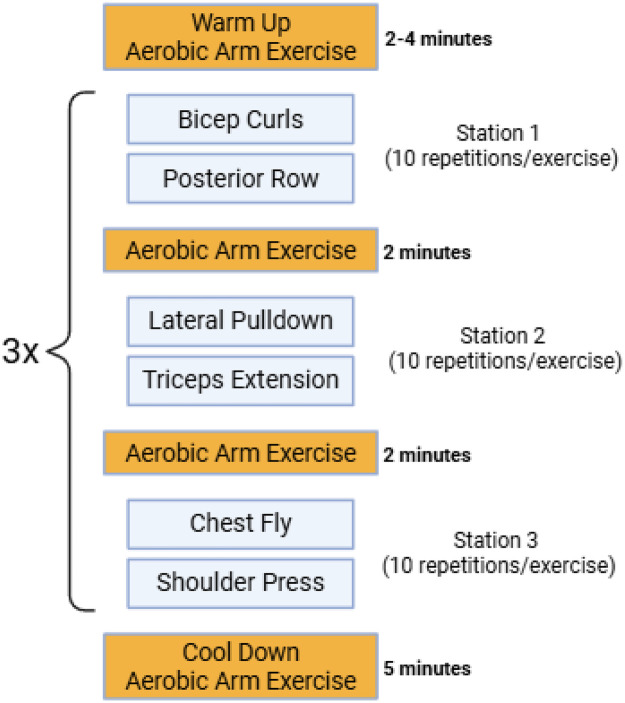 Figure 2
Figure 2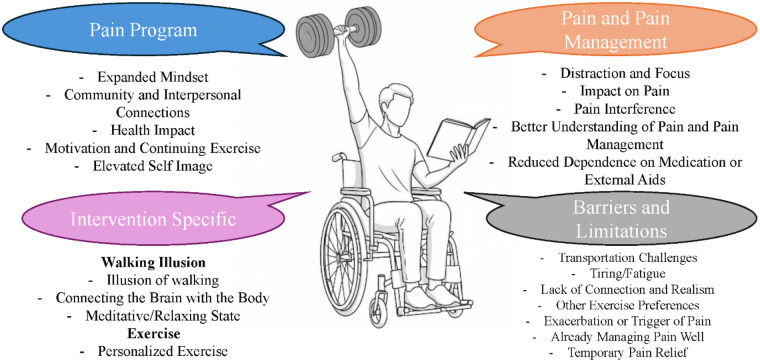 Figure 3
Figure 3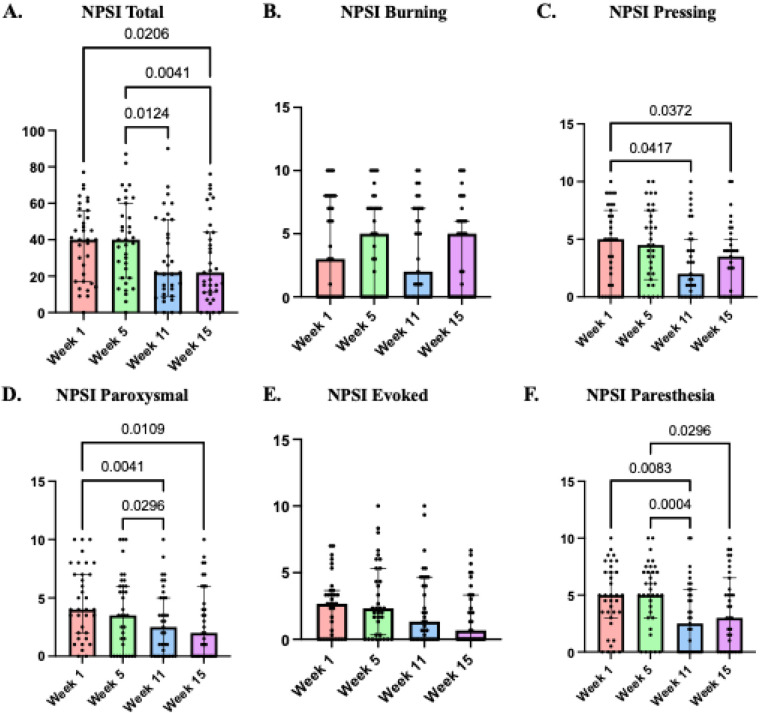 Figure 4
Figure 4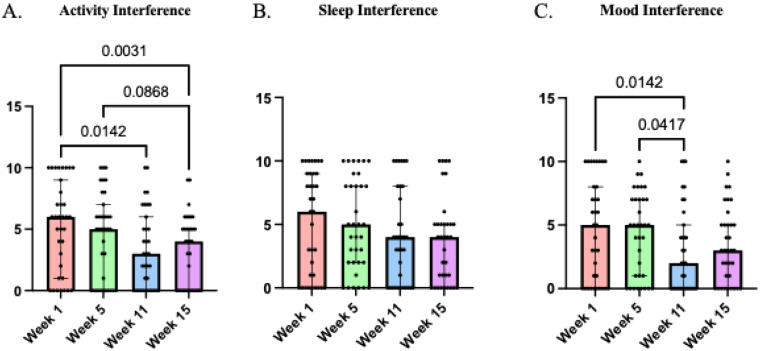 Figure 5
Figure 5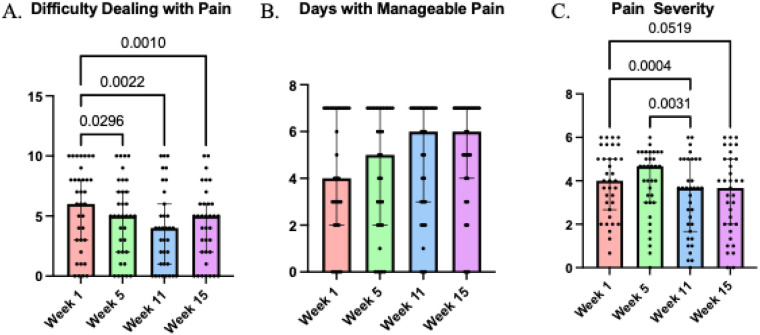 Figure 6
Figure 6| Participant | Age | Sex | Time Since Injury (Years) | ISNCSCI | Injury Level | Cause of Injury |
|---|---|---|---|---|---|---|
| 1 | 30 | F | 2 | D | C4 | Fall |
| 2 | 74 | M | 12 | D | C2 | Fall |
| 3 | 51 | M | 4 | D | T1 | Act of violence |
| 4 | 45 | M | 16 | D | C1 | Vehicle accident |
| 5 | 19 | F | 5 | D | C4 | Vehicle accident |
| 6 | 61 | M | 39 | A | C5 | Vehicle accident |
| 7 | 62 | M | 18 | D | C5 | Fall |
| 8 | 34 | F | 10 | C | T10 | Vehicle accident |
| 9 | 69 | F | 1 | A | T3 | Sporting accident |
| 10 | 19 | M | 0.5 | – | T11-T12 | Act of violence |
| 11 | 31 | M | 11 | C | C4 | Vehicle accident |
| 12 | 33 | M | 9 | A | C2 | Vehicle accident |
| 13 | 35 | M | 4 | B | C4 | Fall |
| 14 | 38 | F | 4 | A | T12 | Vehicle accident |
| 15 | 26 | F | 1 | B | L1 | Fall |
| 16 | 41 | M | 2 | B | C4 | Vehicle accident |
| 17 | 39 | M | 6 | A | T10 | Vehicle accident |
| 18 | 40 | F | 23 | A | C8 | Vehicle accident |
| 19 | 21 | M | 2.25 | A | C6 | Sporting accident |
| 20 | 47 | M | 23, 3 | D | L3-S1, C3-C6 | Other cause |
| 21 | 43 | M | 5 | D | T10 | Fall |
| 22 | 37 | F | 12 | D | T5 | Vehicle accident |
| 23 | 43 | M | 8 | D | C8 | Act of violence |
| 24 | 50 | M | 27 | D | C6 | Vehicle accident |
| 25 | 57 | M | 11 | D | T7-T9 | Other cause |
| 26 | 53 | M | 30 | C | C5 | Other cause |
| 27 | 43 | M | 8 | C | C5 | Fall |
| 28 | 54 | M | 6 | D | C4 | Vehicle accident |
| 29 | 55 | M | 8 | A | C4 | Vehicle accident |
| 30 | 36 | M | 1.25 | B | C7 | Vehicle accident |
| 31 | 30 | M | 6 | C | T10 | Vehicle accident |
| 32 | 28 | M | 7 | A | T5 | Vehicle accident |
| 33 | 40 | M | 0.92 | A | T5 | Vehicle accident |
| 34 | 42 | M | 6 | A | C6 | Sporting accident |
| 35 | 29 | M | 9 | A | T12 | Fall |
| Assessment 1 | Assessment 2 (Week 5) | Assessment 3 (Week 11) | Assessment 4 |
|---|---|---|---|
| Screening | Pain Education | Exercise and Bodily Illusion | Follow-up |
|
Demographic and Injury |
Pain Outcomes |
Pain Outcomes |
Pain Outcomes |
| Characteristics |
Sensory Outcomes |
Sensory Outcomes |
Sensory Outcomes |
|
Pain Outcomes |
Psychosocial Outcomes |
Psychosocial Outcomes |
Psychosocial Outcomes |
|
Sensory Outcomes |
Qualitative Interview |
Qualitative Interview |
Qualitative Interview |
|
Psychosocial Outcomes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPain Mechanisms and Treatments · Spinal Cord Injury Research · Pain Management and Treatment
Introduction
1
Among the numerous consequences of spinal cord injury (SCI), about 80% of individuals develop persistent pain within 12-months post injury (1), with 60% experiencing neuropathic pain (1). The refractory nature of neuropathic pain often significantly and negatively impacts quality of life (QOL) after injury (2). Pharmacological standard treatments include anti-convulsants (i.e., pregabalin and gabapentin) and tricyclic anti-depressants (i.e., amitriptyline) (3). However, these medications do not adequately alleviate pain for everyone (4), have numerous adverse side effects (5), and can be misused (6). Therefore, many people who experience neuropathic pain would like to have greater access to non-pharmacological options to better manage their pain (7). Non-pharmacological interventions used in SCI chronic pain research studies have for example included transcranial magnetic stimulation (TMS) (8–10), transcutaneous electrical nerve stimulation (TENS) (11, 12), transcranial direct current stimulation (tDCS) (13, 14), walking illusions, alone (15) and in combination with tDCS (16).
