Junctional Failures Following Long-Level Fusion to L5 in Elderly Patients: Impact of Spinopelvic Alignment and L5–S1 Disc Degeneration
In-Seok Son, Yong-Chan Kim, Sung-Min Kim, Xiongjie Li, Maolin Jin, Young-Jik Lee, Seung-Hyun Sim, Kee-Yong Ha

TL;DR
This study examines why spinal fusions ending at L5 in elderly patients often lead to junctional failures, finding that spinal alignment is more important than disc degeneration.
Contribution
The study clarifies the relative impact of spinopelvic alignment versus L5–S1 disc degeneration on junctional failure patterns after long spinal fusion.
Findings
Lower L5–S1 disc degeneration is more associated with proximal junctional failure (PJF), while higher degeneration is linked to distal junctional failure (DJF).
Preoperative thoracolumbar kyphosis and T1 pelvic angle are significant risk factors for PJF.
Postoperative proximal junctional angle and lumbar lordosis are independently associated with DJF.
Abstract
Background and Objectives: Long spinal fusion terminating at L5 remains controversial because of the risk of postoperative junctional failure. Although degeneration of the residual L5–S1 disc has been suggested as a contributing factor, the relative impact of disc degeneration versus sagittal spinopelvic alignment on different junctional failure patterns has not been fully clarified. Materials and Methods: This retrospective cohort study included 47 patients aged ≥60 years who underwent ≥5-level thoracolumbar fusion ending at L5 with a minimum follow-up of 2 years. Junctional failures were classified as proximal junctional failure (PJF) or distal junctional failure (DJF). Preoperative L5–S1 disc degeneration was assessed using modified Weiner and Pfirrmann classifications. Spinopelvic parameters were measured preoperatively, postoperatively, and at final follow-up. Junctional…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
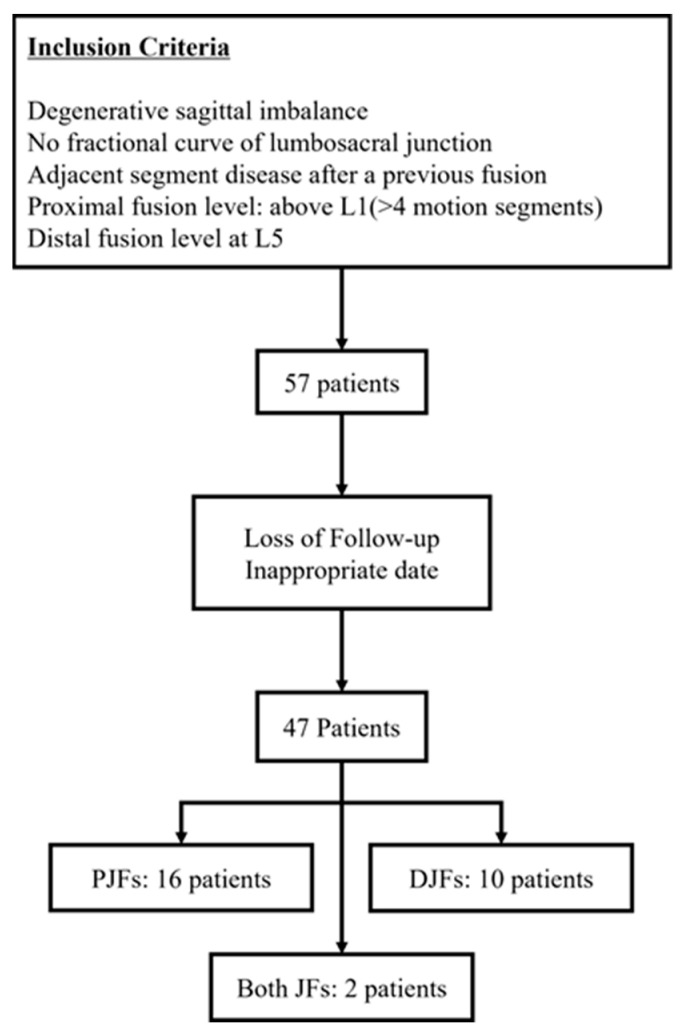 Figure 1
Figure 1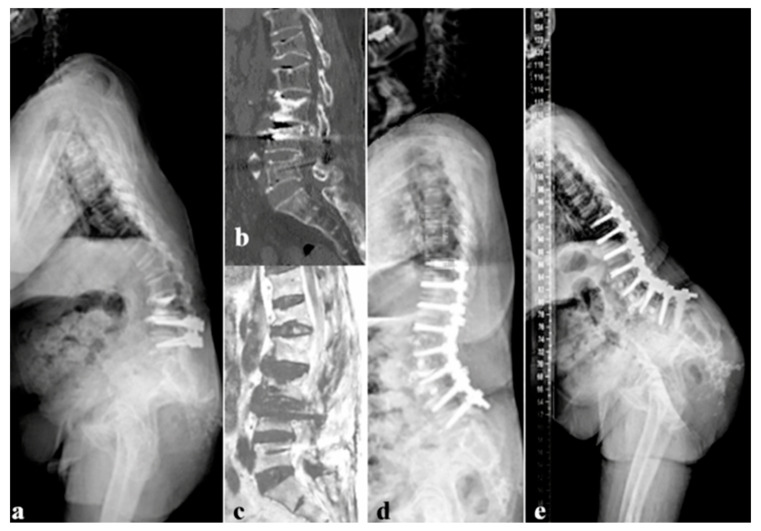 Figure 2
Figure 2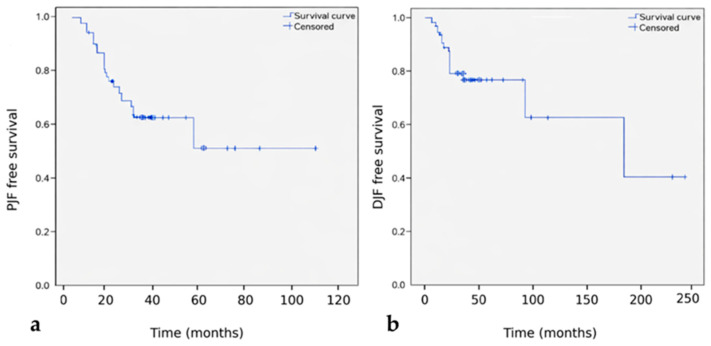 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Scoliosis diagnosis and treatment · Cervical and Thoracic Myelopathy
1. Introduction
