Prognostic Value of Lymph-Node Micrometastases and Isolated Tumour Cells in Gastric Cancer
José Couto, Mariana Leite, João Mendes, Cláudia Lima, Inês Arnaud, Fábio Correia Viveiros, Ana Cristina Rodrigues

TL;DR
This study examines the role of lymph-node micrometastases and isolated tumor cells in gastric cancer and their impact on patient survival.
Contribution
The study evaluates the prognostic value of IHC-detected lymph-node micrometastases and isolated tumor cells in gastric cancer patients.
Findings
Micrometastases and isolated tumor cells were found in 18.6% of patients.
The presence of ITC+/Mic+ was associated with lower survival in patients receiving perioperative chemotherapy.
Routine IHC assessment for these features is not recommended for all patients.
Abstract
Background Lymph node status is a crucial prognostic determinant in gastric cancer (GC). Conventional haematoxylin-eosin (H&E) assessment overlooks the micro volume of nodal disease. This study explored the prevalence and prognostic significance of lymph-node micrometastases (Mic) and isolated tumour cells (ITC) detected by cytokeratin AE1/AE3 immunohistochemistry (IHC) in patients undergoing gastrectomy with curative intent. Methods A retrospective, single-centre analysis of patients with gastric adenocarcinoma treated between 2014 and 2019 by curative intent gastrectomy with D2 lymphadenectomy and with IHC assessment of lymph nodes (LN). Nodal involvement was classified as macrometastases (>2 mm), Mic (>0.2-2 mm), or ITC (≤0.2 mm). Clinicopathological characteristics and survival outcomes were obtained from the institutional database. Data were analysed using χ²/Fisher's exact and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
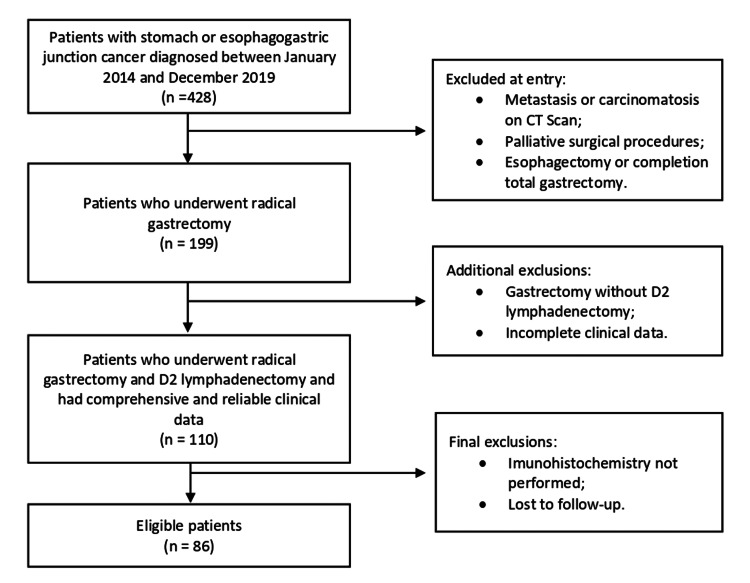 Figure 1
Figure 1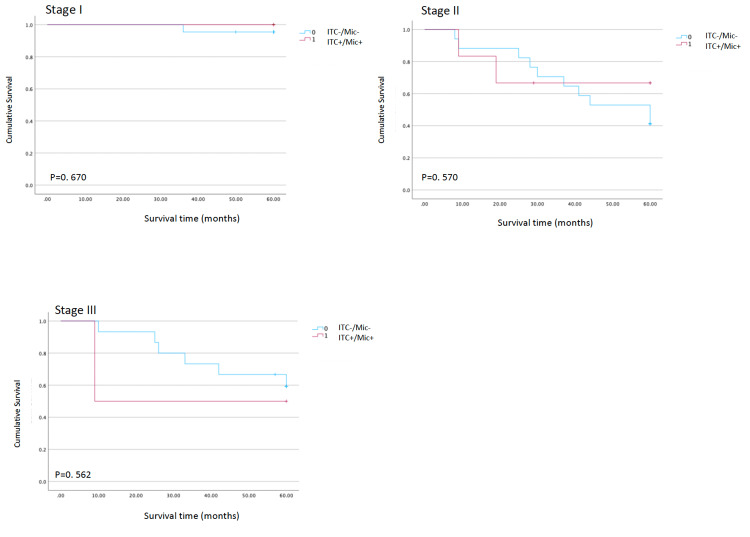 Figure 2
Figure 2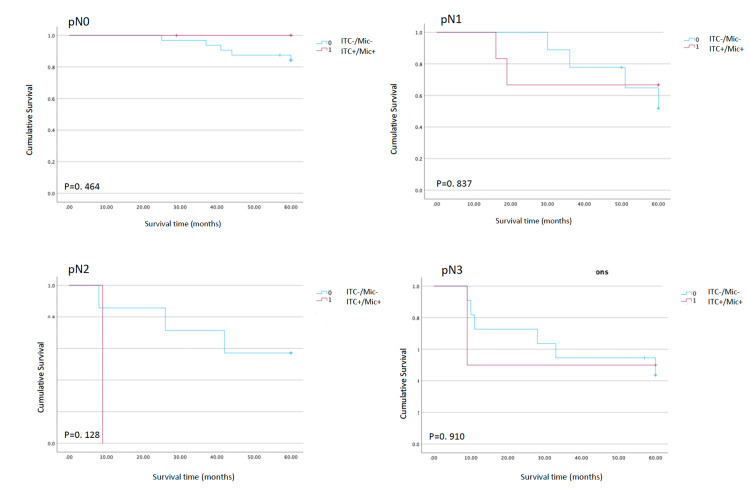 Figure 3
Figure 3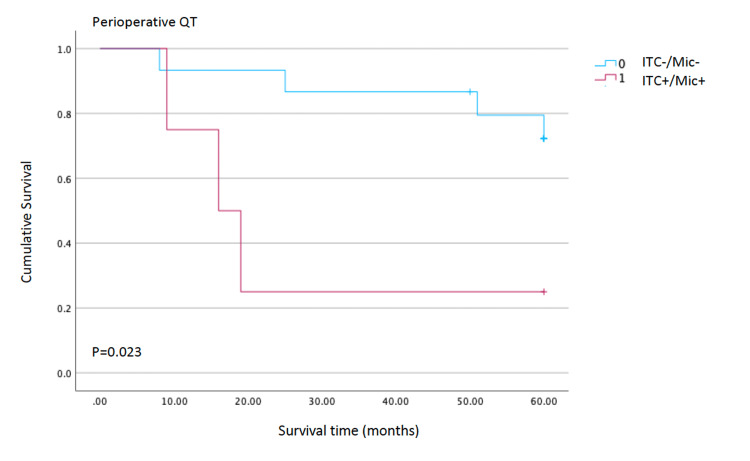 Figure 4