However, many of these interventions have been used in isolation and it is well known that chronic pain is a multidimensional experience influenced by multiple factors (17); therefore, a combination of treatments to manage SCI-related neuropathic pain may be optimal (7). One approach that can be easily incorporated with other treatments options is pain education. Indeed, patient education regarding pain following SCI has previously successfully been incorporated with both pharmacological and non-pharmacological interventions, and has been shown to improve pain outcomes (18). Pain education for chronic pain in SCI should include information regarding the underlying neurophysiological mechanisms of pain and be based on participant feedback regarding content (18, 19).
Similarly, other studies utilizing bodily illusions, like walking illusions (15, 20, 21), have shown that the manipulation of multisensory inputs like visual, tactile, and proprioceptive information can modulate body representation and potentially reduce neuropathic pain (22). After SCI, the deficits in somatosensory and motor function (23) have been linked to altered body perceptions and deficits in body representation in this population (22, 24–27). The analgesic effects of bodily illusions is caused by a correction of sensory-motor mismatch (15), activation of the somatosensory cortex (21), and modulation to other cortical regions when combined with tDCS (20). Although interesting, these types of studies mainly focused on mechanisms that generate analgesic effects and to date participants' perspectives on this type of intervention are still missing.
Finally, exercise in different forms has been shown to be potentially powerful for reducing the severity and negative impact of neuropathic pain. Although there is little research on the effects of exercise on SCI related neuropathic pain, there is compelling evidence that exercise improves pain outcomes in people with peripheral neuropathic pain (28, 29), heterogeneous central neuropathic pain (30), and heterogenous chronic pain (31, 32). There are numerous processes that may be underlying the analgesic effects of exercises (33) including neuroimmune mechanisms (31, 34, 35), modulation of inflammation (36, 37), and activity-dependent neuronal plasticity (36). Transient exercise-induced hypoalgesia has also been demonstrated within a single bout of exercise (38, 39) and has been shown to decrease pain sensation and temporal summation (40, 41). Therefore, the analgesic effects of exercise may partly be due to modulation of neuronal hyperactivity. Neuropathic pain is also closely linked to psychosocial factors, such as life interference, and exercise has improved overall wellness, cardiometabolic risk profile (42–44), psychosocial risk (45, 46) and functional ability (31, 47). However, despite these benefits, perspectives of individuals with SCI on exercise interventions remain largely unexplored.
Understanding participants' view on educational resources, bodily illusions and exercise components is crucial for designing patient-centered programs. Incorporating this feedback can help tailor non-pharmacological approaches alongside other pain management strategies. Therefore, with the repeated requests from the SCI community to have better access to non-pharmacological treatments options (48) and the emergence of promising multimodal approaches to make neuropathic pain manageable (49), we designed this mixed-method study to gain insights into participants' perspectives and explore neuropathic pain outcomes after a 12-week program including pain education, walking illusions and exercise sessions. The present study aimed to significantly expand on previous research in this population (50) by providing detailed feedback on the pain program by study participants with SCI who experienced moderate to severe neuropathic pain. Additionally, the present study evaluated pain and psychosocial outcome scores to complement the participant perspectives.