Long spinal fusion is a well-established surgical strategy for the correction of adult spinal deformity (ASD); however, the choice of the distal fusion level remains controversial. In particular, whether to terminate a long construct at L5 or extend fixation to the sacrum continues to be debated, especially in elderly patients with degenerative pathology. While fusion to L5 preserves lumbosacral motion and may reduce surgical invasiveness, it also exposes the remaining L5–S1 segment to increased mechanical stress, potentially leading to postoperative sagittal decompensation and junctional failure [1,2,3,4].
Postoperative sagittal decompensation following long fusion can manifest as mechanical failure at different locations, including proximal junctional failure (PJF), distal junctional failure (DJF), or intra-construct complications such as rod fracture and pseudarthrosis [5,6,7]. Although risk factors for proximal junctional kyphosis and failure have been extensively investigated, distal junctional failure after fusion ending at L5 remains less well understood and has been relatively underreported. Systematic reviews have demonstrated a wide range in the incidence of distal junctional kyphosis and failure, largely depending on follow-up duration and patient characteristics [8].
Degeneration of the residual L5–S1 disc has been proposed as a key contributor to distal mechanical complications following long fusion terminating at L5. Previous studies have reported substantial rates of progressive disc degeneration and subsequent reoperation at the lumbosacral junction after long constructs stopping at L5 [1,2,9]. However, the relationship between preoperative disc degeneration and the specific pattern of junctional failure—proximal versus distal—has not been clearly defined. In addition, preserved segmental motion at a relatively healthy L5–S1 disc may paradoxically increase mechanical stress transfer to adjacent junctions after fusion, as motion and mechanical load may be concentrated at the transition zone between the rigid long construct and the remaining mobile lumbosacral segment, potentially influencing failure patterns [2,4]. This paradox arises because a rigid long construct can concentrate motion and mechanical load at the remaining mobile L5–S1 segment, creating a stress transition zone that may increase biomechanical demand at adjacent junctions.