Figure 4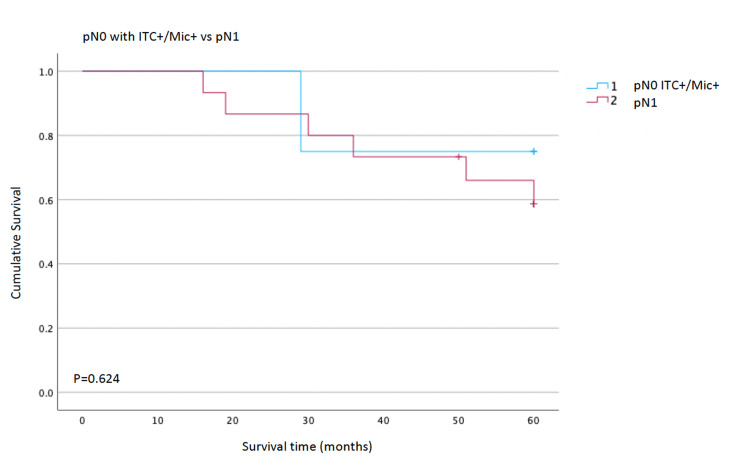 Figure 5
Figure 5| Types of lymph node metastasis | n (%) |
| ITC | 31 (1.57%) |
| Mic | 21 (1.06%) |
| Macrometastasis | 256 (12.97%) |
| Total (mean±SD) | 1974 (22.95±7.43 ) |
| Characteristics | ITC+, n (%) | p-value | Mic+, n (%) | p-value | ITC+/Mic+, n (%) | p-value | Total |
| Age in years | 72 (median) | 0.543 | 68 (median) | 0.62 | 68 (median) | 0.906 | 67.16±11.23 |
| Sex | |||||||
| Male | 6 (7%) | 0.629 | 8 (9.3%) | 0.284 | 10 (12.0%) | 0.397 | 45 (52.3%) |
| Female | 7 (8.1%) | 4 (4.7%) | 6 (7.2%) | 41 (47.7%) | |||
| Chemotherapy modality | |||||||
| Perioperative | 4 (4.7%) | 0.855 | 2 (2.3%) | 0.548 | 5 (5.8%) | 0.817 | 22 (25.6%) |
| Neoadjuvant | 0 (0%) | 0 (0%) | 0 (0%) | 2 (2.3%) | |||
| Adjuvant | 3 (3.5%) | 6 (7.1%) | 7 (8.2%) | 27 (31.4%) | |||
| No chemotherapy | 6 (7.1%) | 4 (4.7%) | 6 (7.1%) | 34 (40%) | |||
| Tumour localization | |||||||
| Proximal | 2 (2.3%) | 0.468 | 2 (2.3%) | 0.411 | 2 (2.3%) | 0.71 | 5 (5.8%) |
| Middle | 5 (5.8%) | 5 (5.8%) | 8 (9.3%) | 39 (45.3%) | |||
| Distal | 6 (7%) | 5 (5.8%) | 8 (9.3%) | 40 (46.5%) | |||
| Greatest tumour dimension (mm) | |||||||
| ≤20 | 2 (2.3%) | 0.207 | 1 (1.2%) | 0.093 | 2 (2.3%) | 0.029 | 28 (32.6%) |
| >20 | 11 (12.8%) | 11 (12.8%) | 16 (18.6%) | 58 (67.4%) | |||
| pT | |||||||
| pis | 0 (0%) | 0.448 | 0 (0%) | 0.394 | 0 (0%) | 0.199 | 2 (2.3%) |
| pT1 | 2 (2.3%) | 3 (3.5%) | 3 (3.5%) | 23 (26.7%) | |||
| pT2 | 2 (2.3%) | 2 (2.3%) | 3 (3.5%) | 17 (19.8%) | |||
| pT3 | 8 (9.3%) | 7 (8.1%) | 11 (12.8%) | 31 (36%) | |||
| pT4 | 1 (1.2%) | 0 (0%) | 1 (1.2%) | 13 (15.1%) | |||
| pN | |||||||
| pN0 | 6 (7%) | 0.432 | 3 (3.5%) | 0.07 | 6 (7.0%) | 0.042 | 44 (51.2%) |
| pN1 | 4 (4.7%) | 7 (8.1%) | 8 (9.3%) | 17 (19.8%) | |||
| pN2 | 0 (0%) | 1 (1.2%) | 1 (1.2%) | 9 (10.5%) | |||
| pN3 | 3 (3.5%) | 1 (1.2%) | 3 (3.5%) | 16 (18.6%) | |||
| pTMN | |||||||