Methods
2
Study participants
2.1
Study participants were recruited via flyers posted at the Miller School of Medicine and from The Miami Project's research volunteer database. The study adhered to the principles of the Declaration of Helsinki. The study was reviewed and approved by Institutional Review Board of the University of Miami Miller School of Medicine and the Department of Defense Office of Human and Animal Research Oversight. All participants went through a screening and an informed consent process and provided written consent after confirmed eligibility.
Potential participants with a history of systemic illness (e.g., cardiovascular disease, multiple sclerosis, rheumatoid arthritis, cancer), severe depression (BDI-II > 29) (51), body mass index (BMI) > 35 (52), unhealthy alcohol (AUDIT>10) (53) or drug (DAST-10 > 6) (54) use within the past year, were not eligible for the study. Thirty-five adult participants with SCI completed the study (Figure 1). Participants included both men and women, aged 19–74 years, with either complete or incomplete traumatic SCI (C2-T12) who had experienced moderate to severe neuropathic pain for a minimum of 6 months [numeric rating scale (NRS) ≥ 4/10]. Participant demographics and injury characteristics are displayed in Table 1.
Flowchart of participant's retention.
Pain program design
2.2
This manuscript includes a subset of data from a larger 12-week mixed-methods research study. The overall pain program included four weekly 1-h group sessions of pain education (19), followed by six weeks of biweekly upper body exercise incorporating walking illusion, and concluded with a four-week follow-up period, shown in Table 2. This manuscript focuses on the qualitative and quantitative outcomes following the exercise and walking illusion interventions and the follow-up assessments as the results after pain education component were published elsewhere (55). The details of the pain program and its development were described in our previous articles (55, 56).
Pain education
2.2.1
During weeks 1–5, all participants completed a pain education block. Educational material was presented in a multitude of ways, including written and oral presentations and guided group discussions. All learning material was taken from the educational resource, SeePain (19). The material presented was regarding: (1) Types of Pain, Pain Experience, and Pain Mechanisms; (2) Real-life Cases of Pain after SCI; (3) Chronicity and Meaning of Pain after SCI; (4) Impact on Life; (5) Approaches to Managing Pain (pain medication, non-pharmacological treatments, self-management, and coping strategies); and (6) Literature resources and web links. The intent of pain education was to improve the participants' understanding of causes and types of pain and how to accurately communicate about their pain to family members and the healthcare community. Also, the pain education was aimed to clearly inform participants what to expect for long-term pain, how to access information regarding pain, and understanding pain management options. Data and details concerning the pain education sessions have already been published (57).
Exercise and walking illusion
2.2.2
Following pain education, individuals participated in 6-week biweekly upper body exercise circuit and walking illusion sessions. Biweekly sessions were administered individually to each participant. The type and duration of exercise were designed based on previous literature on exercise programs for SCI populations (54, 57, 58). All exercises were performed under the supervision of trained staff and investigators. Due to injury level or increased pain severity, adaptations were provided if needed. The resistance circuit, shown in Figure 2 consisted of bicep curls, posterior row, lateral pulldown, triceps extension, chest fly, shoulder press, and an aerobic arm exercise (arm bike or arm ergometer). Each exercise was performed with machines, resistance bands, and/or dumbbells. Movements were conducted to the subject's full range of motion and subjects were encouraged to maintain the same load. The training session began with a 2–4-min aerobic arm exercise warm-up and concluded with a 5-minute aerobic arm exercise cool down. The circuit consisted of 3 stations with 2 exercises in each station, separated with a 2-min aerobic arm exercise. Each exercise included 10 repetitions, with one repetition being 6-s total (3-s concentric, 3-s eccentric). The circuit was completed 3 times with a 15 s rest between stations, which brought the entire training program duration to 45 min. During the exercise sessions, momentary pain was recorded following each exercise. Blood pressure was measured before and after exercise for safety reasons. At the end of each circuit, exercise intensity was assessed using the Borg Rating of Perceived Excretion Scale (59).
Schematic of training circuit.
Following each exercise session, participants underwent a walking illusion. The walking illusion session was conducted as previously shown (15). Participants were seated in their wheelchairs facing a half-mirror, with their upper bodies visible in the mirror and their lower bodies hidden by a black blanket. A 20-min video was projected beneath the mirror, showing the legs of a person walking on a treadmill. The video was tailored to the participant's sex: men viewed males' legs and women viewed female legs. Participants were instructed to move their upper bodies in synchrony with the walking motion in the video, creating a visual experience that they were watching themselves walk.
Questionnaires and pain assessments
2.3
Pain evaluations
2.3.1
Pain evaluations were conducted in interview formats at each assessment week (baseline, 5, 11, and 15).
Pain history and classification
2.3.1.1
The International SCI Pain Basic Dataset (60) is part of the NIH SCI Common Data Elements and was used to provide a pain classification and overall description of all pain experienced. In addition, we used the Appendix A of the International SCI Pain Extended Dataset (60) which includes 7 questions regarding temporal pattern of pain, worst pain intensity, average pain unpleasantness, number of days with manageable pain, and momentary pain intensity.
Neuropathic pain severity
2.3.1.2
The Neuropathic Pain Symptom Inventory (NPSI) is a 12-item questionnaire, which was used to assess the severity of common neuropathic pain symptoms (61). The NPSI assesses five different dimensions of neuropathic pain: burning pain, pressing pain, paroxysmal pain, evoked pain, and paresthesia/dysesthesia. The NPSI has adequate psychometric properties in people with SCI (62).
Psychosocial evaluations
2.3.2
We used the SCI version of the Multidimensional Pain Inventory, MPI-SCI, to assess the psychosocial impact of pain (63). This was adapted from the West Haven-Yale Multidimensional Pain Inventory (MPI) which is a comprehensive instrument designed to assess a range of self-reported behavioral and psychosocial factors associated with chronic pain symptoms (63). The MPI-SCI consists of 50 items, that are answered on a 7-point Likert scale. In this manuscript, pain severity was assessed via the MPI subscale.
Qualitive interviews
2.4
Interviews were conducted via Zoom using an interview guide to ensure consistency. The interview guide probed the individual perspectives on the pain program. The interviews also examined the perceived impact of pain education, exercise, and walking illusion on participants' ability to manage their pain. During each interview, participants were asked a set of predetermined open-ended questions:
-
(i)Manageable pain: Please describe what manageable pain means to you right now.
-
(ii)Please describe your experience with the pain education/exercise/visual illusion part of the study.
-
(a)What did you like about it?
-
(b)What did you not like about it?
-
(c)What were the benefits, if any, of pain education/ exercise/visual illusion?
-
(d)What were the risks or burden, if any, of pain education/ exercise/visual illusion?