Beyond disc degeneration, sagittal spinopelvic alignment plays a critical role in postoperative mechanical stability following long spinal fusion. Parameters such as pelvic incidence–lumbar lordosis (PI–LL) mismatch, global sagittal balance, and thoracolumbar kyphosis have been consistently reported to influence mechanical complications after long fusion procedures [10,11,12]. However, despite these observations, few studies have simultaneously evaluated the relative contributions of residual L5–S1 disc degeneration and sagittal alignment parameters to both proximal and distal junctional failure patterns in patients undergoing long fusion terminating at L5 [13,14].
Therefore, the purpose of this study was to identify risk factors for junctional failure following long thoracolumbar fusion ending at L5, with particular emphasis on the interaction between preoperative L5–S1 disc degeneration and sagittal spinopelvic alignment. We further sought to clarify whether distinct radiographic and biomechanical profiles are associated with proximal versus distal junctional failure patterns in this patient population.
2. Materials and Methods
2.1. Study Design and Patient Selection
This retrospective cohort study was conducted at a single tertiary referral center and reviewed consecutive elderly patients who underwent long thoracolumbar fusion terminating at L5 between January 2010 and December 2020. Long fusion was defined as fixation involving five or more vertebral levels, with the uppermost instrumented vertebra located at or above L1 and L5 as the lowest instrumented vertebra.
Inclusion criteria were as follows: (1) age ≥60 years at the time of surgery; (2) minimum follow-up duration of 24 months; (3) fusion length of ≥5 levels terminating at L5; (4) circumferential fusion performed at L4–L5; and (5) absence of a significant fractional lumbosacral curve in patients with degenerative lumbar scoliosis. Exclusion criteria included (1) previous decompression or fusion at L5–S1; (2) sacralization of L5; (3) spontaneous fusion of the L5–S1 segment caused by advanced osteophyte formation; (4) neuromuscular, congenital, infectious, traumatic, or neoplastic spinal disorders; and (5) incomplete radiographic or clinical follow-up.
Among 57 initially screened patients, 47 met all inclusion criteria and were included in the final analysis (Figure 1). Indications for surgery included degenerative lumbar scoliosis, degenerative sagittal imbalance, multilevel spinal stenosis, or revision surgery for adjacent segment degeneration with sagittal imbalance.
2.2. Surgical Procedure
All surgeries were performed via a posterior approach with segmental pedicle screw instrumentation. Long-segment fusion terminating at L5 was performed according to the extent of deformity and clinical symptoms.
Anterior column support at the L4–L5 level was selectively employed when additional segmental stability or sagittal correction was required, and circumferential fusion at L4–L5 was routinely performed to enhance distal fixation strength.
Sagittal alignment correction was achieved using posterior column osteotomies and rod contouring as needed, based on individual deformity characteristics. Sagittal correction strategies were individualized rather than standardized, considering patient age, baseline sagittal alignment, and overall clinical condition, rather than applying a uniform alignment target across all patients.
2.3. Radiographic Evaluation
Standing full-length anteroposterior and lateral radiographs were obtained preoperatively, within one month postoperatively, and at the final follow-up. Radiographic parameters included pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), lumbar lordosis (LL), thoracolumbar kyphosis (TLK), thoracic kyphosis (TK), C7 sagittal vertical axis (SVA), T1 pelvic angle (T1PA), proximal junctional angle (PJA), and distal junctional angle (DJA). DJA was defined as the angle between the inferior endplate of L5 and the superior endplate of S1.
All radiographic measurements were independently performed by two fellowship-trained spine surgeons who were blinded to clinical outcomes. Interobserver discrepancies were resolved through joint review, and consensus values were used for analysis
2.4. Assessment of L5–S1 Disc Degeneration
Preoperative L5–S1 disc degeneration was evaluated using lateral radiographs according to the modified Weiner classification and magnetic resonance imaging (MRI) using the Pfirrmann grading system [11,12]. In cases of discordance between radiographic and MRI-based assessments, computed tomography was additionally reviewed. Final grading was determined by consensus among all authors. A representative case of distal junctional failure is shown in Figure 2.