| pTMN, stage I | 3 (3.5%) | 0.397 | 3 (3.5%) | 0.278 | 4 (4.7%) | 0.129 | 31 (36.0%) |
| pTMN, stage II | 6 (7%) | 8 (9.3%) | 10 (11.6%) | 29 (33.7%) | |||
| pTMN, stage III | 3 (3.5%) | 1 (1.2%) | 3 (3.5%) | 20 (23.3%) | |||
| pTMN, stage IV | 0 (0%) | 0 (0%) | 0 (0%) | 1 (1.2%) | |||
| Type of invasion | |||||||
| Lymphatic | 6 (7%) | 0.75 | 6 (7%) | 0.063 | 8 (9.3%) | 0.035 | 21 (24.4%) |
| Venous | 5 (5.8%) | 0.291 | 7 (8.1%) | 0.007 | 8 (9.3%) | 0.035 | 21 (24.4%) |
| Perineural | 8 (9.3%) | 0.238 | 8 (9.3%) | 0.131 | 11 (12.8%) | 0.163 | 40 (46.5%) |
| Laurén classification | |||||||
| Intestinal | 6 (7.0%) | 0.161 | 6 (7.0%) | 0.192 | 8 (9.3%) | 0.16 | 52 (60.5%) |
| Diffuse | 5 (5.8%) | 4 (4.7%) | 8 (9.3%) | 29 (33.7%) | |||
| Mixed | 2 (2.3%) | 2 (2.3%) | 2 (2.3%) | 5 (5.8%) | |||
| Differentiation | |||||||
| Well differentiated (G1) | 1 (1.2%) | 0.320 | 0 (0%) | 0.208 | 1 (1.2%) | 0.164 | 15 (17.4%) |
| Moderately differentiated (G2) | 4 (4.7%) | 5 (5.8%) | 6 (7.0%) | 34 (39.5%) | |||
| Poorly differentiated (G3) | 8 (9.3%) | 7 (8.1%) | 11 (12.8%) | 37 (43.0%) | |||
| Operative procedure | |||||||
| Total gastrectomy | 36 (41.9%) | ||||||
| Distal gastrectomy | 50 (58.1%) | ||||||
| Anastomosis | |||||||
| BII | 44 (51.2%) | ||||||
| Y-Roux | 42 (48%) | ||||||
| Mean of LN retrieved | 22.95 (±7.43) | ||||||
| Five-year OS | 2 (2.8%) | 1 | 3 (4.2%) | 0.847 | 4 (5.6%) | 1 | 22 (30.6%) |
| Non-oncologic mortality | 14 (16.3%) | ||||||
| Patients demise due to postoperative complications | 5 (5.8%) | ||||||
| Death related to chemotherapy | 2 (2.3%) | ||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal Cancer Research and Treatment · Cancer Cells and Metastasis
Introduction
