Primary fungal iliopsoas abscess caused by Candida albicans: a rare clinical entity
Hazem Alouani, Ghazi Lâamiri, Manel Yaacoubi, Jasser Rchidi, Mahdi Bouassida, Hassen Touinsi

TL;DR
This paper reports a rare case of a fungal abscess in the iliopsoas muscle caused by Candida albicans in a diabetic patient, highlighting the importance of diagnosis and treatment.
Contribution
The paper presents a rare clinical case of C. albicans causing iliopsoas abscess, emphasizing its diagnostic challenges and management.
Findings
Candida albicans is an extremely rare cause of iliopsoas abscess.
Diabetes increases the risk of fungal abscesses due to hematogenous spread.
Combined drainage and antifungal therapy leads to favorable outcomes in such cases.
Abstract
•Candida albicans is an extremely rare cause of iliopsoas abscess.•Diabetes predisposes to hematogenous fungal spread.•Fungal abscesses may initially mimic pyogenic infections.•Culture confirmation is essential, especially when empirical antibiotics fail.•Combined drainage and antifungal therapy lead to excellent outcomes. Candida albicans is an extremely rare cause of iliopsoas abscess. Diabetes predisposes to hematogenous fungal spread. Fungal abscesses may initially mimic pyogenic infections. Culture confirmation is essential, especially when empirical antibiotics fail. Combined drainage and antifungal therapy lead to excellent outcomes. Fungal iliopsoas abscesses are exceedingly rare and typically occur in immunocompromised individuals. Candida albicans is an uncommon pathogen in this location and may lead to delayed diagnosis due to its nonspecific clinical features. Groin…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
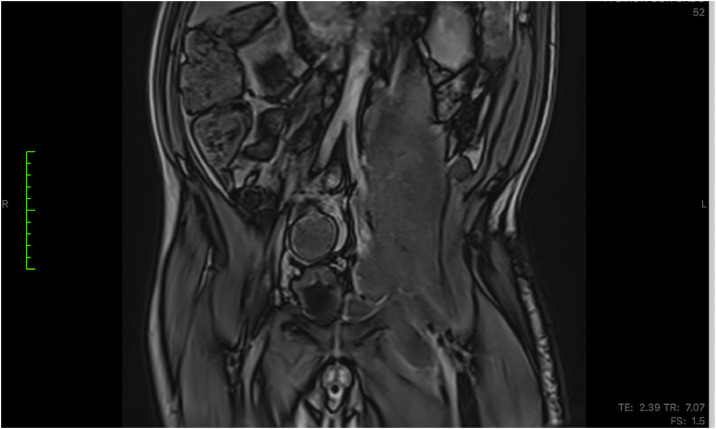 Figure 1
Figure 1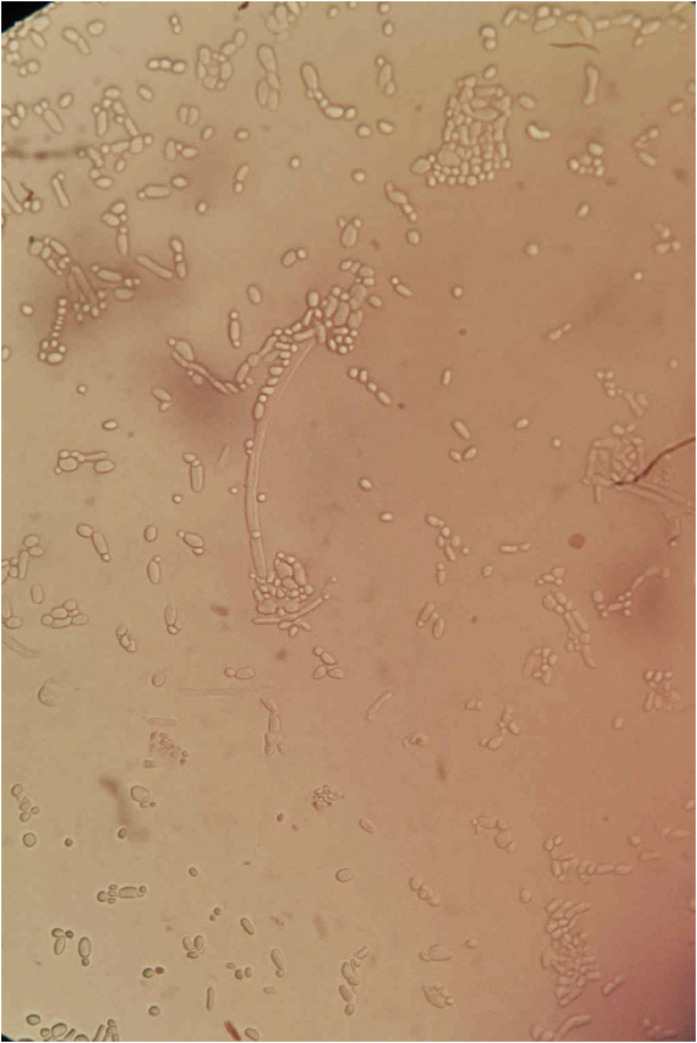 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Orthopedic Infections and Treatments · Amoebic Infections and Treatments
Introduction
Iliopsoas abscess is an infrequent condition that may be primary (hematogenous spread) or secondary to adjacent infection [1]. While bacterial causes—particularly Staphylococcus aureus—are most common, fungal iliopsoas abscesses remain exceptionally rare and are typically associated with immunosuppression, prolonged hospitalization, or invasive medical procedures [2].