2.5. Definition and Classification of Junctional Failure (Revised)
Proximal junctional kyphosis (PJK) was defined radiographically as a proximal junctional angle (PJA) greater than 10° and at least 10° greater than the preoperative measurement [15]. Proximal junctional failure (PJF) was diagnosed when PJK was accompanied by clinical symptoms and structural failure, including fracture of the upper instrumented vertebra (UIV) or UIV+1, junctional subluxation, implant loosening or breakage at the proximal junction, or the development of new neurological deficits requiring medical or surgical intervention [15,16].
Distal junctional kyphosis (DJK) was defined as a postoperative distal junctional angle (DJA) greater than 10° or an increase of more than 10° compared with the immediate postoperative measurement [17]. Distal junctional failure (DJF) was defined as symptomatic DJK associated with structural failure at the distal junction, including fracture of the L5 vertebra (lowest instrumented vertebra), loosening or pull-out of distal pedicle screws, rod or screw breakage, or progressive distal instability requiring revision surgery [8,17].
The proximal junctional angle (PJA) was measured between the inferior endplate of the upper instrumented vertebra and the superior endplate of the vertebra two levels above. The distal junctional angle (DJA) was measured between the inferior endplate of L5 and the superior endplate of S1.
Patients were classified into three groups according to the type of junctional failure observed during follow-up: no junctional failure, PJF, and DJF. Patients who developed both PJF and DJF were analyzed separately when appropriate.
2.6. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 21.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation and compared using the Kruskal–Wallis test, with post hoc pairwise comparisons performed using the Mann–Whitney U test with Bonferroni correction. Categorical variables were analyzed using Fisher’s exact test or the linear-by-linear association test, as appropriate.
Junctional failure–free survival was analyzed using the Kaplan–Meier method, and differences between groups were assessed using the log-rank test. Variables with a p-value < 0.10 in univariate analysis were entered into a multivariate Cox proportional hazards regression model to explore independent risk factors for PJF and DJF. Given the retrospective design and limited number of junctional failure events, multivariate Cox regression analyses were performed in an exploratory manner, and the results were interpreted with caution. A two-sided p-value < 0.05 was considered statistically significant.
3. Results
3.1. Patient Demographics and Surgical Characteristics
A total of 47 patients met the inclusion criteria and were included in the analysis. The mean age was 70.6 ± 5.7 years, and 37 patients (78.7%) were female. The mean body mass index was 24.1 ± 3.5 kg/m^2^, and the mean follow-up duration was 48.7 ± 43.9 months. The average number of fused levels was 6.2 ± 1.4 (range, 5–10).
Among the cohort, 28 patients (59.6%) developed junctional failure during follow-up, whereas 19 patients (40.4%) did not. Proximal junctional failure (PJF) occurred in 16 patients (34.0%), distal junctional failure (DJF) in 10 patients (21.3%), and both PJF and DJF in 2 patients (4.3%). There were no significant differences among the normal, PJF, and DJF groups in terms of age, sex distribution, body mass index, bone mineral density, or fusion length (Table 1).
3.2. Association Between Junctional Failure and Revision Surgery
Twenty-seven patients (57.4%) underwent primary index surgery, whereas 20 patients (42.6%) had a history of prior floating lumbar fusion. Junctional failure developed in 15 patients (55.6%) after primary surgery and in 12 patients (60.0%) following revision surgery.
Although distal junctional failure was more frequently observed in the revision surgery group than in the primary surgery group (35.0% vs. 18.5%), the overall distribution of junctional failure types did not differ significantly according to revision status (p = 0.300, Table 2).
3.3. Relationship Between Junctional Failure and L5–S1 Disc Degeneration
Preoperative L5–S1 disc degeneration, assessed using the modified Weiner classification, showed a statistically significant difference in distribution among junctional failure patterns (p = 0.024, Table 2). Among patients with minimal disc degeneration (Weiner grades 0–1), proximal junctional failure was more prevalent than distal junctional failure. In contrast, patients with moderate degeneration (grade ≥ 2) more frequently developed distal junctional failure.