Lymph node metastasis is a key prognostic factor in gastric cancer (GC). The number of positive lymph nodes (LN) is essential for stage stratification and helps predict patient survival [1]. The current standard of care is radical gastrectomy, comprising gastric resection with adequate tumour-free margins and a D2 lymphadenectomy [2]. Available evidence demonstrates that radical gastrectomy with lymphadenectomy, resulting in node-negative (pN0) status on hematoxylin-eosin (H&E) staining, does not rule out the risk of recurrence [3,4]. Lymph node histopathological analysis depends on representative sections from resected nodes; consequently, lymph node micrometastases often escape routine detection. Recognition of this limited sensitivity has prompted the use of more sensitive assays to detect micrometastatic tumour cells.
With advances such as immunohistochemistry (IHC), the detection rate of micrometastases (Mic) or isolated tumour cells (ITC), not visible on routinely performed H&E staining, has increased [5-7]. Regional lymph node metastases could be subclassified based on the maximal tumour deposit dimension. Metastatic deposits measuring >0.2 to ≤2.0 mm are classified as micrometastases. Isolated tumour cells are defined as single cells or small clusters measuring <0.2 mm in greatest dimension [8]. Despite the growing research enabled by these methods, ITC and Mic have become an emerging area of investigation. Nevertheless, its clinical relevance remains debated, and there is no consensus on either optimal management or the prognostic impact [9]. To address this knowledge gap, we conducted a retrospective cohort study of patients undergoing curative-intent gastrectomy with D2 lymphadenectomy and cytokeratin AE1/AE3 immunohistochemistry assessment of negative lymph nodes. The primary objective was to evaluate the prognostic value of low-volume nodal disease, defined as isolated tumour cells and/or micrometastases, on overall survival. Secondary objectives were to quantify the prevalence of isolated tumour cells and micrometastases at both the patient and lymph-node levels and to identify clinicopathological features associated with them.