-
(iii)What impact, if any, did it have on your ability to manage your pain? Qualitative data is influenced by multiple factors that can affect responses in several ways, and therefore this type of data should not be treated as discrete, independent responses to be counted. Due to the open-ended qualitative interview questions, systematically quantifying each theme could potentially bias the qualitative data as some participants may not spontaneously express a specific opinion (64). We allowed participants to take the questions posed in the interview guide in their preferred direction, only adding probing questions related to the topic they brought up for clarification. Thus, it is not possible to ascertain whether a participant agreed or not with a specific theme if they did not mention it. The purpose of the interview probes was to gain clarity, detail, and more descriptive thoughts or feelings when necessary. To maintain a non-biased interview, we did not utilize responses from other participants to guide the conversation towards a specific theme or topic. For the purposes of the present paper only interviews conducted after the exercise/walking illusion were analyzed as their perspectives on the pain education were previously published (56).
Statistical plan
2.5
Qualitative
2.5.1
The sample size of 35 was consistent with our previous experience in qualitative research and on recommendations for qualitative research (65). The recommendations for grounded theory qualitative studies (66) suggested that such studies should generally include between 20 and 30 interviews. We conducted 35 interviews via zoom for each of the 4 test weeks. The transcripts of the interviews were entered into NVIVO (software headquartered in Lumivero, Denver, CO), coded independently by two coders, and further discussed in team meetings to ensure credible data and introduce revisions if appropriate.
Quantitative
2.5.2
Although this mixed method study was adequately powered for qualitative research the analyses of the pain and psychosocial scores were conducted to complement the qualitative analyses without statistical power considerations. Quantitative analyses were assessed for normality and homogeneity of variance using Shapiro–Wilk tests which indicated non-normality. Median scores for ISCIBPD-2 worst pain intensity, and pain interference with activities, mood, and sleep, difficulty dealing with pain and MPI sub-scales (pain severity, life interference, life control, affective distress, support, general activity, and pain impacting general activity), and total intensity NPSI score, were compared between baseline and post-pain education (week 5), post-exercise and bodily illusion (week 11), and post-follow-up (week 15). Non-parametric Friedman's test was used and pairwise post-hoc comparisons were uncorrected (Dunn's). All statistical analyses were conducted using GraphPad Prism version 10.0.0 for Windows, GraphPad Software, Boston, Massachusetts USA. Results were considered significant if values met p ≤ 0.05.
Results
3
The qualitative interviews reflected participants' perspectives directly after completing the pain program and at a follow-up, which was 4 weeks later. The main themes that were identified with representative quotes are summarized below. Participant perspectives with respect to benefits were categorized into the following over-arching themes regarding: (1) The pain program overall, (2) The specific interventions, (3) Pain and pain management, and (4) Barriers and limitations. Within these topics, specific subthemes were found and are listed in more detail below and in Figure 3.
Schematic of overarching themes and subthemes based on qualitative interviews of participant's perceptions on the pain program.
Pain program
3.1
Expanded mindset
3.1.1
Following the pain program, several participants stated that this program had influenced how they viewed their lives, “I can have a better life than what I'm living. There's more out there than I'd realized.” Some stated that it was “like a mindset shift of what I could accomplish in life now that I'm in a wheelchair”. Participants mentioned that they felt “not as constricted by pain” and instead of “just laying in bed,” some held the view that “you're better off going, even though you're in pain, just take your meds.” This program impacted participants differently; however, a common perspective on the benefits of the pain program shared by many participants is illustrated by “I'm processing pain differently.”
Community and interpersonal connections
3.1.2
Some participants mentioned that they valued being part of a supportive community and not being alone reflected in one participant's quote “I'm not alone in this,”. Another participant appreciated the sense of community, saying that it's “hard to get a group of guys that's had spinal cord injury”. Participants felt that “the interaction was a big part”, with some sharing the benefit of, “being able to be around the other people that are like me and talk to them and figure out things, and they tell me things that I don't know.” and the “wealth of knowledge amongst, not only the staff… but also stuff like spending time with other people in wheelchairs”. Many participants shared similar feelings, with one expressing, “the value of that there, there's no price I could put on that”. These perspectives highlight the value of community interaction in addition to specific interventions.
Health impact
3.1.3
Participants reported improvements in strength, mobility, and overall physical health. Many participants reported improvements in upper body strength “I'm not dragging myself,”, “I really see how, day to day, that upper body strength is really helping me”, and “Now I do believe my upper body is stronger, and I think because of that also, I might've clicked in better posture”. Some participants also noticed the benefit of increased core strength, illustrated by “my core body has gotten stronger so I'm not falling over” and “I could shift and I could stay there in a better position for a while”. Due to the increase in strength one participant noticed, “I can react faster, you know, stop or dodge something in the way”. Several participants attributed reduction in pain to be a result of the exercise, with one participant saying that the program “Increased my strength and decreased my pain”, and that “the more I exercise it out, the less tight that knot becomes,” and that their muscles are “not stiff” after exercise. Participants also noted other health benefits, “My blood pressure's been coming down” and that prior to the study, “my cholesterol was slightly elevated… I was able to lower it 50 points” by the 15-week follow-up. Others reported that “I mean, it made my life easier, it makes me stronger” and that “I start the day in another mood”.
Motivation and continuing exercise
3.1.4
Participants were encouraged by their progress throughout the program and got motivated, many of them stated “I didn't even know that I could do all that so I'm super happy and really motivated”, Additionally, some participants described feeling motivated also outside the research environment “I have more motivation to do everything. So I'm so happy” and “I'm always constantly moving. And then, my pain, I don't think of my pain. It really takes my pain away.”
Many participants were encouraged to incorporate what they learned during the program, saying “pushed me to start using the arm cycle again”, “I've been working out every day, trying to, and just trying everything that I've learned” “Like I'm going to continue working out on my own.”. With many having the determination*, “I don't care about the pain. I might as well just going to face it, little by little.” Because if I keep saying, “I'm not going to do shoulders because of the pain,” then “I'll never get there.”* and to “keep trying. Not to give up.”
Elevated self-image
3.1.5
Some participants expressed a new sense of self during this program, mentioning that they “liked how it made me feel.” With some expressing that “it brings back life almost” and “It made me feel energized. It made me feel alive.” Before this program, “I didn't even know that I could work out so hard”, and that this program is “a little bit more challenging, which is good”. Some participants started to “expand the ideas of how can I work out or what can I do” and gave the confidence to say, “Hey, I can do these workouts. I can do them every day. I just need to do it a little different,” “it opened my mind up to trying out other equipment.” This confidence translated in different ways for participants, with some saying, “I'm glad I did it because there's a way to face your fears,” and that they, “just felt more energy again”.
