Polymicrobial Late-Onset Knee Prosthetic Joint Infection Involving Parvimonas micra: A Case Report and Genomic Characterization
Mauro Jose Salles, Daniel Litardi Pereira, Ícaro Santos Oliveira, Fabiano Nunes Farias, Rafaela Carvalho Luz, Paola Cappellano, André Mário Doi, Raquel Bandeira da Silva

TL;DR
A rare case of knee prosthetic joint infection involving Parvimonas micra and Staphylococcus aureus is reported, with genomic insights into the pathogen's virulence and treatment outcomes.
Contribution
This case highlights the overlooked role of Parvimonas micra in chronic prosthetic joint infections and provides genomic characterization of its virulence traits.
Findings
The P. micra strain showed 97.2% identity to a reference strain and carried virulence genes like groEL, tufA, clpP, and gaIE.
Resistance genes vanW, vanT, and vanY were detected, but vanA and vanB were absent.
The patient's symptoms resolved after two-stage revision surgery and targeted antimicrobial therapy.
Abstract
We report a rare case of polymicrobial late-onset knee prosthetic joint infection (PJI) caused by Parvimonas micra and Staphylococcus aureus. An 80-year-old woman with multiple comorbidities presented, five years after total knee arthroplasty, with progressive pain and radiographic signs of prosthetic loosening. Synovial fluid analysis revealed marked neutrophilic inflammation, and intraoperative tissue cultures, including sonication fluid yielded both pathogens. Identification was confirmed by MALDI-TOF MS and whole-genome sequencing (WGS). The P. micra strain showed 97.2% identity to reference strain SAMN29629855, and carried virulence genes such as groEL, tufA, clpP, ctrD, srtC4, and gaIE, associated with oxidative stress response, adhesion, immune evasion, and biofilm formation. Resistance genes vanW, vanT, and vanY from the van operon were also detected, though vanA and vanB were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
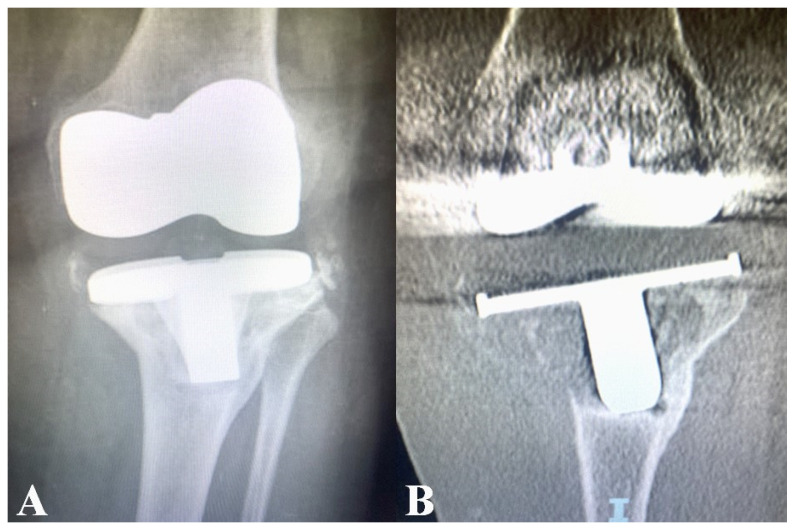 Figure 1
Figure 1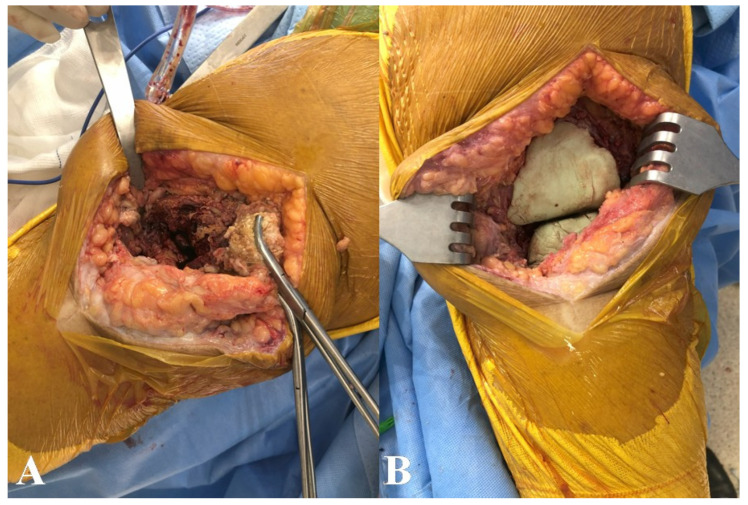 Figure 2
Figure 2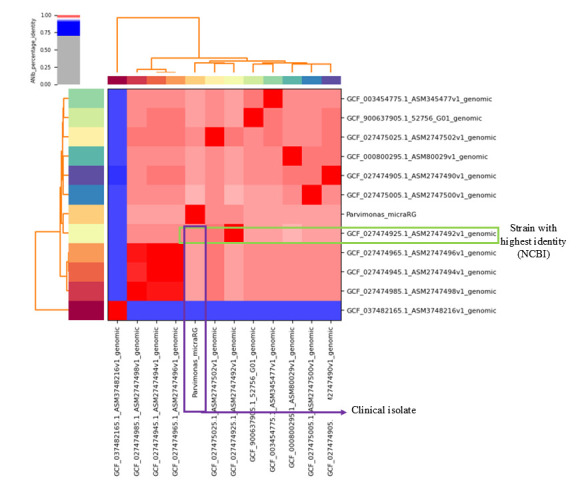 Figure 3
