Epidemiological Landscape of Breast Cancer in Northern India: A Narrative Review of Jammu and Kashmir
Gita Devi, Mittal Rathod, Mehul Kaliya, Aneri Rathod

TL;DR
This paper reviews breast cancer trends in Jammu and Kashmir, highlighting late diagnosis, low awareness, and high psychological stress among patients.
Contribution
The study provides a synthesized overview of breast cancer epidemiology and psychosocial factors in Jammu and Kashmir, emphasizing regional-specific challenges.
Findings
Breast cancer in J&K is diagnosed at a younger age and later stages, particularly in Kashmir.
Low screening rates and awareness contribute to delayed detection and high psychological burden.
Infiltrating ductal carcinoma and HR+/HER2- subtype are most common in the region.
Abstract
Breast cancer is increasingly affecting younger women across India, with the Union Territory (UT) of Jammu and Kashmir (J&K) experiencing a similar shift. Limited regional data and poor screening access contribute to late diagnosis and high psychosocial burden, necessitating a synthesized evaluation of existing evidence. The objective of this review is to summarize and critically appraise the published literature on breast cancer in Jammu and Kashmir, with a specific focus on its epidemiology, clinical characteristics, molecular subtype distribution, awareness levels, and psychosocial determinants. A narrative review approach was adopted. Studies published in English and conducted within J&K were searched through PubMed, MEDLINE, and Google Scholar. Eligible studies included those reporting epidemiology, staging, molecular patterns, risk awareness, and mental-health outcomes. Data were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
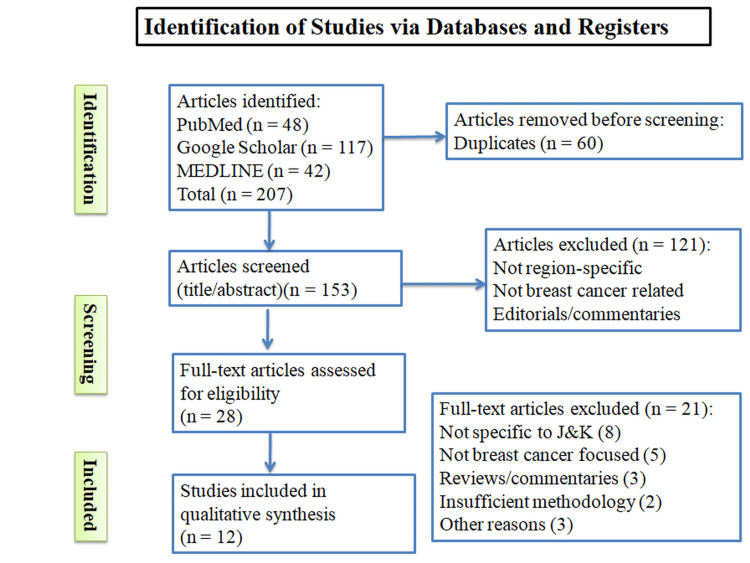 Figure 1
Figure 1| Sr. No. | Year | Journal | Title and authors | Study type (n) | Study population | Study area | Study tool | Objectives |
| 1 | 2023 | JK Science | Kumari et al. Prevalence and determinants of anxiety disorders among females with breast cancer attending a tertiary care hospital in Jammu [ | Hospital-based cross-sectional (n=275) | Females ≥ 18 years with confirmed breast cancer | Jammu (Tertiary Care Hospital) | Structured questionnaire (anxiety screening) | To determine the prevalence of anxiety disorders and assess socio-demographic and clinical determinants. |
| 2 | 2023 | J Cancer Res Ther | Mir et al. Psychiatric comorbidities and breast cancer: a study from Jammu region of UT of J&K, India [ | Cross-sectional (n=205) | Females ≥ 18 years with breast cancer | Jammu (Regional Cancer Centre) | Self-designed proforma + HADS + PSS-10 | To assess psychiatric comorbidities and associations with demographic/clinical factors. |
| 3 | 2020 | Int Health Res J | Javaid et al. Knowledge and practice of breast cancer screening and awareness of its risk factors among reproductive women of Jammu & Kashmir [ | Community-based cross-sectional (n=387) | Women aged 15-45 years from he general population | Jammu and Kashmir (urban + rural) | Structured questionnaire (awareness and screening) | To assess awareness of risk factors and screening practices among reproductive-age women. |
| 4 | 2021 | Health Promot Int | Hamid et al. Lived experiences of women suffering from breast cancer in Kashmir: a phenomenological study [ | Qualitative phenomenological (n=12) | Women ≥ 18 years; diagnosed ≥ 6 months earlier | Kashmir (various districts) | In-depth interviews (snowball + theoretical sampling) | To explore lived experiences, challenges, and coping strategies of women with breast cancer. |
| 5 | 2019 | Ann Int Med Den Res | Paul et al. Patterns of failure in breast cancer patients of Kashmir Valley [ | Retrospective observational (n=212) | Biopsy-proven breast cancer patients treated at tertiary centre | Kashmir Valley | Hospital records + follow-up data | To analyze local, regional, and distant failure patterns after treatment. |