Similarly, Pfirrmann grading based on magnetic resonance imaging demonstrated a significant difference in degeneration severity among the groups (p = 0.044). Higher Pfirrmann grades were more commonly observed in patients who developed distal junctional failure compared with those without junctional failure or with proximal failure.
3.4. Comparison of Spinopelvic Parameters Among Groups
Preoperative spinopelvic parameters were largely comparable among the three groups, except for thoracolumbar kyphosis (TLK) and proximal junctional angle (PJA), which differed significantly between the PJF and DJF groups. Preoperative T1 pelvic angle was significantly greater in the PJF group compared with patients without junctional failure.
At one month postoperatively, thoracic kyphosis and proximal junctional angle were significantly greater in the PJF group than in the DJF group. At the final follow-up, patients with junctional failure demonstrated significantly greater sagittal vertical axis and T1 pelvic angle values compared with patients without junctional failure. Detailed comparisons of radiographic parameters are summarized in Table 3.
3.5. Junctional Failure–Free Survival and Risk Factor Analysis
Kaplan–Meier survival analysis demonstrated that proximal junctional failure occurred earlier and more frequently than distal junctional failure (Figure 3). At one year postoperatively, the cumulative incidence of PJF and DJF was 14.9% and 8.5%, respectively. At two years, these values increased to 34.0% for PJF and 19.1% for DJF.
Multivariate Cox proportional hazards regression showed that preoperative thoracolumbar kyphosis, preoperative T1 pelvic angle, and postoperative pelvic incidence–lumbar lordosis mismatch were associated with proximal junctional failure. Postoperative proximal junctional angle and lumbar lordosis were associated with distal junctional failure (Table 4).
3.6. Reoperation Due to Junctional Failure
Nine of the 28 patients with junctional failure (32.1%) required reoperation, representing 19.1% of the entire cohort. Reoperation was more commonly performed for proximal junctional failure than for distal junctional failure. No patient underwent revision surgery solely for distal junctional failure without concomitant proximal pathology (Figure 4).
4. Discussion
The present study evaluated risk factors for junctional failure following long thoracolumbar fusion terminating at L5, with particular emphasis on the relative contributions of residual L5–S1 disc degeneration and sagittal spinopelvic alignment. The principal finding is that sagittal alignment parameters appear to play a more prominent role in both the occurrence and pattern of junctional failure than preoperative disc degeneration at L5–S1. Furthermore, proximal and distal junctional failures demonstrated distinct radiographic and biomechanical profiles, supporting the concept that these entities represent different modes of postoperative mechanical failure rather than a single continuous spectrum [1,3,4,5,6,7].
The decision to terminate a long fusion at L5 or extend fixation to the sacrum remains one of the most debated issues in adult spinal deformity surgery, particularly in elderly patients [1,3,4]. Fusion stopping at L5 preserves lumbosacral motion and may reduce operative time, blood loss, and perioperative morbidity; however, it also places substantial mechanical demands on the remaining L5–S1 segment. Previous studies have reported variable rates of postoperative sagittal decompensation and reoperation following long fusion to L5, underscoring the need to better define patient- and alignment-specific risk factors [1,2,4,9]. From a clinical decision-making perspective, our findings suggest that elderly patients with pronounced sagittal imbalance, such as elevated preoperative T1 pelvic angle or residual postoperative PI–LL mismatch, may be suboptimal candidates for fusion terminating at L5. In such cases, extension of fixation to the sacrum or ilium should be considered to enhance mechanical stability and reduce the risk of junctional failure.