Figure 3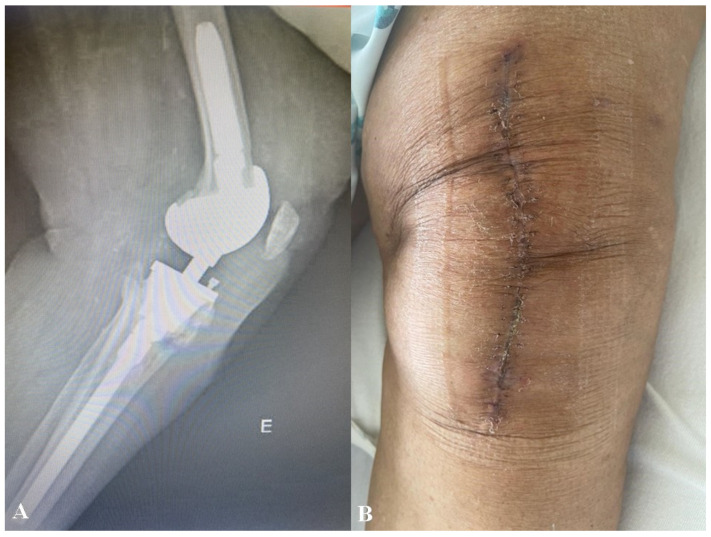 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Bacterial Identification and Susceptibility Testing · Infective Endocarditis Diagnosis and Management
1. Introduction
Prosthetic joint infections (PJIs) remain the leading postsurgical complication, affecting up to 2% of primary and 4% of revision arthroplasties, profoundly impacting patients’ quality of life, increasing healthcare costs, and posing significant challenges to the management of implant-related infections [1,2,3].
The incorporation of advanced microbiological identification technologies has provided critical means to optimize clinical outcomes and resource utilization, thereby contributing to a reduction in adverse events in empirical therapy and mortality [4,5,6,7]. In this context, often overlooked or underrecognized anaerobic bacteria—such as Cutibacterium acnes, Finegoldia magna, Fusobacterium spp., Prevotella spp, and Parvimonas micra—are increasingly being recognized as true pathogens in PJIs [8]. Prosthetic joint infections associated with microorganisms of oral origin are uncommon and represent only a small subset of PJIs. A systematic review identified just 44 reported cases of PJIs temporally associated with dental procedures over several decades, with anaerobic Gram-positive bacteria from the oral microbiota accounting for approximately 18% of isolated pathogens, highlighting both the rarity and the likely underrecognition of these organisms [9]. We report on the case of an elderly patient who developed a late-onset total knee arthroplasty (TKA) coinfection involving Staphylococcus aureus and P. micra. Comprehensive whole-genome sequencing (WGS) and phenotypic characterization of P. micra were performed to elucidate its clonality and pathogenic potential, including adhesion, intracellular invasion, biofilm formation, and antimicrobial resistance mechanisms within the framework of PJI. This study was reviewed and approved by the Research Ethics Committee (CEP) of Instituto Fleury/SP, Brazil, through Plataforma Brasil, and received ethical approval under Opinion Number 7.017.378 (CAAE: 77143523.0.0000.5474), confirming compliance with all applicable ethical standards for research involving human data.