Intervention specific
3.2
Walking illusion
3.2.1
Illusion of walking
3.2.1.1
Participants felt that the walking illusion closely mimicked the sensation of walking*, “it's actually like a treadmill and it's moving, and it moves fast and it moves slow, and I find myself feeling like I'm actually moving my feet. I feel the circulation is more in my legs when I'm doing it, and so it feels like I'm really walking, and it feels good”.* Participants experienced ownership with the projected legs and reported “seeing myself walk” and feeling genuine movement through “counting the steps, movements, and rapid steps, slow steps,” creating a comprehensive sense of embodied movement. They also expressed feelings of agency (i.e., the ability to feel control over movements) “the brain sending my body the signal, I'm walking” and “where you can feel yourself telling your leg to move.” Additionally, participants actively engaged in imagination practices where they would “pretend like I'm walking with it” and “as far as just trying to imagine even yourself walking again”. A motivational aspect of this mental practice was also noted “motivated me and it helped me imagine myself if I was walking or if I was to walk”. Participants extended these imagination practices beyond their sessions, with some describing how they would sit “under the tree” and imagine “walking around the block” or observing people running around them and “thinking about that”. These experiences also had mood benefits where imagining “I would imagine myself walking again and then walking on the beach I used to. So I would see that and I'm like, okay. It would put me in a good mood.”
Connecting the brain with the body
3.2.1.2
Participants reported that the illusion facilitated bodily reconnection and integration “I could connect, that I was part of my body” “That kind of connects with my injury.”, and again “that the brain is connected”. This also elicited positive affective responses “I walk away from it in a very pleasant way, instead of being burdened by it”.
Meditative/relaxing state
3.2.1.3
Participants experienced meditative state and mental engagement during the bodily illusion interventions. The quotes reveal that the experience was “almost like a meditative state” and induced feelings of relaxation “getting into the character they put in front of you. And I don't know, it helps out. It relaxes you” “To me, it was a relaxation type of thing.”
Exercise
3.2.2
Personalized exercise
3.2.2.1
Participants reported that exercise programs were adapted to their physical limitations (e.g., weight adjustments, pacing), “I had to use the lowest weight. If I use heavier, try to prove something, I get in trouble with my neck, my shoulder, or something like that. So the weight, they accommodated the weight for me that I could handle” and “we took it easy and ramped it up slowly” with “enough time to rest my muscles in between,”. Supervision and expertise were seen as critical for maintaining safety, correcting posture, and encouraging appropriate challenges. This supportive environment encouraged participants to safely challenge themselves beyond their comfort zones, with the guidance allowing them “to challenge myself, to do something I wouldn't normally do” while maintaining confidence that “with their supervision, I felt good about it.”
Pain and pain management
3.3
Benefits and facilitators
3.3.1
Distraction & focus
3.3.1.1
Many participants perceived that the interventions “really distracted me… pain didn't get in the way” and “Took my mind off the pain”. Throughout the pain program, a new way to manage pain emerged for many participants. During the exercise intervention, participants noted that “when you just go through and through and just keep doing it, you don't think about the pain”; “it reinforced me that when I exercise I can take the pain and put it somewhere else. I can exercise and don't think about my pain problem.”, and that the bodily illusion allowed one participant to think, “Hey look, I can take my mind from here and visualize something else to keep your mind from the pain”. One participant expressed that this momentary relief of pain was positive because, “being able to live without pain, even for a few hours is better than living with pain all the time”.
Impact on pain
3.3.1.2
(a)Qualitative
Most participants described how the pain program positively impacted their overall pain. When asked to rate their pain, one participant noted pain levels dropping “from eight it went down to four, and from four sometimes I don't even feel it” and chronic pain that “used to always hurt would be at a constant six, maybe even a seven all day long. Right now, it's at a zero.” Participants described both immediate relief during exercise sessions where they became “pretty much pain-free” and some reported specific pains like, “shooting pain that I had in my biceps” and “neuropathic pain” that's “gotten better.” Throughout the exercise intervention, participants noticed progressive relief, saying their pain was decreasing during the exercise sessions “sometimes I will get there, and it's six or seven and by the time I start working they say”, “What's your pain?” I say, “I'm about four right now.” Then keep going, I said “I'm three”. Other participants reported longer-term changes post exercise sessions, where they say, “don't have any pain anymore and I believe it's because of the exercise that I did”; “I have less pain because I haven't noticed a lot of pain like before” and “just not in pain a whole lot now”.
- (b)Quantitative Consistent with participants' perspectives, quantitative pain outcomes improved. Non-parametric Friedman's ANOVA on NPSI total score showed a significant differences χ^2^(3 = 12.65, p = 0.006; Kendall's W = .12), with total NPSI scores decreasing from baseline (week 1) to week 15 and from week 5 to weeks 11 and 15. NPSI subscale scores, presented in panels B–F, also revealed significant reductions in clinically relevant domains, including pressing pain χ^2^(3 = 7.8, p = 0.05; Kendall's W = .07) with a decrease from week 1 to weeks 11 and 15, paroxysmal pain χ^2^(3 = 13.87, p = 0.003; Kendall's W = .13) with a decrease from week 1 to weeks 11 and 15 and from week 5 to week 11, and finally paresthesia/dysesthesia χ^2^(3 = 17.05, p = 0.001; Kendall's W = .16) with a decrease from week 1 to week 11 and from week 5 to weeks 11 and 15. Together with the qualitative findings these results indicate a meaningful reduction in neuropathic pain severity, particularly following the combined exercise and bodily illusion intervention (week 11), that remained at follow-up, as shown in Figure 4.
Neuropathic pain symptom inventory (NPSI) scores at weeks 1, 5, 11, and 15. (A) Summation of the total questionnaire (out of 100). (B–F) Clinically relevant dimensions of neuropathic pain syndromes were shown in their respective sub scores. P-values represented on the graph indicate Dunn's comparisons.
Pain interference
3.3.1.3
(a)Qualitative
Participants reported less pain interference in their daily activities during and after the pain program in many domains such as their activity, sleep, and mood.
Activity
3.3.1.3.1
Participants highlighted that the pain program directly enhanced their ability to manage daily life, promoting greater independence, confidence, and participation in meaningful activities. They reported that “Pain didn't get in the way of completing other tasks”; “I last way longer throughout the day now”; “I would say it impacted it greatly a lot because now I could sit in the chair.” Which opened the door to more active routines, “I was able to fill my calendar with some more activity” and “Things I couldn't easily handle or couldn't handle it at all before, now I'm handling them on the lower level.”
Sleep
3.3.1.3.2
Several participants described experiencing improved sleep following exercise. One participant noted it was “the best I would sleep at night. I would just rest at night.” Others reported that “when I come home, I can get a good rest” and that the program “gives you a better sleep, deeper”. Another participant reported, “I'm able to manage it better sleep”, highlighting the perceived benefits of the program on their overall restfulness.