Materials and methods
Study design and data collection
We analyzed gastric cancer patients treated with curative-intent gastrectomy between 2014 and 2019 at our institution. Patients were enrolled if they underwent radical gastrectomy with D2 lymphadenectomy, R0 margins, had no evidence of distant metastases, had complete clinicopathologic data available, and underwent immunohistochemical examination of lymph nodes (Figure 1). Of 428 patients diagnosed with gastric or oesophagogastric junction cancer (2014-2019), 199 underwent radical gastrectomy; 110 had D2 lymphadenectomy and comprehensive clinical data; and 86 met all inclusion criteria. Clinicopathological features, including tumour characteristics and overall survival (OS), were collected.
Flow chart showing the patient selection process
Lymph node evaluation
Immunohistochemistry Analysis
Lymph nodes retrieved were fixed in formalin and embedded in paraffin according to a standardized protocol. Routine histopathological examination with H&E was first conducted, and only cases classified as node-negative on conventional H&E were selected for supplementary immunohistochemical analysis, irrespective of the patient's overall pathological lymph node (pN) category. Lymph nodes already positive on H&E were not subjected to IHC.
For each lymph node, a single section was obtained at the mid-level (central portion) of the node, and two slides were prepared from this central section: one for routine H&E staining and, when applicable, a second slide for IHC.
IHC reassessment was performed using monoclonal antibodies against human cytokeratins (AE1/AE3). The AE1/AE3 antibody mixture targets human epithelial cytokeratins and shows no reactivity in lymphoid tissue.
Tissue sections from paraffin blocks were deparaffinized with xylene and rehydrated with graded ethanol. Endogenous peroxidase activity was blocked with hydrogen peroxide for 30 minutes, followed by overnight incubation with the AE1/AE3 primary antibody at 4° C. The secondary antibody was then applied, followed by exposure to streptavidin-biotin peroxidase.
Positive expression was defined as cells displaying brownish-yellow granular staining within the cytoplasm.
Initial microscopic evaluation with H&E was performed by experienced gastrointestinal pathologists.
All immunohistochemically stained sections were evaluated by a single pathologist according to predefined histopathological criteria. Given the single-observer assessment, no formal interobserver agreement analysis was performed.
Definition of Lymph Node Positive Findings
Nodal disease was classified according to the maximal diameter of the metastatic deposit: macrometastasis (>2.0 mm), Mic (>0.2-2.0 mm), and ITC (single cells or clusters ≤0.2 mm). According to European Society for Medical Oncology (ESMO) and National Comprehensive Cancer Network (NCCN) guidelines, patients with isolated tumour ceIls or micrometastases in lymph nodes are staged as pN0. For comparative analyses, patients were categorized as ITC+ (presence of ITC), Mic+ (presence of micrometastasis), or ITC+/Mic+ (presence of ITC and/or micrometastasis) [10,11].
Statistical analysis
The descriptive analysis of qualitative variables was performed using absolute and relative frequencies; for quantitative variables, the mean and standard deviation were found. The comparison of means between groups was performed using the Wilcoxon non-parametric test. The association between categorical variables was evaluated by Fisher's exact test or the chi-square test, when appropriate. All tests were two-sided, and p-values less than 0.05 were considered statistically significant. Statistical analysis was performed using SPSS software, version 29.0 (IBM Inc., Armonk, US). This manuscript was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [12].
Results
Patient and tumour characteristics
A total of 428 GC cases were reviewed, 86 met the inclusion criteria of curative-intent radical gastrectomy, R0 resection, and available immunohistochemical nodal assessment. The median follow-up duration was 50 months, and the five-year OS rate for the entire cohort was 55.8%. The mean age of the patients was 67.2±11.2 years, and 52.3% (n=45) were male.
The vast majority of tumours (91.8%, n=79) were located in the middle or distal third of the stomach. According to Laurén's classification, the diffuse type was documented in 33.7% (n=29) of cases, followed by the intestinal type (60.5%, n=52) and the mixed type (5.8%, n=5).
Tumour was confined to the lamina propria of the mucosa in 2.3% (Tis, n=2), invaded the lamina propria, muscularis mucosae, or submucosa in 26.7% (T1, n=23), the muscularis propria in 19.8% (T2, n=17), the subserosa in 36.0% (T3, n=31), and the serosa in 15.1% (T4, n=13).