Candida albicans is an uncommon pathogen in this anatomical location, and only isolated cases have been reported. Diabetes mellitus is a recognized risk factor for invasive candidiasis due to impaired neutrophil function and altered host immunity [3].
This report describes a large C albicans iliopsoas abscess extending into the groin, highlighting diagnostic challenges and therapeutic considerations. This case has been reported in line with the Surgical Case Report (SCARE criteria) [4].
Case presentation
A 46-year-old diabetic male with no additional comorbidities presented with a several-week history of progressive left lower abdominal, flank, and groin pain. The pain radiated along the anterior aspect of the thigh and worsened with ambulation and hip flexion. He denied fever, chills, urinary symptoms, or recent gastrointestinal infection. There was no history of trauma, spinal disease, or prior abdominal surgery.
On examination, the patient appeared uncomfortable, maintaining the left hip in slight flexion. There was deep tenderness over the left iliac fossa and along the iliopsoas trajectory, with marked pain during passive hip extension (positive psoas sign). An inguinal swelling was detected, and the patient reported a groin fullness.
Laboratory tests demonstrated moderate inflammatory markers without leukocytosis. Blood glucose levels were elevated but there were no signs of ketoacidosis. Blood cultures were drawn and remained negative.
An magnetic resonance imaging (MRI) of the abdomen and pelvis revealed a large left iliopsoas abscess exceeding 10 cm, extending inferiorly along the muscle sheath, and reaching the inguinal region (Figure 1). The collection exhibited thickened margins but no gas. No gastrointestinal or vertebral source of infection was identified, suggesting a primary abscess likely related to hematogenous spread.Figure 1. Magnetic resource imaging showing a large left iliopsoas abscess (>10 cm) extending inferiorly into the groin.Figure 1 dummy alt text
MRI was selected as the initial imaging modality because it was readily accessible at the time of evaluation and provides superior soft-tissue contrast for defining iliopsoas muscle involvement and extension toward the groin. Given the patient’s stable condition and absence of acute abdominal symptoms, MRI did not delay management and was deemed appropriate for characterizing the collection.
Given the size and inferior extension into the groin, a combined approach was chosen. The patient underwent surgical drainage through an inguinal incision with evacuation of thick purulent material, followed by placement of a wide-bore drain. A computed tomography-guided percutaneous drain was inserted into a deeper loculated portion of the collection. Empirical antifungal therapy with fluconazole was started early due to the atypical presentation and the patient’s diabetic status.
Microbiological analysis of the drained material revealed pure growth of C. albicans on Sabouraud dextrose agar (Figure 2). No bacteria were isolated. Blood cultures remained sterile, confirming a primary fungal iliopsoas abscess.Figure 2. Microscopic appearance showing growth of Candida albicans obtained from the drained abscess.Figure 2 dummy alt text
Additional investigations were performed to identify a potential infectious source. HIV serology was negative, and a dental evaluation revealed no oral or odontogenic infection. Colonoscopy was not performed, as the patient had no gastrointestinal symptoms and imaging showed no communication with the bowel or signs suggestive of an underlying colonic pathology.
The patient responded well to drainage and targeted antifungal treatment, with rapid pain improvement and progressive decrease in drain output. Follow-up imaging showed near-complete resolution. The patient received fluconazole at a dose of 400 mg/day intravenously for 7 days, followed by oral fluconazole 400 mg/day to complete a total 4-week course, in accordance with current Infectious Diseases Society of America (IDSA) recommendations for deep-seated candidiasis.