2. Case Report
An 80-year-old female with a complex medical history—including active smoking, diabetes mellitus, atrial fibrillation, morbid obesity (BMI > 40), and a history of successfully treated breast cancer—presented with left knee osteoarthritis. She underwent TKA while exhibiting ongoing gingivitis, which was not considered clinically significant at the time. Three months after TKA, she underwent gastrectomy for the treatment of a perforated ulcer. Five years later, the patient presented with insidious left knee pain that had progressively become disabling, accompanied by radiographic findings suggestive of prosthetic loosening (Figure 1A,B).
Laboratory workup revealed a white blood cell count of 10,420/µL and a C-reactive protein level of 6.9 mg/L. Synovial fluid analysis demonstrated 51,195 leukocytes/µL, with 83% neutrophils. A two-stage revision surgery was performed. A polymethylmethacrylate (PMMA) spacer loaded with vancomycin and gentamicin was implanted (Figure 2A,B), and empirical intravenous ceftriaxone was initiated.
Intraoperative cultures of periprosthetic tissues and synovial and sonication fluids were processed using anaerobic culture in both solid and liquid media, yielding P. micra and S. aureus, both confirmed by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) and WGS (Figure 3). Synovial fluid cytology with white blood cell counts higher than 3000 cells/µL and a percentage of polymorphonuclear cells (PMN) higher than 80%, with the same pathogen yield in deep tissue and sonication fluid of the retrieved implant, supported that it represents a true pathogen rather than contamination, which confirms the diagnosis of PJI according to the European Bone and Joint Infection Society (EBJIS)’s PJI definition [10]. In addition, the P. micra susceptibility profile was confirmed by antimicrobial susceptibility testing (AST) using E-test and/or microdilution, providing MIC values (mg/L). The isolate demonstrated a fully susceptible anaerobic phenotype, with very low MICs to penicillin G ≤ 0.016 mg/L (S), metronidazole 0.047 mg/L (S), and clindamycin 0.19 mg/L (S). Antimicrobial susceptibility testing for Staphylococcus aureus was performed using a standard automated susceptibility testing system, with interpretation according to EUCAST criteria. The isolate was susceptible to all tested agents except penicillin, confirming methicillin susceptibility
Whole-genome sequencing was carried out with paired-end Illumina NextSeq550 platform with NextTera kit (Illumina, Inc., San Diego, CA, USA) producing 150 bp read fragments. Raw sequence data was submitted to metagenomic analysis software, Varsmetagen^®^ (v2.3, cloud-based pipeline), that carried a WGS pipeline for classification and generation of complete bacterial genomes. Briefly, a total of 3 million reads were filtered and classified with Kraken2 (Version v2.17.0) using a custom database. Reads were assembled with SPAdes v4.1 followed by a second round of classification with kraken2.
MetaWRAP (Version v1.3.2) was employed to group contigs into bins, which were subsequently classified as metagenome-assembled genomes (MAGs) using GTDB-Tk (GTDB R214). Over 1 million reads and 17 assembled sequences (contigs) were classified as Parvimonas micra. The final MAG had a total of 1.6 Mb, with a 248× depth coverage, and is available in GenBank (SAMN54754354).
After 12 weeks of targeted antimicrobial therapy, the PMMA spacer was removed, ceftriaxone was discontinued, and a revision prosthesis was successfully implanted. During 12 months of follow-up, the patient exhibited restored motor function and no evidence of infection recurrence (Figure 4).