| 6 | 2021 | J Community Med | Khursheed et al. Epidemiological studies on breast cancer in Kashmir Valley [ | Secondary data analysis (n=226) | Female patients aged 19-78 years, pathological breast cancer | Kashmir Valley | Hospital cancer registry dataset | To describe epidemiological characteristics of breast cancer cases attending tertiary centre. |
| 7 | 2017 | Surg Sci | Mir et al. Clinicopathological profile of breast cancer patients at a tertiary care hospital in Kashmir Valley [ | Hospital-based cross-sectional observational (total malignant cases n=34) | Males and females, aged 22-60 years, histopathologically confirmed breast cancer | Kashmir Valley (GMC Srinagar) | Clinical evaluation, histopathology, record review | To determine demographic, clinical, pathological, and staging profile of breast cancer in Kashmir. |
| 8 | 2017 | Indian J Comput Sci Eng | Nisa et al. Survey of patients with cancer in Jammu & Kashmir: based on hospital registry records [ | Hospital-based registry retrospective survey (total n=6359; breast cancer subset n=234) | All cancer patients; breast cancer subset analyzed | Jammu and Kashmir (four major hospitals) | Review of hospital registry records | To describe cancer site distribution, age/sex distribution among cancers, including breast cancer in J&K. |
| 9 | 2024 | J Cancer Res Ther | Banday et al. Receptor subtype and outcomes of breast cancer - single-center experience from North India [ | Retrospective cohort (n=944) | Female, biopsy-proven breast cancer patients treated 2014-2018 | Kashmir (SKIMS, Srinagar) | Hospital records; pathology and IHC data; follow-up records | To determine molecular subtype distribution and compare survival across subtypes. |
| 10 | 2024 | BMC Public Health | Gupta et al. The Chiraiya Project: retrospective analysis of breast cancer detection gaps via mobile mammography in Jammu Province, India [ | Retrospective observational screening (n=1505 screened) | Women ≥ 40 years, general population | Jammu Province, J&K (urban + rural) | Mobile mammography; BI-RADS + structured database | To analyze detection gaps, follow-up adherence, urban-rural uptake, feasibility of mobile mammography in underserved areas. |
| Study | Domain of Study | Key Findings | Implications for J&K |
| Kumari et al. [ | Psychological morbidity (anxiety disorders) | High prevalence of panic disorder, PTSD, and agoraphobia; rural residence and age/family type associated with higher PTSD/agoraphobia rates. | Need for integrated mental-health services for oncology patients. |
| Mir et al. [ | Psychiatric comorbidity (depression, anxiety, stress) | High burden of depression and anxiety; associated with parity, hospital visits, duration since diagnosis, treatment type. | Psychological screening should be integrated into routine breast cancer care. |
| Javaid et al. [ | Awareness and screening practices (general population) | Low awareness of symptoms and risk factors; poor screening uptake; younger women are somewhat more informed. | Targeted awareness campaigns and community education, especially for older women needed. |
| Hamid et al. [ | Lived experiences and coping mechanisms | Women reported serious psychological, social, financial, and emotional challenges; coping through spirituality, family support, and emotional venting. | Psychosocial support and stigma-reduction interventions essential. |
| Paul et al. [ | Patterns of failure (post-treatment) | Significant rates of local, regional, and distant recurrences; infiltrating ductal carcinoma is common. | Strengthened follow-up protocols and early detection of recurrence required. |
| Khursheed et al. [ | Epidemiological profile | Younger age at diagnosis; early menarche identified as risk factor; majority present at advanced stages. | Urgent need for screening, awareness, and early-detection strategies. |