Mood
3.3.1.3.3
Participants reported enhanced mood “I start the day in another mood, I'm so happy. I'm telling you that I'm so proud of myself doing what I doing now. I'm stronger, I'm more motivated and I am another person right now.”, and “So my mood is a little better, not as irritable because I'm in pain or not as agitated, I'm not as bothered because I'm in pain all the time”.
- (b)Quantitative: Friedman's ANOVA showed a significant reduction in pain interference related to daily activities χ^2^(3 = 14.82, p = 0.002; Kendall's W = .14) (with a decrease from week 1 to weeks 11 and 15 and from week 5 to week 15), and mood χ^2^(3 = 9.925, p = 0.019; Kendall's W = .09) (with a decrease from week 1 to week 11 and from week 5–11). Sleep interference was not significantly decreased χ^2^(3 = 4.55, p = 0.208; Kendall's W = .04). Interferences were assessed via the pain interference questionnaire, see Figure 5.
Interference in daily activities at weeks 1, 5, 11, and 15 of the multimodal pain program as indicated from the pain interference questionnaire: pain interfering with (A) activities, (B) sleep, and (C) mood. P-values represented on the graph indicate Dunn's comparisons.
Better understanding of pain and pain management
3.3.1.4
(a)Qualitative
The goal of the pain program was to increase participants' ability to reduce their pain and its impact. Following the interventions, one participant said, “Before I didn't know what to do to take away the pain or what to do to somewhat lessen the pain temporarily,” but now feel like they are able to understand and manage their pain better, which was echoed through interviews with other participants “It made me understand the pain more” and “Getting a broader understanding of my injury. Getting a broader understanding of just how the body process things, how the body heals, how the body try to.. Just the body itself is an amazing tool”. One participant noted, “I liked the exercise, the pain relief, the knowledge that I was able to gain from the study. Most of all, it was just learning how to deal with pain and manage pain”.
The results are likely an additive effect from the pain education, bodily illusion, and exercise, some participants highlighted the impact from the change in mindset “Let's just do it. Let's just see where it leads”, “it gets you up. It gets you going so you don't always feel defeated and depleted”, and “Power of the mind works really well,” and exercise “I learned different ways to manage a pain as far as exercising,” “When next woke up, I feel a little tight. After I finish working out, I feel great. My body feel loose” and “now I'll just stretch myself cause it makes it feel good”. Overall, participants felt that “The study emotionally gave me more awareness and the understanding of why the pain is bothering me” and “helped me learn that I can manage my pain”. Another benefit that came from this program was participants reporting that “things I couldn't easily handle or couldn't handle it at all before, now I'm handling them on the lower level” and that they were “Really, really happy for what happened to me now”. Although each participant has a unique, individualized pain, many participants expressed similar perspectives as this participant, “So I mean, the situation comes with chronic pain, there's no way, there's no if, ands or buts about it, but the more you can manage it, the better your daily life can be.”
- (b)Qualitative/Quantitative Participants reported a significant improvement in their ability to deal with pain χ^2^(3 = 16.14, p = 0.001; Kendall's W = .15) (Figure 6), as reflected in the question, “How difficult is it to deal with pain?”, with improvements maintained through week 15. Although the quantitative analysis of days with manageable pain did not reach significance, as shown in Figure 6B, there is a clear trend towards an increase in days with manageable pain throughout the pain program. Supporting this trend, participants gained “new tools” that “helped me manage the pain even more” and strategies that they could apply in their daily lives, “I am more able to process the pain on daily basis.”. For many, this program offered “other options and ways that I could try to manage or control the pain,” with one participant saying that they are “implementing a lot of what I learned to my daily activities now to help reduce the pain that I have.” Additionally, pain severity, a subscale of the Multidimensional Pain Inventory (MPI) (Figure 6C), showed a significant effect χ^2^(3 = 16.96, p < 0.0007; Kendall's W = .16), with a decrease from week 1 to weeks 11 and 15 and from week 5 to 11.
Participants responses to: (A) how difficult it is to deal with pain on a 0–10 scale; (B) how many days do you have manageable pain on a 0-7 scale; (C) overall pain severity, taken from the subscale of the MPI, throughout the 4 assessments in the pain program. P-values represented on the graph indicate Dunn's comparisons.
Reduced dependence on medication or external aids
3.3.1.5
Participants expressed that this program allowed them to utilize other pain management options other than medication and external aids, with participants stating that, “Before, I'd always be in a fetal position… now I do the workout instead” and that despite having “TENS unit, patches” available, “here I feel no pain” during exercise sessions, suggesting that the exercise circuit provided relief. One participant also noted that they began “taking a little less pain meds” as their “pain level was coming down,” throughout the pain program.
Barriers and limitations
3.3.2
Despite the positive outcomes reported by participants, there were barriers related to transportation, tiring interventions, lack of realism, negative impact from the walking illusion, other exercise preferences, triggering pain, already managing pain well, and temporary pain relief.
Transportation challenges
3.3.2.1
Transportation challenges represented the most significant obstacle, with participants noting, “The only thing is that I live an hour away. Just traveling there. Even though I like the workout part is I had to go twice a week and it was just a lot” and “the transportation was probably the hardest”.
Tiring/fatigue
3.3.2.2
Participants also noted that “the whole study was a little long”, which made it difficult to participate. For some participants, the exercise intervention was tiring, with some participants mentioning that they were “Just draining myself out” and “very tired after the exercises”.
Lack of connection and realism
3.3.2.3
The walking illusion intervention faced some barriers that may have limited its impact. A primary challenge was participants' inability to maintain a connection with the illusion, with many experiencing cognitive disconnection from the virtual representation. As participants described, “Don't feel like those are my legs” and “Hard to convince yourself that you're walking when you're just looking,” highlighting the difficulty in achieving embodiment of the virtual limbs. Participants perceived the intervention as lacking utility or realism, expressing that it “Didn't feel like it was too useful” and “Doesn't do much.” and “trying to elude myself into believing that these could be my legs actually moving like this. Those are my hopes, those are my dreams, that's what I'm striving for. But in the moment I'm grounded with the reality that this is what I'm dealing with”. The intervention triggered emotional distress for some participants, evoking sadness and disappointment as one explained: “I want to say it's sad, because it reminds you of what you should be doing.”.
Other exercise preferences
3.3.2.4
The intensity and duration of exercise sessions sometimes exceeded participants' physical capacity, “Just draining myself out, not knowing my limitations”. Specific exercise equipment proved problematic for certain participants, they reported “Don't like the glider” and discomfort with “the rower”. Some exercises triggered or exacerbated existing pain conditions in some of the participants. Participants experienced anxiety about potential injury, with one stating “The risk for me was I would be sometimes scared of a certain movement or do something to hurt my back,” while others reported direct pain increases: “I was starting to feel lots of pain in my neck”; “some exercises in the study that were incorporated that aggravated my pain” and “end of the study my pain would be a little bit more flared up” suggesting that for some individuals, the exercise intervention may have been counterproductive to the primary goal of pain management.