In the current cohort, preoperative L5–S1 disc degeneration was significantly associated with the pattern of junctional failure. Patients with minimal degeneration (modified Weiner grades 0–1) more frequently developed proximal junctional failure, whereas those with more advanced degeneration (grade ≥ 2) were more likely to experience distal junctional failure. Similar trends have been reported by Witiw et al. [4], who demonstrated that preserved L5–S1 disc integrity was associated with a higher incidence of proximal junctional pathology, whereas advanced degeneration increased the risk of distal failure. These findings may suggest that a relatively mobile lumbosacral segment may contribute to increased stress transfer to the proximal junction following long fusion, whereas structural compromise at L5–S1 predisposes patients to distal mechanical breakdown. From a long-term perspective, these findings highlight a trade-off between preserving L5–S1 motion and ensuring mechanical stability in long-segment fusion. While motion preservation may be advantageous in selected patients, a relatively mobile lumbosacral junction can increase stress transfer to the proximal junction in certain sagittal alignment contexts; therefore, the decision to preserve or sacrifice L5–S1 should be individualized.
Despite this association, disc degeneration alone did not fully account for junctional failure occurrence. In our study, sagittal spinopelvic alignment parameters were more consistently associated with mechanical failure than disc degeneration. Preoperative thoracolumbar kyphosis and T1 pelvic angle, as well as postoperative pelvic incidence–lumbar lordosis (PI–LL) mismatch, were independently associated with proximal junctional failure. These findings are consistent with prior studies demonstrating that insufficient restoration of sagittal alignment increases proximal stress concentration and predisposes patients to junctional collapse [10,16].
Distal junctional failure demonstrated a different risk profile. Postoperative proximal junctional angle and lumbar lordosis were independently associated with DJF, suggesting that distal failure is closely related to residual sagittal imbalance and local junctional mechanics rather than preoperative disc status alone. Previous biomechanical and clinical studies have shown that inadequate lumbar lordosis correction, particularly in patients with high pelvic incidence, results in increased shear and bending moments at the distal end of long constructs [14,18,19]. Our findings support these observations and highlight the importance of achieving appropriate global and segmental alignment when selecting L5 as the distal fusion level. Although specific age-adjusted alignment thresholds could not be established in the present study, these findings support the concept that sagittal correction goals in elderly patients should be individualized according to patient age and baseline alignment rather than applying a uniform target. Future studies are warranted to determine whether age-adjusted parameters, such as PI–LL mismatch or T1 pelvic angle thresholds, may further reduce the risk of junctional failure.
The angle thresholds used to define proximal and distal junctional kyphosis in this study were based on widely accepted and validated criteria. Proximal junctional kyphosis was defined as a proximal junctional angle exceeding 10° and increasing by more than 10° relative to the preoperative value, as originally described by Glattes et al. [15]. Distal junctional kyphosis was defined using similar angular criteria, consistent with definitions proposed in previous studies evaluating distal junctional pathology and mechanical failure [17,18]. These thresholds have been adopted in multiple large series and systematic reviews, providing a reproducible framework for distinguishing clinically meaningful junctional deformity from expected postoperative alignment changes [8,17].
Measurement reliability is a critical consideration when evaluating sagittal alignment and junctional angles. In the present study, all radiographic parameters were independently assessed by two fellowship-trained spine surgeons who were blinded to clinical outcomes. Interobserver agreement was high, with intraclass correlation coefficients exceeding 0.80 for all key sagittal alignment parameters. This level of reliability is comparable to that reported in previous alignment-focused studies and minimizes the likelihood that observer variability influenced the observed associations [15].
Interestingly, although a deep-seated L5 vertebra has been biomechanically implicated as a potential contributor to increased stress concentration at the lumbosacral junction, no significant association was observed between intercristal line position and junctional failure in this cohort. This finding suggests that global sagittal alignment may outweigh local anatomical variations in determining postoperative mechanical outcomes. Similar conclusions have been reported in studies emphasizing alignment-based surgical planning over isolated anatomical factors [10,13,14].