Discussion
Iliopsoas abscess is a rare but potentially serious condition that may arise from hematogenous spread (primary) or from contiguous infection (secondary) [1]. While S. aureus remains the most common pathogen in primary cases, fungal involvement—particularly due to C. albicans—is extremely uncommon [2]. The differential microbiological diagnosis of iliopsoas abscesses classically includes S. aureus in primary hematogenous cases, and enteric gram-negative bacilli, streptococci, and mixed aerobic–anaerobic flora in secondary abscesses related to gastrointestinal or genitourinary disease. Mycobacterium tuberculosis must also be considered, particularly in endemic regions. Fungal etiologies are rare, and most frequently accompany mixed bacterial infections rather than appearing in isolation.
Isolated Candida iliopsoas abscesses have been described only sporadically, typically in immunocompromised individuals, intravenous drug users, or patients with prolonged hospitalization [3].
In the present case, diabetes mellitus was the sole identifiable predisposing factor. Diabetes impairs neutrophil chemotaxis, reduces phagocytic function, and facilitates fungal translocation, creating a permissive environment for invasive candidiasis. Hematogenous seeding is the most likely mechanism, especially given the absence of any adjacent infectious source on imaging [5].
Clinical manifestations of iliopsoas abscesses are often nonspecific. The classic triad—fever, back pain, and psoas spasm—is observed in fewer than one-third of patients [6]. Groin extension, as in this case, may mimic inguinal pathology or musculoskeletal disorders, contributing to delays in diagnosis. Pain during hip extension (positive psoas sign) and limitation of hip movement are important clues.
The isolation of pure C. albicans from the drained pus represents strong evidence for a true fungal abscess rather than colonization. The absence of any bacterial growth reinforces the diagnosis of a primary fungal abscess, demonstrating the ability of Candida species to behave as true pathogens in susceptible hosts such as patients with diabetes. Mixed bacterial–fungal infections are more common, and pure fungal abscesses highlight the pathogenic capacity of Candida in susceptible hosts [7].
Optimal management requires drainage—either percutaneous or surgical—combined with systemic antifungal therapy [8]. Large or multiloculated abscesses, especially those extending into the groin, often benefit from a combined approach, as performed in this case. Fluconazole remains the drug of choice for susceptible C. albicans strains, offering excellent penetration into soft tissues.
Early recognition of fungal etiology is essential, as empirical antibacterial therapy alone is ineffective and may delay appropriate treatment. With adequate drainage and antifungal therapy, outcomes are generally favorable.
Conclusion
Large C. albicans iliopsoas abscesses extending into the groin are exceptionally rare. Early microbiological identification, prompt drainage, and appropriate antifungal treatment are key to a successful outcome.
Declaration of competing interest
The authors have no competing interests to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1He W.Yuan Y.Huang J.A case report of iliopsoas abscess and literature review Medicine 1032024 e 3935610.1097/MD.0000000000039356 PMC 1133274239151535 · doi ↗ · pubmed ↗
- 2Kawai Y.Banshodani M.Moriishi M.Sato T.Shintaku S.Masaki T.Iliopsoas abscess in hemodialysis patients with end-stage kidney disease Ther Apher Dial 23201953454110.1111/1744-9987.1280130864296 · doi ↗ · pubmed ↗
- 3Fukuhara S.Nishimura K.Yoshimura K.Okuyama A.Yamato M.Kawamori D.A case of psoas abscess caused by Candida albicans Hinyokika Kiyo 49200314114312728526 · pubmed ↗
- 4Kerwan A.Al-Jabir A.Mathew G.Sohrabi C.Rashid R.Franchi T.Revised surgical case report (SCARE) guideline: an update for the age of artificial intelligence Premier J Sci 10202510007910.70389/PJS.100079 · doi ↗
- 5Valero Soriano M.González Valverde F.M.Albarracín Marín-Blázquez A.Absceso de psoas por Candida spp. en un paciente inmunocompetente. Absceso de psoas por Candida spp. en un paciente inmunocompetente Med Clin (Barc)157202125926010.1016/j.medcli.2020.06.03532792259 · doi ↗ · pubmed ↗
- 6Sobaih B.Sobaih L.Zamil FA.Iliopsoas abscess Pak J Med Sci 37202160560710.12669/pjms.37.2.381633679960 PMC 7931313 · doi ↗ · pubmed ↗
- 7Lin M.F.Lau Y.J.Hu B.S.Shi Z.Y.Lin YH.Pyogenic psoas abscess: analysis of 27 cases J Microbiol Immunol Infect Wei Mian Yu Gan Ran Za Zhi 32199926126810650491 · pubmed ↗
- 8Tuon F.F.Nicodemo AC.Candida albicans skin abscess Rev Inst Med Trop Sao Paulo 48200630130210.1590/s 0036-4665200600050001217086322 · doi ↗ · pubmed ↗