Exacerbation or trigger of pain
3.3.2.5
Counterproductively, some participants experienced increased pain due to heightened focus on their paralyzed limbs, with one noting “Almost made my pain worse because I was just sitting there and thinking about moving my own legs. But then that made it hurt more” and “I was thinking about my pain more.” Additional physical discomfort also included motion sickness “I got a little motion sick”
Already managing pain well
3.3.2.6
A subset of participants felt that were already implementing the pain management strategies, as one participant expressed, “I've been managing the pain for so long already,” while another noted, “So though I learned ways to cope with my pain and how to manage it, I feel like I've been doing the same things on my own.”
Temporary pain relief
3.3.2.7
Additionally, the temporary pain relief posed a challenge for some participants, with one participant described this limitation by explaining that “while I'm exercising, yes, it was good, but then throughout the whole day, the other day, it's just pain again,”. These barriers indicate that while the program provided valuable benefits for many participants, future programs may need to incorporate more individualized pain management skills.
Discussion
4
The main objective of this mixed method study was to assess participants' perspectives on a non-pharmacological multimodal pain program in general and its effects on neuropathic pain. Participants reported multiple important benefits including positive effects on overall physical and mental health, engagement, and neuropathic pain and pain management. Importantly, these qualitative findings were congruent with statistically significant overall reductions in pain severity scores, improvement in psychosocial outcomes, and decreased pain interference with activities and mood scores.
In general, there has been an increased emphasis on multimodal therapeutic pain management (67–71). Multimodal programs focusing on chronic pain have utilized non-pharmacological interventions including pain education (50, 67, 72, 73), exercise (50, 72, 74–76), acupuncture (76), electrical stimulation (11, 14, 16, 20), bodily illusions (20, 26), virtual reality (77, 78), and cognitive behavioral therapies (50, 76, 79); individually or in combination. It appears that pain education is best utilized in combination with other treatment strategies (67, 73, 76). For example, programs incorporating only pain education found improvements in pain interference and depression (67) but when incorporated with other interventions, specific pain outcomes such as momentary pain (76) and pain interference (73), were significantly improved. Therefore, having an education resource and comprehensive knowledge of pain can impact participants perceptions of pain (50, 55. The initial phase of this study previously published (55), focused on pain education, likely significantly contributed to the overall positive results although only minimal effects on pain and psychosocial scores were observed directly after pain education. The perceived benefits of pain education included having a better understanding about pain, treatment options and self-management in general, learning from and interacting with peers, having a better understanding about pathophysiology of pain and being able to better communicate with healthcare providers, family, and friends. In addition, the pain education had a significant positive impact on participants difficulty in dealing with pain scores, supporting the idea that pain education can facilitate the adjustment to living with chronic pain after SCI and possibly reduce some of psychological distress associated with experiencing persistent neuropathic pain (80). Consistent with this idea, affective distress is known to be significantly linked to chronic pain that has a high impact on life after SCI (81) and therefore a reduction in pain impact is likely also reducing the emotional impact. Previous research has shown that a combination of perceived greater pain impact and limitations, difficult nature of pain, poor communication from provider, lower resilience, greater medication use, and younger age predicts greater difficulty in dealing with pain after SCI (82). This highlights both the complexity in not only underlying mechanisms of pain after SCI but also the intricate association with multiple psychosocial domains.
Many people with SCI-related neuropathic pain utilize multiple self-remedies to manage their pain effectively (83). In the present study, participants reported that they frequently managed their pain using distraction and shifting focus to something else. Distraction as a tool for managing pain has been reported in studies involving both SCI (82) and other chronic pain populations (84). Indeed, our results show that during both exercise and walking illusion, some participants noted that they gradually developed a skill where they mentally could distract themselves from their pain and redirect their focus to the present activity. These findings are consistent with other studies reporting significant reductions in both pain interference and pain-related anxiety following mindfulness (85, 86) and cognitive engagement (84) interventions. Additionally, coping skills have been shown to predict daily management of pain following SCI (83, 87, 88). This concurs with the positive reports of managing pain in the present study and the significant reductions in difficulty dealing with pain. Although number of days with manageable pain were not significantly increased post exercise and walking illusion, there was a trend towards having more days with manageable pain. The lack of significant improvement was probably related to the fact that a large proportion of our participants, despite experiencing moderate to severe neuropathic pain, felt that they had manageable pain every day already at the baseline assessment. Because of the refractory nature of neuropathic pain, making pain manageable is a more realistic goal than complete amelioration. However, the meaning of manageable pain in people with SCI varies widely among individuals. A recent study in SCI (49) found that manageable pain was generally characterized by moderate pain intensity, predictability, low interference with daily activities, and pain not requiring medication (87, 88).
Congruent with this, we found a significant improvement with pain interference across both qualitative reports and quantitative scores. Several participants reported that they were able to fill their calendar with activities and complete tasks without being limited by their pain, which was also supported by the significant decreases in pain interference scores. A reduction in pain interference with daily activity has a profound impact on QOL following SCI (89) and our results highlight the importance of reducing pain interference to improve daily functioning. Additionally, some participants reported having better sleep, which was supported by a slight non-significant average improvement in pain interference with sleep scores. The significant decrease in pain interference with mood was paralleled by some participants reported starting the day in a better mood than before.
Other benefits reported by some participants included that they felt as though they had newfound control of their life and expanded mindset regarding what they could do. Others felt that this allowed them to reduce the limitations they put on themselves. Along with the confidence to accomplish more, participants reported their own self-image improved. This has been shown to impact the success of pain self-management, due to participants motivation and readiness to change (90). Increased motivation and continuing to exercise after the end of the study was reported by most participants at the follow-up interview, with some emphasizing that the positive experience of participating in the study changed the way they viewed their future. These positive views were also supported by the retention of significant improvements at the follow-up assessments for NPSI total and sub scores, pain interference with activities, and difficulty dealing with pain.
It is widely accepted that social interactions and communication may influence individuals perceptions of pain and responsiveness to therapeutic interventions (91). Indeed, some participants noted the positive impact of the community and interpersonal connections throughout the program. In the SCI community, research supports that social support directly impacts QOL and can influence the negative effects of pain on QOL (92). For example, prior to the study, some participants reported feeling isolated due to their injury and emphasized the significant and positive impact of connecting with others with SCI during the study and valued the opportunity to exchange knowledge and resources with each other.
