Long‐Term Impact of EGUIDE Training on Facility‐Wide Guideline Adherence Rate in Schizophrenia and Major Depressive Disorder—A Methodological Reflection
Ghufran Saeed Rizvi

TL;DR
This paper points out methodological issues in a study about training effects on mental health treatment guidelines and suggests better research approaches.
Contribution
The paper introduces methodological recommendations to improve future evaluations of training programs in clinical settings.
Findings
The original study had selection bias and ignored data clustering.
Quasiexperimental designs and multilevel modeling are recommended for future research.
Patient-centered outcomes should be prioritized to assess clinical effectiveness accurately.
Abstract
This Letter highlights crucial methodological flaws, including selection bias and ignored data clustering, in the EGUIDE training impact study. We recommend adopting quasiexperimental designs, multilevel modeling, and patient‐centered outcomes to ensure future research accurately confirms the program's true clinical effectiveness.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
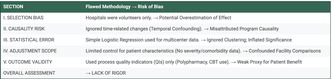 Figure 1
Figure 1| Issue | Potential impact | Recommended improvement |
|---|---|---|
| Selection bias | Overestimation of EGUIDE impact | Include baseline comparisons and structured recruitment |
| Temporal confounding | Misattributed causality | Use interrupted time‐series or difference‐in‐differences designs |
| Ignored clustering | Inflated significance | Apply multilevel or hierarchical models |
| Limited case‐mix control | Confounded facility comparisons | Include illness severity and comorbidity adjustments |
| QI validity concerns | Weak proxy for actual patient benefit | Integrate patient‐centered and outcome‐based indicators |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSchizophrenia research and treatment · Health Policy Implementation Science · Digital Mental Health Interventions
Dear Editor,
I read with great interest the article “Long‐Term Impact of EGUIDE Training on Facility‐Wide Guideline Adherence Rate in Schizophrenia and Major Depressive Disorder: A Multicenter Study” by Naomi Hasegawa et al., published in Neuropsychopharmacology Reports (DOI: 10.1002/npr2.70067). The study made an important contribution by examining how EGUIDE training improved psychiatric guideline adherence across Japan. The large sample size and multicenter approach are strengths of this work.
However, some methodological points need more attention. First, the study included only hospitals that volunteered for the EGUIDE program. Such hospitals may already have better facilities, more motivated staff, or higher awareness of guideline‐based care. This may have caused selection bias and overestimated the true impact of training. Studies by Millard et al. [1] and Enzenbach et al. [2] have shown that structured recruitment and baseline comparisons can reduce this bias. Including preparticipation data about hospitals would improve generalizability.
Second, the study design lacked quasiexperimental elements, such as interrupted time‐series or difference‐in‐differences analysis. These methods help to separate the program's effects from other national mental health initiatives or gradual improvements in care. Trutschel et al. [3] and Chang and Stuart [4] noted that ignoring time‐related changes in observational studies may lead to false causal conclusions.
Third, the authors used simple logistic regression, though the data were collected from multiple hospitals. This ignores the fact that results from the same facility are related. Multilevel models or generalized estimating equations, as suggested by Austin and Kapral [5], would account for clustering and provide more accurate results. These methods are now widely used in multicenter studies.
Fourth, the study adjusted only for limited factors such as age, sex, and hospital type. It did not control for disease severity, comorbidities, or illness duration, which can strongly influence outcomes. As shown by Sibert et al. [6] and Groenewegen et al. [7], adjusting for these case‐mix factors helps to make fair comparisons between hospitals.
Lastly, the quality indicators (QIs) used in this study mainly measured process outcomes such as polypharmacy reduction and use of CBT. These do not directly reflect patient benefits. Imani et al. [8] and Sterrantino et al. [9] recommend including both process and patient‐centered outcomes, such as relapse rate or quality of life, to capture the real clinical effect. The comprehensive summary of methodological issues and recommendations is presented in Table 1.
Future studies on educational programs like EGUIDE should include these methodological improvements. Careful selection of hospitals can reduce bias. Quasiexperimental designs can separate program effects from background trends. Multilevel analysis can improve accuracy. Broader covariate adjustment and better outcome measures can make findings more meaningful.
The EGUIDE program is a valuable national initiative for improving mental health care in Japan. Strengthening its research design will ensure that its benefits reflect real clinical improvements. With stronger methods and broader outcomes, EGUIDE can become a global model for evidence‐based psychiatric practice.
Funding
The author has nothing to report.
Ethics Statement
The author has nothing to report.
Consent
Not required.
Conflicts of Interest
The author declares no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1L. A. C. Millard , A. Fernández‐Sanlés , A. R. Carter , et al., “Exploring the Impact of Selection Bias in Observational Studies of COVID‐19: A Simulation Study,” International Journal of Epidemiology 52, no. 1 (2023): 44–57.36474414 10.1093/ije/dyac 221PMC 9908043 · doi ↗ · pubmed ↗
- 2C. Enzenbach , B. Wicklein , K. Wirkner , and M. Loeffler , “Evaluating Selection Bias in a Population‐Based Cohort Study With Low Baseline Participation: The LIFE‐Adult‐Study,” BMC Medical Research Methodology 19, no. 1 (2019): 135.31262266 10.1186/s 12874-019-0779-8PMC 6604357 · doi ↗ · pubmed ↗
- 3D. Trutschel , R. Palm , B. Holle , and M. Simon , “Methodological Approaches in Analysing Observational Data: A Practical Example on How to Address Clustering and Selection Bias,” International Journal of Nursing Studies 76 (2017): 36–44.28915416 10.1016/j.ijnurstu.2017.06.017 · doi ↗ · pubmed ↗
- 4T. Chang and E. A. Stuart , “Propensity Score Methods for Observational Studies With Clustered Data: A Review,” Statistics in Medicine 41, no. 18 (2022): 3612–3626.35603766 10.1002/sim.9437 PMC 9540428 · doi ↗ · pubmed ↗
- 5P. C. Austin , M. K. Kapral , M. V. Vyas , J. Fang , and A. Y. X. Yu , “Using Multilevel Models and Generalized Estimating Equation Models to Account for Clustering in Neurology Clinical Research,” Neurology 103, no. 9 (2024): e 209947.39393031 10.1212/WNL.0000000000209947 PMC 11469681 · doi ↗ · pubmed ↗
- 6N. T. Sibert , H. Pfaff , C. Breidenbach , S. Wesselmann , and C. Kowalski , “Different Approaches for Case‐Mix Adjustment of Patient‐Reported Outcomes to Compare Healthcare Providers—Methodological Results of a Systematic Review,” Cancers (Basel) 13, no. 16 (2021): 3964.34439117 10.3390/cancers 13163964 PMC 8392243 · doi ↗ · pubmed ↗
- 7P. P. Groenewegen , P. Spreeuwenberg , A. H. Leyland , D. de Boer , and W. Boerma , “Case‐Mix Adjustments for Patient Reported Experience and Outcome Measures in Primary Care: An Empirical Approach to Identify Patient Characteristics as Case‐Mix Adjusters Based on a Secondary Analysis of an International Survey Among Patients and Their General Practitioners in 34 Countries,” Journal of Patient‐Reported Outcomes 7, no. 1 (2023): 127.38048040 10.1186/s 41687-023-00667-8PMC 10695892 · doi ↗ · pubmed ↗
- 8A. Imani , R. Alibabayee , M. Golestani , and K. Dalal , “Key Indicators Affecting Hospital Efficiency: A Systematic Review,” Frontiers in Public Health 10 (2022): 830102.35359774 10.3389/fpubh.2022.830102 PMC 8964142 · doi ↗ · pubmed ↗