Vascular, lymphatic, and perineural invasion were present in 24.4% (n=21), 24.4% (n=21), and 46.5% (n=40) of cases, respectively. Total gastrectomy was performed in 41.9% of patients and subtotal gastrectomy in 58.1% (n=50).
Nodal involvement profile
A total of 1974 lymph nodes were obtained and examined by routine H&E (mean 22.95±7.43 per specimen), whereas Mic and ITC were identified on H&E-negative nodes.
Overall, 256 (12.97%) held macrometastases, 21 (1.06%) Mic and 31 (1.57%) ITC. At the patient level, 44 patients (51.2%) were classified as pN0 on routine H&E, while 48.8% had macroscopic nodal involvement (pN1-pN3). Sixteen patients (18.6%) had either micrometastases or ITC identified by immunohistochemistry.
Associations with clinicopathological features: risk factors for lymph node metastasis
The clinicopathologic characteristics of GC patients with and without Mic or ITC are summarised in Table 1.
No statistically significant differences were observed among the three cohorts: ITC+ (lymph nodes with isolated tumour cells only), Mic+ (lymph nodes with micrometastases only), and ITC+/Mic+ (lymph nodes with either isolated tumour cells or micrometastases). Baseline clinicopathological characteristics were comparable across cohorts, including age, sex, tumour location, histologic type, tumour differentiation grade, non-oncologic mortality, chemotherapy modality, and pathological tumour-node-metastases (pTNM) stage.
Tumour size and lymphovascular invasion emerged as relevant risk factors: tumours >20 mm were significantly more likely to have ITC+/Mic+ nodes than tumours ≤20 mm (18.6% vs 2.3%, p=0.029). Lymphatic invasion and venous invasion were both associated with a higher frequency of ITC+/Mic+ (each p=0.035). ITC+/Mic+ was also associated with lower nodal categories (p=0.042).
Overall cohort
Kaplan-Meier analysis showed no significant difference in OS between patients with (ITC+/Mic+) and without micrometastases (ITC-/Mic-). The overall five-year recurrence rate was 30.6%. When patients were stratified by pathological TNM stage, the presence of ITC+/Mic+ did not significantly affect OS in any subgroup (Figure 2). Similarly, when survival was analysed according to pathological nodal status (pN0-pN3), ITC/Mic status had no significant impact on OS (pN0: p=0.464; pN1: p=0.837; pN2: p=0.128; pN3: p=0.910; Figure 3).
Test of equality of survival distributions for the presence of ITC or Mic in different stagesKaplan-Meier overall survival curves comparing patients with occult nodal disease (ITC+/Mic+) versus those without occult nodal disease (ITC-/Mic-), stratified by pathological tumour-node-metastases (TNM) stage (I–III). P-values shown in each panel correspond to log-rank tests comparing survival distributions between groups within each stage.ITC - isolated tumour cells; Mic - micrometastases
Test of equality of survival distributions for the presence of ITC or Mic in different pN stagesKaplan-Meier overall survival curves comparing patients with occult nodal disease (ITC+/Mic+) versus those without occult nodal disease (ITC-/Mic-), stratified by pathological nodal category (pN0-pN3). Group differences were assessed using log-rank tests, with p-values reported for each pN stratum.ITC - isolated tumour cells; Mic - micrometastases; pN0 - node-negative; pN0-pN3 - node-positive
pN0 and perioperative subgroups
Among the 44 patients classified as pN0 on conventional histology, cytokeratin immunostaining revealed occult nodal disease in six patients (13.6% of pN0; 7% of the entire cohort). In this group, 20 of 946 lymph nodes initially reported as negative (2.11%) were found to contain tumour deposits (six nodes with micrometastases and 14 with ITC).
A subset of patients who received perioperative chemotherapy observed a significant association between occult nodal disease and OS. In these patients, the presence of micrometastatic nodal involvement detected by immunohistochemistry was associated with a higher recurrence rate (p=0.023; Figure 4), suggesting a potential prognostic role for ITC/Mic status.