Several limitations of this study should be acknowledged. First, the retrospective design and relatively small sample size, particularly after subdivision into multiple junctional failure patterns, may limit statistical power and increase the risk of type I error and overfitting in multivariable Cox regression analyses. Second, the absence of a control group undergoing fusion to the sacrum precludes direct comparison between distal fusion strategies and limits determination of whether the observed junctional failure patterns are specific to fusion terminating at L5 or reflect a general consequence of long spinal fusion in elderly patients. Third, assessment of L5–S1 disc degeneration relied on integration of radiographic, MRI, and selectively CT-based evaluations with final author consensus, without formal quantitative assessment of inter-method reliability, and disc degeneration was treated as a static variable without evaluation of its temporal progression. Fourth, interpretation of sagittal alignment parameters may be limited by modest statistical significance in some intergroup comparisons, lack of correction for multiple comparisons, and potential multicollinearity among biomechanically related variables. Lastly, potentially confounding factors such as bone quality, construct stiffness, osteotomy techniques, and proximal reinforcement strategies were not systematically analyzed, and although the mean follow-up duration exceeded four years, longer-term follow-up may be required to fully capture late-onset junctional failures. Accordingly, the present findings should be interpreted as exploratory and hypothesis-generating rather than definitive evidence.
5. Conclusions
Sagittal spinopelvic alignment parameters appear to play a more prominent role in junctional failure patterns than residual L5–S1 disc degeneration in long spinal fusions ending at L5. Proximal and distal junctional failures represent distinct mechanical entities with different radiographic and biomechanical risk profiles. Careful preoperative assessment and adequate restoration of sagittal alignment should be prioritized when selecting L5 as the distal fusion level.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Edwards C.C.2nd Bridwell K.H. Patel A. Rinella A.S. Berra A. Lenke L.G. Long adult deformity fusions to L 5 and the sacrum. A matched cohort analysis Spine 2004291996200510.1097/01.brs.0000138272.54896.3315371700 · doi ↗ · pubmed ↗
- 2Jia F. Wang G. Liu X. Li T. Sun J. Comparison of long fusion terminating at L 5 versus the sacrum in treating adult spinal deformity: A meta-analysis Eur. Spine J.202029243510.1007/s 00586-019-06187-831624908 · doi ↗ · pubmed ↗
- 3Sardar Z.M. Ouellet J.A. Fischer D.J. Skelly A.C. Outcomes in adult scoliosis patients who undergo spinal fusion stopping at L 5 compared with extension to the sacrum Evid. Based Spine Care J.201349610410.1055/s-0033-135736024436707 PMC 3836950 · doi ↗ · pubmed ↗
- 4Witiw C.D. Fessler R.G. Nguyen S. Mummaneni P. Anand N. Blaskiewicz D. Uribe J. Wang M.Y. Kanter A.S. Okonkwo D. Re-operation After Long-Segment Fusions for Adult Spinal Deformity: The Impact of Extending the Construct Below the Lumbar Spine Neurosurgery 20188221121910.1093/neuros/nyx 16328472486 · doi ↗ · pubmed ↗
- 5Edwards C.C.2nd Bridwell K.H. Patel A. Rinella A.S. Jung Kim Y. Berra A.B. Della Rocca G.J. Lenke L.G. Thoracolumbar deformity arthrodesis to L 5 in adults: The fate of the L 5-S 1 disc Spine 2003282122213110.1097/01.BRS.0000084266.37210.8514501924 · doi ↗ · pubmed ↗
- 6Kuhns C.A. Bridwell K.H. Lenke L.G. Amor C. Lehman R.A. Buchowski J.M. Edwards C.2nd Christine B. Thoracolumbar deformity arthrodesis stopping at L 5: Fate of the L 5-S 1 disc, minimum 5-year follow-up Spine 2007322771277610.1097/BRS.0b 013e 31815 a 7ece 18007259 · doi ↗ · pubmed ↗
- 7Park H.Y. Kim Y.H. Kim S.I. Han S.B. Ha K.Y. Two different types of postoperative sagittal imbalance after long instrumented fusion to the sacrum for degenerative sagittal imbalance J. Neurosurg. Spine 20203361362210.3171/2020.4.SPINE 2015332590350 · doi ↗ · pubmed ↗
- 8Mc Donnell J.M. Ahern D.P. Wagner S.C. Morrissey P.B. Kaye I.D. Sebastian A.S. Butler J.S. A Systematic Review of Risk Factors Associated with Distal Junctional Failure in Adult Spinal Deformity Surgery Clin. Spine Surg.20213434735410.1097/BSD.000000000000122434232153 · doi ↗ · pubmed ↗