3. Literature Review and Discussion
We describe the first polymicrobial chronic knee PJI caused by the association of biofilm-producing P. micra and S. aureus. Formerly known as Micromonas micros and Peptostreptococcus micros, P. micra is a slow-growing, fastidious, strictly anaerobic, Gram-positive coccus that colonizes the human gastrointestinal tract and is typically associated with periodontitis [11]. However, under certain conditions, it can transition into an invasive phenotype, leading to bacteremia associated with a variety of infections—including meningitis, central nervous system abscesses, panophthalmitis, endocarditis, pulmonary empyema, spondylodiscitis, osteomyelitis, pyomyositis, and native joint arthritis—and has also been implicated in colorectal oncogenesis [12,13,14,15,16,17,18,19,20,21,22,23].
The paucity of symptoms observed in the present case aligns with reports in the literature. A systematic review of P. micra infection routes found fever in fewer than 50% of reported cases, with nonspecific constitutional symptoms such as general malaise and anorexia being frequently noted. Pain was the most reported symptom, primarily associated with musculoskeletal inflammation [11]. Notably, only five cases of Parvimonas micra-related PJI following TKA have been reported in the literature to date [24,25,26,27,28]. To further illustrate the association between P. micra infection and arthroplasty, a comparative table summarizing clinical findings, diagnostic methods, and treatment strategies from reported cases is provided [24,25,26,27,28,29,30,31,32,33,34,35] (Table 1).
We speculate that distinct sources of P. micra and S. aureus contributed to the development of PJI, with chronic periodontitis or gut translocation serving as potential origins for the former, and nasal colonization for the latter [36]. Indeed, P. micra often exhibits mutualistic relationships with other bacteria within biofilms, including Porphyromonas gingivalis, Fusobacterium nucleatum, Actinomyces naeslundii, members of the order Enterobacterales, and various Streptococcus species [37,38,39,40]. These microbial communities, supported by an extracellular matrix primarily composed of exopolysaccharides and lipoteichoic acids, contribute to microbiome stability and pathogenic potential. As demonstrated by Liu et al., regulation of the dltA gene in P. micra modulates lipoteichoic acid expression within the biofilm matrix, directly influencing biofilm formation and bacterial growth [41].
Beyond the descriptive comparison of previously reported cases, the data summarized in Table 1 allow a deeper interpretation of the clinical behavior and pathogenic relevance of Parvimonas micra in PJI. The remarkably small number of documented cases, despite the widespread use of joint arthroplasty and the well-recognized prevalence of anaerobic bacteria within the human microbiota, strongly suggests that P. micra–associated PJIs are substantially underdiagnosed rather than genuinely rare. This discrepancy likely reflects a longstanding diagnostic bias towards aerobic and rapidly growing organisms, together with the limited routine use of prolonged anaerobic incubation, implant sonication, and molecular diagnostic techniques in many orthopedic centers [8].
The temporal evolution of reported cases further supports this interpretation. Earlier publications relied almost exclusively on conventional culture-based methods, often resulting in delayed or incomplete pathogen identification. In contrast, more recent studies increasingly incorporate advanced technologies such as MALDI-TOF MS, metagenomic sequencing, and whole-genome sequencing [27,31]. This shift mirrors broader developments in clinical microbiology and indicates that improved diagnostic resolution has played a pivotal role in recognizing P. micra as a true pathogen rather than an incidental or contaminant organism. Its repeated recovery from deep periprosthetic tissues [29,32], synovial fluid [25,26,27,28], and sonication fluid [30] across independent cases further substantiates its pathogenic significance.
Clinically, a consistent pattern of late-onset infection with indolent presentation emerges. Unlike acute PJIs caused by highly virulent organisms, P. micra infections typically manifest as isolated or progressive joint pain, functional decline, and radiological evidence of prosthetic loosening, frequently in the absence of systemic inflammatory features [31,35]. Such presentations increase the risk of misdiagnosis as aseptic failure and may delay appropriate microbiological investigation and definitive management. These observations underscore the importance of maintaining a high index of suspicion for anaerobic pathogens in cases of chronic prosthetic dysfunction, particularly in elderly patients and those with substantial comorbidities that may predispose them to haematogenous seeding or impaired immune responses.