Test of equality of survival distributions for the presence of ITC or Mic with perioperative chemotherapyKaplan-Meier curves in the subgroup treated with perioperative chemotherapy, comparing outcomes between patients with occult nodal disease (ITC+/Mic+) and those without occult nodal disease (ITC-/Mic-). The log-rank test indicates a significant difference between curves (p=0.023), suggesting an association between occult nodal disease and higher relapse risk in this subgroup.ITC - isolated tumour cells; Mic - micrometastases
Comparison of pN0 with ITC+/Mic+ vs pN1
The Kaplan-Meier analysis comparing OS between patients with pN0 disease with ITC+/Mic+ and those with pN1 nodal involvement shows largely overlapping survival curves throughout the follow-up period. Both groups maintain estimated survival above roughly 70% at five years, and no clear separation of the curves is observed.
There was no statistically significant difference in survival between the two groups (p=0.624, Figure 5), indicating that patients with micrometastatic nodal disease classified as pN0 do not experience significantly different overall survival compared with patients classified as pN1.
Test of equality of survival distributions for the presence of ITC or Mic in pN0 and pN1Kaplan-Meier overall survival curves comparing patients classified as pN0 on conventional histology but harbouring occult nodal disease on immunohistochemistry (pN0 with ITC+/Mic+) versus patients with overt pN1 disease. Survival distributions were compared using a log-rank test (p=0.624), showing no statistically significant difference between groups.ITC - isolated tumour cells; Mic - micrometastases; pN0 - node-negative; pN1 - node-positive
Discussion
In this single-centre cohort, we observed that micrometastases and ITC affected a non-negligible proportion of patients. Sixteen patients (18.6%) had either micrometastases or ITC, indicating that a relevant subset of patients carried occult nodal tumour cells detectable exclusively by IHC.
In patients staged as pN0 by routine histology, cytokeratin immunostaining revealed previously unidentified tumour cells in six cases (13.64%), corresponding to 7% of the overall cohort. These findings are somewhat lower than the 20-30% prevalence of micrometastases reported in several series that employed serial sectioning, but they are consistent with the wide range observed in the literature and likely reflect methodological differences, including the number of sections per node [13,14].
Consistent with previous reports, we identified specific histopathological features associated with micrometastatic disease. Tumour size greater than 20 mm and the presence of lymphovascular invasion were significantly associated with a higher prevalence of micrometastatic lymph-node involvement. The proportion of patients with ITC+/Mic + was 18.6% among tumours >20 mm compared with 2.3% among smaller tumours. These findings support the concept that micrometastatic spread is not a random event but rather a marker of a more biologically aggressive phenotype marked by enhanced lymphovascular dissemination.
Despite this, our survival analysis did not demonstrate a clear adverse impact of these cells on overall prognosis in the study population as a whole. Kaplan-Meier curves showed no significant difference in OS between patients with and without lymph node metastasis, either when stratified by pathological TNM stage or by nodal category (pN0-pN3). These observations place our results closer to those series in which micrometastases were not identified as a prognostic factor and contrast with meta-analytic data suggesting a consistently negative impact of micrometastatic disease on long-term outcomes [15].
A potentially clinically relevant result was observed from the subgroup of patients treated with perioperative chemotherapy. In this subset, the presence of Mic or ITC was associated with a significantly lower OS (p=0.023), suggesting that occult nodal disease might have prognostic value in these patients. One possible explanation is that micrometastatic involvement identifies a subgroup with higher systemic dissemination potential, in whom perioperative chemotherapy may be insufficient to eradicate residual nodal disease. Alternatively, this association may partly reflect selection bias and the small number of events. We also compared survival between patients with pN0 disease with ITC+/Mic + and those with overt pN1 nodal involvement. Interestingly, Kaplan-Meier curves showed substantial overlap, and the log-rank test revealed no significant difference in OS between these groups (p=0.624). Although our study was underpowered to draw definitive conclusions, this finding suggests that micrometastatic nodal disease may, in prognostic terms, behave more similarly to limited macrometastatic involvement (pN1) than to truly node-negative disease. This observation is consistent with the stage-migration hypothesis proposed in other series, in which the inclusion of micrometastases in the count of positive nodes tends to align survival more closely with higher N categories [14-15]. From a surgical perspective, our data confirm the feasibility of achieving adequate nodal retrieval in routine practice, with a mean of approximately 23 lymph nodes examined per specimen, in accordance with D2 lymphadenectomy standards. A small proportion of lymph nodes exhibit occult tumour deposits detectable only by IHC, underscoring the intrinsic limitations of single-section H&E evaluation. Nevertheless, given that micrometastases and ITC did not significantly affect OS in the overall cohort, routine immunohistochemical assessment of all patients with gastric cancer does not appear justified based on our results.
