Invasive Pneumococcal Disease among Childbearing-Age Women, United States, 2007–2023
Namrata Prasad, Sopio Chochua, Bridget J. Anderson, Kathy M. Angeles, Meghan Barnes, Lee H. Harrison, Corinne Holtzman, Jessica R. Howard-Anderson, Shannon O’Brien, Susan Petit, Arthur Reingold, William Schaffner, Lesley McGee, Adam L. Cohen, Miwako Kobayashi

TL;DR
This study examines how often invasive pneumococcal disease occurs in pregnant and postpartum women in the US compared to nonpregnant women.
Contribution
The study provides new population-based incidence estimates for pneumococcal disease in pregnant and postpartum women.
Findings
Pregnant women had similar pneumococcal disease rates as nonpregnant women of childbearing age.
Postpartum women had 3.5 times higher disease incidence compared to nonpregnant women.
Findings may help guide pneumococcal vaccination recommendations for these groups.
Abstract
US data on invasive pneumococcal disease incidence among pregnant and postpartum women are limited. We estimated incidence in those groups using population-based surveillance. Compared with nonpregnant women of childbearing age, incidence was similar for pregnant women but 3.5 times higher for postpartum women. Our findings could inform pneumococcal vaccine recommendations.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
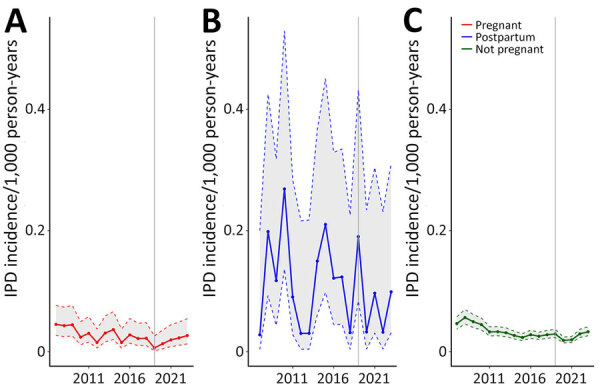 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Reproductive tract infections research · Influenza Virus Research Studies
Streptococcus pneumoniae is a leading cause of serious bacterial infections, including invasive pneumococcal disease (IPD), defined as S. pneumoniae infection in a normally sterile site (e.g., blood, cerebrospinal fluid). IPD most commonly affects young children, older adults, and people with certain underlying conditions (1). For adolescents and adults <50 years of age with specific conditions, the Advisory Committee on Immunization Practices (ACIP) recommends use of 15-valent, 20-valent, or 21-valent pneumococcal conjugate vaccines (PCV) (2). However, ACIP has not reviewed data on PCV use in pregnant or postpartum women and does not offer recommendations for those groups (3). The American College of Obstetricians and Gynecologists, by contrast, recommends PCV for pregnant women at increased risk for severe disease (4). To help address this gap in recommendations, we analyzed IPD epidemiology among US women of childbearing age. We conducted research in accordance with applicable federal law and Centers for Disease Control and Prevention policy.
We included all IPD cases among pregnant, postpartum, and nonpregnant childbearing-age women (15–44 years of age) reported by Active Bacterial Core surveillance (ABCs) during 2007–2023. ABCs is an active laboratory- and population-based, multistate surveillance system. We defined IPD as isolation of S. pneumoniae bacteria from a sterile site in a surveillance-area resident (5). We defined the postpartum period as <30 days after delivery.
We reported IPD incidence as cases per 1,000 person-years. We estimated denominators for incidence rates using published methods (6). In brief, we estimated the number of pregnant women by multiplying annual live births, induced abortions, and early and late fetal losses by the mean proportion of the year a woman is pregnant for each outcome (live birth = 0.75, abortion = 0.12, early loss = 0.14, late loss = 0.52). We estimated the number of postpartum women by multiplying live births by one twelfth. We estimated the number of nonpregnant women by subtracting pregnant and postpartum women from the total number of childbearing-age women in ABCs areas. We used a mixed-effects Poisson model, including ABCs site as a random effect, to estimate incidence rates, incidence rate ratios (IRRs), and 95% CIs.
We compared demographic and clinical characteristics and PCV20 and PCV21 serotype groups by pregnancy status across cases. We assessed differences using t test, Pearson χ^2^ test, or Fisher exact test and considered p<0.05 statistically significant. We conducted analyses using R version 4.0.4 (The R Project for Statistical Computing, https://www.r-project.org) across the entire surveillance period and during the more recent period of 2019–2023 to account for changes in PCV recommendations and serotype distribution over time.