From a therapeutic perspective, published cases indicate that P. micra remains largely susceptible to commonly used anti-anaerobic agents, including β-lactams, clindamycin, and metronidazole. The absence of clinically relevant resistance is consistent with existing microbiological data and supports the effectiveness of targeted antimicrobial therapy once the organism is accurately identified. Nevertheless, the frequent requirement for revision surgery, especially two-stage exchange procedures in late-onset infections, highlights the central role of biofilm formation and implant-associated persistence in disease pathogenesis. These findings reinforce the principle that surgical decision-making should be driven primarily by infection chronicity, implant stability, and host-related factors rather than antimicrobial susceptibility alone [1].
An additional challenge arises from the polymicrobial potential of P. micra, which may further complicate both diagnosis and management. Anaerobic cocci are known to engage in synergistic interactions within polymicrobial biofilms, enhancing microbial survival, immune evasion, and tissue destruction. In this context, failure to detect P. micra may result in incomplete pathogen coverage and suboptimal antimicrobial strategies. The selective integration of molecular diagnostics into routine workflows may therefore not only improve detection rates but also strengthen antimicrobial stewardship by enabling more precise, pathogen-directed therapy [8].
Regarding clinical outcome, most reported patients achieved favorable results following appropriate surgical and antimicrobial intervention. Infection resolution was commonly attained through adequate surgical source control combined with prolonged, targeted antimicrobial therapy. Recurrence was rarely reported, and adverse outcomes, when present, were predominantly related to host factors such as advanced age or cardiovascular comorbidities rather than microbiological failure [26]. These observations suggest that delayed recognition, rather than intrinsic pathogen virulence, represents the principal determinant of unfavorable outcome in P. micra-associated PJIs.
Despite these insights, important knowledge gaps remain. Systematic data on the true incidence of P. micra in PJIs, its virulence determinants in vivo, and its interactions with other microorganisms within prosthetic biofilms are still limited. Furthermore, the predominance of single case reports and small case series constrains the ability to draw robust conclusions regarding optimal surgical or antimicrobial strategies. Future multicenter studies integrating detailed clinical data with advanced microbiological and genomic analyses are therefore essential to better define the epidemiological burden and clinical significance of this organism in implant-associated infections.
Preventive considerations for PJI caused by oral pathobionts have been advocated for, and they should be guided by current evidence rather than routine dental interventions. Although P. micra, another Gram-positive anaerobic cocci commonly colonizing the oral cavity, has been implicated in hematogenous seeding of joints in selected cases, particularly in the presence of poor oral hygiene, gingivitis, or periodontitis, PJIs attributable to oral anaerobes remain rare when compared with those caused by staphylococci [28]. A recent international consensus and meta-analysis published in 2025 found no statistically significant reduction in surgical site infection or PJI rates among patients undergoing major orthopedic procedures who received routine preoperative dental screening compared with those who did not [42]. Consistently, current clinical practice guidelines from the American Academy of Orthopaedic Surgeons and the Infectious Diseases Society of America do not recommend routine dental clearance or antibiotic prophylaxis prior to dental procedures in patients with hip or knee arthroplasties, even in high-risk populations, due to the low incidence of oral flora-related PJI and the lack of demonstrated benefit [43]. Preventive strategies should therefore focus on established perioperative measures, including optimization of comorbidities, standard perioperative antimicrobial prophylaxis, and skin and nasal decolonization [44,45]. Perhaps, in selected patients such as elderly individuals and those with poor dentition, active periodontal disease, prior PJI, or significant immunosuppression, an individualized risk assessment and multidisciplinary approach may be reasonable, while maintaining good oral hygiene and prompt treatment of dental infections remains universally recommended [42]. Despite continuous technical advancements, conventional culture-based identification methods often result in low microbial yields and delayed diagnoses [28,41]. In addition, due to the polymicrobial contexts in which it is often found, P. micra remains poorly characterized in implant-associated infections. In a literature review, Watanabe et al. found 126 cases of bacteremia caused by Gram-positive anaerobes between 2016 and 2018, a substantial increase compared to the 70 cases reported between 2013 and 2015, largely attributed to the introduction of techniques such as MALDI-TOF MS and 16S rRNA gene sequencing [46].