The present study has several limitations that must be acknowledged. It is a retrospective, single-centre study with a relatively small sample size, which limits statistical power, particularly in subgroup analyses. The number of patients with ITC+/Mic+ and the number of recurrences were modest, increasing the risk of type II error and potentially masking subtle prognostic effects. Furthermore, our methodology did not include exhaustive serial sectioning of all lymph nodes, which may have led to underestimation of other small deposits. Despite these limitations, our findings contribute to the existing literature by providing contemporary data from a Western cohort treated with radical gastrectomy with D2 surgery and perioperative therapy.
Considering all available evidence, our study results suggest that, while micrometastases and ITC are biologically meaningful and associated with adverse histopathological features, their prognostic impact on long-term survival may be limited. Their role may be more subtle, potentially refining risk stratification in specific subgroups, such as those receiving perioperative chemotherapy, rather than serving as a universal indicator of poor prognosis.
Conclusions
Micrometastases and isolated tumour cells were detected in nearly one-fifth of patients, most often in association with larger tumours and lymphovascular invasion. However, their presence did not affect overall survival in the cohort, and outcomes in pN0 patients with micrometastases were similar to those of pN1 patients. A prognostic effect was observed exclusively in patients receiving perioperative chemotherapy, in whom micrometastases or ITC were linked to a lower OS. This technique appears to reveal features of a more aggressive tumour phenotype but, by itself, does not justify routine use. Prospective, standardised studies are needed to clarify their role in staging and treatment decision-making.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prognostic significance of the number of positive lymph nodes in gastric carcinoma Br J Surg Adachi Y Kamakura T Mori M Baba H Maehara Y Sugimachi K 414416811994817391610.1002/bjs.1800810331 · doi ↗ · pubmed ↗
- 2Gastric cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up Ann Oncol Lordick F Carneiro F Cascinu S 100510203320223591463910.1016/j.annonc.2022.07.004 · doi ↗ · pubmed ↗
- 3Proliferative activity of micrometastases in the lymph nodes of patients with gastric cancer Br J Surg Yonemura Y Endo Y Hayashi I Kawamura T Yun HY Bandou E 7317369420071737793010.1002/bjs.5604 · doi ↗ · pubmed ↗
- 4Benefits of D 2 lymph node dissection for patients with gastric cancer and p N 0 and p N 1 lymph node metastases Br J Surg Siewert JR Kestlmeier R Busch R 11441147831996886933010.1002/bjs.1800830836 · doi ↗ · pubmed ↗
- 5Gastric carcinoma: stage migration by immunohistochemically detected lymph node micrometastases Gastric Cancer Jeuck TL Wittekind C 1001081820152455006610.1007/s 10120-014-0352-4 · doi ↗ · pubmed ↗
- 6Lymph node micrometastases in early gastric cancer and their impact on prognosis World J Surg Morgagni P Saragoni L Scarpi E Zattini PS Zaccaroni A Morgagni D Bazzocchi F 5585612720031271522310.1007/s 00268-003-6797-y · doi ↗ · pubmed ↗
- 7Detection and clinical significance of lymph node micrometastasis in gastric cardia adenocarcinoma J Int Med Res Ru Y Zhang L Chen Q 2932994020122242936810.1177/147323001204000129 · doi ↗ · pubmed ↗
- 8Prognostic implication of isolated tumor cells and micrometastases in regional lymph nodes of gastric cancer World J Gastroenterol Lee HS Kim MA Yang HK Lee BL Kim WH 592059251120051627360010.3748/wjg.v 11.i 38.5920 PMC 4436711 · doi ↗ · pubmed ↗