Finally, although our study combined exercise and walking illusion, we believe that exercise had some specific beneficial effects. Specific to the exercise intervention, some participants noted that their increase in strength and stamina had an overall health impact. Beyond the noticeable change in upper-extremity strength, participants noticed an improvement in core strength, which allowed them to maintain better posture and have better balance throughout the day. Other participants reported an improvement in their cardiovascular health, with two participants improving blood pressure and cholesterol levels. Participants also felt as though they benefited from the personalized exercise, with many reporting that they were able to push themselves and improve weight in subsequent weeks because of the adaptations and instructions provided at the beginning of the intervention. Previous studies have shown that exercise has a wide range of beneficial effects for people with SCI (93). However, the optimal level of intensity, duration, and type of exercise specifically for pain management still being debated (75, 94). Upper limb circuit training has been shown to have significant improvements in strength, endurance, cardiometabolic markers, and pain outcomes (58, 95, 96). Several studies in SCI highlight the benefits of exercise on cardiometabolic health (97–100); which was consistent with lower blood pressure and cholesterol levels mentioned by participants in the present study. However, some studies also report conflicting results regarding the effects of exercise on physiological and pain outcomes. For example, while some studies report improvements on QOL (101, 102), and pain outcomes in chronic pain populations (28–32), others show no clinically significant changes in QOL, physiological state (74), and pain outcomes (74). However, the results from the present study are consistent with literature supporting evidence that exercise-based interventions can lead to measurable improvements in pain. As mentioned earlier, our program included both exercise and walking illusion. This latter has previously been shown to reduce neuropathic pain intensity in SCI individuals, either alone (15) or in combination with tDCS (16, 20). However, these studies only focused on quantitative pain outcomes, mainly a reduction in pain intensity, and did not consider participants' perspectives on these types of interventions. In the present study we aimed to significantly expand on these prior studies and included extensive qualitative interviews exploring participants' perspectives on a wide range of aspects of the study. We show that some participants experienced the walking illusion as a convincing simulation of movement that enhanced bodily ownership and agency. The intervention also elicited relaxation and positive mood, with some participants continuing the imagery practice outside the sessions. However, some negative perspectives were also provided by participants. For instance, some participants reported that the illusion felt unrealistic or, in some cases, triggered negative emotions by highlighting their lost abilities. These reports open the way for improvement in future trials using similar non-invasive interventions.
In conclusion, the outcomes from the present study provide support for non-pharmacological approaches that can be combined with pharmacological treatments for pain when needed. With the wide range of positive benefits reported in the qualitative interviews and the significant improvements in pain outcomes, pain interference in daily activities, this multimodal pain program successfully helped some individuals manage their neuropathic pain. However, some barriers emerged. For instance, transportation was a frequently mentioned significant difficulty for the participation in the study. Therefore, future studies need to take into consideration at-home options for non-pharmacological treatments, in this way access to these types of programs can be beneficial also for those individuals unable to attend multiple study sessions in experimental settings. Additionally, some suggested the use of a more realistic walking illusion using virtual reality (VR). The use of VR has recently been utilized as a non-pharmacological intervention for neuropathic pain and chronic pain populations (77, 78, 103, 104) via the remapping of body representation (104) and distraction from pain (103). It would be beneficial to develop VR interventions that can be home-based and consider participants' preferences for enhanced realism. Future studies should therefore focus on individually targeted and integrated combinations of interventions to improve overall outcomes.
Although this pain program showed meaningful benefits, the study also presents some limitations that must be acknowledged. This study was adequately powered for qualitative analysis, it was not powered for quantitative analyses, and we did not include a comparison intervention. This means that while the sample size was sufficient to generate reliable themes from participants' interviews, the quantitative findings may not be robust enough to be generalized to a broader SCI population, and the missing comparison intervention may introduce some bias in the results. Our sample also included a larger percentage of male participants, and although this is representative of the SCI population in the US (105), this may present a limitation for the generalizability of the results to women with SCI. Additionally, we did not include individuals with mild neuropathic pain or those with severe depression, and this limits our understanding of whether these benefits also apply to individuals with mild pain or severe depression. Finally, we believe that future studies including multidimensional pain programs similar to ours may have a benefit on psychosocial aspects and although our participants reported changes in their mood in the qualitative interviews, we did not include a more comprehensive mood or psychosocial assessment that might have further supported these reports.
In conclusion, the combination of both qualitative data with pain outcome measures strongly supports the usefulness of the present non-pharmacological multimodal pain program for many who experience moderate to severe neuropathic pain long after injury.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Finnerup NB Norrbrink C Trok K Piehl F Johannesen IL Sørensen JC Phenotypes and predictors of pain following traumatic spinal cord injury: a prospective study. J Pain. (2014) 15(1):40–8. 10.1016/j.jpain.2013.09.00824268112 · doi ↗ · pubmed ↗
- 2Andresen SR Biering-Sørensen F Hagen EM Nielsen JF Bach FW Finnerup NB. Pain, spasticity and quality of life in individuals with traumatic spinal cord injury in Denmark. Spinal Cord. (2016) 54(11):973–9. 10.1038/sc.2016.4627067654 · doi ↗ · pubmed ↗
- 3Loh E Mirkowski M Agudelo AR Allison DJ Benton B Bryce TN The Can Pain SCI clinical practice guidelines for rehabilitation management of neuropathic pain after spinal cord injury: 2021 update. Spinal Cord. (2022) 60(6):548–66. 10.1038/s 41393-021-00744-z 35124700 PMC 9209331 · doi ↗ · pubmed ↗
- 4Cardenas DD Nieshoff EC Suda K Goto SI Sanin L Kaneko T A randomized trial of pregabalin in patients with neuropathic pain due to spinal cord injury. Neurology. (2013) 80(6):533–9. 10.1212/WNL.0b 013e 318281546 b 23345639 PMC 3589291 · doi ↗ · pubmed ↗
- 5Onakpoya IJ Thomas ET Lee JJ Goldacre B Heneghan CJ. Benefits and harms of pregabalin in the management of neuropathic pain: a rapid review and meta-analysis of randomised clinical trials. BMJ Open. (2019) 9(1):e 023600. 10.1136/bmjopen-2018-02360030670513 PMC 6347863 · doi ↗ · pubmed ↗
- 6Polat CS Konak HE AkıncıMG Onat SS Altas EU. Misuse of gabapentinoids (pregabalin and gabapentin) in patients with neuropathic pain related to spinal cord injury. J Spinal Cord Med. (2023) 46(5):859–64. 10.1080/10790268.2021.202470935108174 PMC 10446779 · doi ↗ · pubmed ↗
- 7Widerstrom-Noga E Anderson KD Perez S Martinez-Arizala A Calle-Coule L Fleming L. Barriers and facilitators to optimal neuropathic pain management: s CI consumer, significant other, and health care provider perspectives. Pain Med Malden Mass. (2020) 21(11):2913–24. 10.1093/pm/pnaa 05832219441 · doi ↗ · pubmed ↗
- 8Kesikburun S. Non-invasive brain stimulation in rehabilitation. Turk J Phys Med Rehabil. (2022) 68(1):1–8. 10.5606/tftrd.2022.1060835949977 PMC 9305642 · doi ↗ · pubmed ↗