During 2007–2023, we identified 3,651 IPD cases among childbearing-age women, including 146 (4.0%) pregnant, 61 (1.7%) postpartum, and 3,444 (94.4%) nonpregnant women (Figure). Gestational week data were available for 77 (52.7%) cases; of those, 12 (15.6%) were in the first trimester, 31 (40.3%) the second trimester, and 34 (44.2%) the third trimester at the time of illness. During 2019–2023, IPD incidence in pregnant women (0.017 [95% CI 0.011–0.028] per 1,000 person-years) was not significantly different from that in nonpregnant women (0.025 [95% CI 0.019–0.034] per 1,000 person-years) (IRR 0.68 [95% CI 0.47–1.00]). In contrast, postpartum women (0.088 [95% CI 0.048–0.161] per 1,000 person-years) had higher IPD risk than did nonpregnant women (IRR 3.49 [95% CI 2.06–5.90]).
Compared with IPD cases among nonpregnant women (mean age 35 years), pregnant (mean age 29 years; p<0.001) and postpartum case-patients (mean age 30 years; p<0.001) were younger and less likely to have underlying conditions (pregnant women = 45.2%; postpartum women = 41.0%; nonpregnant women = 69.9%; p<0.001) (Table). That difference was particularly noticeable for women with immunocompromising conditions. Pregnant women had a lower IPD case-fatality ratio (2.1%) than did nonpregnant women (7.9%; p = 0.014). Among IPD cases in pregnant and postpartum women, most (>75%) experienced favorable fetal outcomes (no pregnancy loss or clinical infection). During 2019–2023, the proportion of IPD cases caused by PCV20, PCV21, or nonvaccine serotypes did not vary significantly by pregnancy status; 484/778 (62.2%) of cases were caused by serotypes covered by PCV20 and 587/778 (75.4%) by serotypes covered by PCV21 (Table).
Our findings align with previous studies showing no increased IPD risk during pregnancy but elevated risk postpartum (7,8). One study also found IPD risk was slightly increased in third-trimester pregnant women compared with nonpregnant women (7). Similar stratifications were not possible in our study because we lacked complete gestational week data. In our study, pregnant and postpartum women were younger and healthier than nonpregnant women, which likely reflected the underlying population that becomes pregnant. Those differences might have influenced observed IPD risk and outcomes; we could not account for them in incidence and IRR estimations because we lacked denominator data stratified by age and underlying conditions. Further studies are needed to determine factors associated with increased risk for IPD in the postpartum period.
In conclusion, we found that IPD incidence was similar among pregnant and nonpregnant women but higher among postpartum women. Our findings could inform pneumococcal vaccine recommendations for women of childbearing age.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Centers for Disease Control and Prevention. Pneumococcal disease: causes and how it spreads. [cited 2025 May 21]. https://www.cdc.gov/pneumococcal/causes
- 2Centers for Disease Control and Prevention. Pneumococcal vaccine recommendations. 2024 [cited 2025 May 21]. https://www.cdc.gov/pneumococcal/hcp/vaccine-recommendations
- 3Kobayashi M, Pilishvili T, Farrar JL, Leidner AJ, Gierke R, Prasad N, et al. Pneumococcal vaccine for adults aged ≥19 years: recommendations of the Advisory Committee on Immunization Practices, United States, 2023. MMWR Recomm Rep. 2023;72:1–39. 10.15585/mmwr.rr 7203 a 137669242 PMC 10495181 · doi ↗ · pubmed ↗
- 4American College of Obstetricians and Gynecologists. Maternal immunization. 2022 [cited 2025 Jun 9]. https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2022/10/maternal-immunization
- 5Centers for Disease Control and Prevention. Active Bacterial Core surveillance (AB Cs). [cited 2025 Jun 9]. https://www.cdc.gov/abcs
- 6Centers for Disease Control and Prevention. Estimating the number of pregnant women in a geographic area—a reproductive health tool. 2024 [cited 2024 May 12]. https://www.cdc.gov/reproductive-health/media/pdfs/emergency/Pregnant-Population-Size-Estimator-508.pdf
- 7Amin-Chowdhury Z, Bertran M, Abdullahi F, Sheppard CL, Eletu SD, Litt DJ, et al. Risk of invasive pneumococcal disease during pregnancy and postpartum and association with adverse maternal and foetal outcomes: A prospective cohort study, England, 2014-19. J Infect. 2025;90:106363. 10.1016/j.jinf.2024.10636339603347 · doi ↗ · pubmed ↗
- 8Deutscher M, Lewis M, Zell ER, Taylor TH Jr, Van Beneden C, Schrag S; Active Bacterial Core Surveillance Team. Incidence and severity of invasive Streptococcus pneumoniae, group A Streptococcus, and group B Streptococcus infections among pregnant and postpartum women. Clin Infect Dis. 2011;53:114–23. 10.1093/cid/cir 32521690617 · doi ↗ · pubmed ↗