Genomic analyses of P. micra have revealed potential virulent genes that may contribute to its pathogenicity [47,48]. The BLAST search (https://blast.ncbi.nlm.nih.gov/Blast.cgi, accessed on 26 April 2025) revealed a 97.2% identity with a strain isolated from a Spanish biorepository, SAMN29629855, representing the genome with the highest similarity. The constructed dendrogram (Figure 4) highlighted virulent genes such as groEL, tufA, clpP, ctrD, srtC4, and gaIE, which are associated with adhesion, survival under oxidative stress, and immune modulation. Pinheiro et al., in a metatranscriptomic analysis of the endodontic microbiome, showed that the tufA was among the most highly expressed genes in the context of periodontitis pathogenesis, primarily contributing to bacterial adhesion, promoting coaggregation/coadhesion with other bacterial species and epithelial cells of the oral mucosa, thereby facilitating tissue invasion and dissemination [49]. The activation of cellular proliferation signaling pathways by P. micra has even been implicated in colorectal carcinogenesis, as demonstrated by Chang et al. in an animal model [17]. Additionally, groEL chaperonins play a key role in biofilm formation by enabling bacterial survival under neutrophil-generated oxidative stress [47,49]. Proteases such as gingipains, produced during polymicrobial interactions, further contribute to virulence by cleaving proinflammatory cytokines—including IL-2, IL-1β, TNF-α, IL-6, and IL-8—thereby creating irregularities in the host’s immune response, favoring local dysbiosis and tissue destruction. Indeed, intense bone tissue reabsorption was clearly identified surrounding the knee prosthesis of our clinical case. Other pathogenic mechanisms include the remodeling of the biofilm in favor of inflammatory bacteria, evasion of innate immunity, and proteolytic degradation of immunoglobulins (IgG, IgA, and IgM) and complement proteins C3 and C4 [48,49].
In the genome analysis, resistance genes from the van operon (vanW, vanT, and vanY) were detected. However, none of these genes are directly associated with glycopeptide resistance, particularly in the absence of key determinants such as vanA or vanB, which are the main drivers of high-level vancomycin resistance through modification of the antimicrobial binding target. Pinheiro et al. found an association of vanA and vanB genes with resistance to glycopeptides by altering the antimicrobial binding site, but these genes were lacking in the clinical strain analyzed [49]. Interpretation of sequencing results should always be based on clinical context, as the method can identify DNA from colonizing organisms, which is one of the limitations of the WGS technique. Consistently, MIC-based phenotypic susceptibility testing did not demonstrate glycopeptide resistance in the isolate. Therefore, the van operon finding in this case was interpreted as a genomic observation with potential epidemiological relevance, rather than evidence of expressed resistance requiring modification of therapy. Importantly, sequencing data should always be interpreted within the clinical context, as WGS may identify resistance-associated genetic elements that are not expressed or that lack functional impacts, and may also capture DNA from colonizing organisms. In the present case, concordant identification of P. micra by both culture and WGS, together with the clinical scenario, supported its role as a true pathogen.
This report is limited by its single-case design, which inherently restricts the generalisability of the clinical, microbiological, and genomic observations presented. Although whole-genome sequencing identified several genes previously associated with virulence and antimicrobial resistance in Parvimonas micra, these findings are based on genomic annotation and homology and were not supported by functional validation. No experimental assays, such as biofilm formation studies or gene expression analyses, were performed; therefore, the presence of these genes should not be interpreted as definitive evidence of their expression or biological activity in vivo. Our case report is unique in that it demonstrates an unusual association of P. micra and S. aureus with a chronic onset of PJI. The clinical presentation was atypical for a polymicrobial Gram-positive PJI, as progressive local pain was the unique presenting symptom. It is known that anaerobic bacteria account for 15% of the etiological agents in PJIs, as reported by Zeller et al. in a retrospective cohort study, although this figure is likely an underestimation [50]. Cases of PJIs caused by anaerobic species such as Cutibacterium, Clostridium, Veillonella, Bacteroides, Finegoldia, Fusobacterium, and Actinomyces have been documented, occurring either as monomicrobial or polymicrobial infections. These can be found in either monomicrobial or polymicrobial infections. Therefore, the advent of next-generation sequencing methods has greatly optimized early diagnosis and guided therapy for affected patients, as illustrated by the present case, and has enhanced understanding of the phenotypic expression of virulent genes in the context of implant-associated infections [51,52].
4. Conclusions
This case report highlights the underestimated pathogenic role of Parvimonas micra in chronic PJI, particularly in late-onset and polymicrobial biofilm-associated scenarios. The association of P. micra with Staphylococcus aureus in a delayed knee prosthetic joint infection likely underscores the capacity of this anaerobic organism, traditionally regarded as a commensal of the oral and gastrointestinal microbiota, to behave as a clinically relevant pathogen in implant-related infections. The indolent clinical presentation observed, characterized mainly by progressive pain and radiographic evidence of prosthetic loosening in the absence of prominent systemic inflammatory signs, illustrates the diagnostic challenges inherent to anaerobic PJIs. The consistent recovery of P. micra and S. aureus from synovial fluid, multiple deep intraoperative tissue samples, and sonication fluid, together with marked neutrophilic inflammation, supports their role as true pathogens and reinforces the importance of optimized microbiological diagnostic strategies, including prolonged anaerobic culture and advanced identification techniques. The integration of MALDI-TOF MS and whole-genome sequencing was pivotal for accurate pathogen identification and characterization. Genomic analysis of the isolated P. micra strain revealed the presence of likely genomic traits associated with infection, including genes related to adhesion, oxidative stress response, immune modulation, and biofilm formation, which may contribute to persistence in the prosthetic joint environment. Whole-genome sequencing also enabled high-resolution comparison with reference strains and identification of resistance-associated elements of the van operon, although the absence of phenotypic glycopeptide resistance emphasizes the need to interpret genomic findings within the clinical and microbiological context. The favorable clinical outcome achieved through a two-stage revision procedure combined with prolonged, pathogen-targeted antimicrobial therapy highlights the effectiveness of a multidisciplinary approach integrating orthopedic surgery, infectious diseases, and clinical microbiology. Overall, this case reinforces that Parvimonas micra should not be overlooked in chronic prosthetic joint infections and demonstrates that the incorporation of whole-genome sequencing may enhance biological understanding, refine diagnostic accuracy, and support precision diagnostics in rare causes of prosthetic joint infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patel R. Periprosthetic joint infection N. Engl. J. Med.20233882512623665235610.1056/NEJ Mra 2203477 · doi ↗ · pubmed ↗
- 2Pappas M.A. Spindler K.P. Hu B. Higuera-Rueda C.A. Rothberg M.B. Volume and outcomes of joint arthroplasty J. Arthroplast.2022372128213310.1016/j.arth.2022.05.011PMC 1044886735568138 · doi ↗ · pubmed ↗
- 3Kurtz S. Ong K. Lau E. Mowat F. Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030 J. Bone Jt. Surg. Am.2007897807851740380010.2106/JBJS.F.00222 · doi ↗ · pubmed ↗
- 4RomanòC.L. Trentinaglia M.T. De Vecchi E. Logoluso N. George D.A. Morelli I. Drago L. Cost-benefit analysis of antibiofilm microbiological techniques for peri-prosthetic joint infection diagnosis BMC Infect. Dis.2018186552960954010.1186/s 12879-018-3050-8PMC 5879767 · doi ↗ · pubmed ↗
- 5Leonenko V.N. Kaliberda Y.E. Muravyova Y.V. Artyukh V.A. A decision support framework for periprosthetic joint infection treatment: A cost-effectiveness analysis using two modeling approaches J. Pers. Med.202212121610.3390/jpm 1208121635893309 PMC 9394318 · doi ↗ · pubmed ↗
- 6Bozic K.J. Ries M.D. The impact of infection after total hip arthroplasty on hospital and surgeon resource utilization J. Bone Jt. Surg. Am.200587174617511608561410.2106/JBJS.D.02937 · doi ↗ · pubmed ↗
- 7Zmistowski B. Karam J.A. Durinka J.B. Casper D.S. Parvizi J. Periprosthetic joint infection increases the risk of one-year mortality J. Bone Jt. Surg. Am.2013952177218410.2106/JBJS.L.0078924352771 · doi ↗ · pubmed ↗
- 8Shah N.B. Tande A.J. Patel R. Berbari E.F. Anaerobic prosthetic joint infection Anaerobe 2015361810.1016/j.anaerobe.2015.08.00326341272 · doi ↗ · pubmed ↗