| Mir et al. [ | Clinicopathological profile | High proportion presenting in stage III; infiltrating ductal carcinoma predominant. | Indicates delayed presentation - emphasizes need for community outreach and timely Refral. |
| Nisa et al. [ | Cancer registry-based survey | Breast cancer among top reported cancers; data limited to hospital-based registry; under-reporting probable. | Population-based cancer registry establishment needed for accurate disease burden assessment. |
| Banday et al. [ | Molecular subtype distribution and outcomes | HR+/HER2- subtype most common (44.5%); TNBC 15.7%, associated with worst survival outcomes. | First molecular profile for J&K - informs subtype-specific treatment and prognosis. |
| Gupta et al. [ | Screening-gap analysis via mobile mammography | Screening outreach to 1,505 women; detection gaps, poor follow-up, urban-rural disparities were observed. | Mobile screening shows promise, but follow-up and Refral systems must be strengthened. |
| Parameter | Findings from Jammu-based studies [ | Findings from Kashmir-based studies [ | Overall Interpretation/trend |
| Age at diagnosis | Limited data - mainly psychological studies, age ≥ 18 years; no precise staging or histopathology data | Clinical studies report diagnosis between late 30s and early 60s; younger onset cases exist | Early-onset trend seen in Kashmir; Jammu lacks clinical cohort data |
| Stage at presentation | Not reported | High proportion present at stage III (70-73%) | Late-stage presentation is common; region-wide challenge |
| Most common symptoms | Not reported | Breast lump most frequent; nipple discharge, skin changes also observed | Clinical symptom and presentation data predominantly from Kashmir |
| Histopathology | Not available | Infiltrating ductal carcinoma predominant in pathology reviews | Infiltrating ductal carcinoma is dominant subtype in region; clinical data from Kashmir essential |
| Molecular subtypes | Not reported | HR+/HER2- most common; TNBC significant (15.7%) with poorer prognosis | Molecular profiling limited to Kashmir; critical data gap for Jammu |
| Psychiatric and psychosocial impact | High anxiety, depression, stress [ | High psychosocial burden described in phenomenological study [ | Psychological distress common across both divisions; need for mental-health integration |
| Awareness and screening uptake | Low awareness; poor screening practices [ | Mobile screening shows reach but follow-up gaps and rural-urban disparity [ | Screening coverage limited; both community awareness and structured programmes needed |
| Recurrence / treatment failure patterns | Not reported | Documented local, regional, distant failures [ | Follow-up care and surveillance critical post-treatment |
| Cancer registry and surveillance data | Registry-based survey includes cancer distribution but limited clinical detail | Hospital-based epidemiological and pathology data [ | Kashmir offers richer clinical datasets; Jammu relies on registry - need integrated registry + clinical data |
| Screening initiatives and innovation | No community-level screening innovation reported | Mobile mammography implemented in underserved areas [ | Mobile screening is a viable model for broader coverage; needs support for follow-up |
| Domain | Jammu | Kashmir | Relevance to breast cancer research |
| Urbanization | Higher | Lower | Affects access to screening and diagnostics |
| Major cities | Jammu | Srinagar | Concentration of tertiary care |
| Health facilities | Relatively better distributed | Concentrated in few centers | Influences reporting and early diagnosis |
| Female literacy | Relatively higher | Lower in some districts | Affects awareness and care-seeking |
| Research institutions | More medical colleges | Fewer centers | Influences volume of publications |
| Cancer surveillance | Limited | Limited | Under-reporting in both regions |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Cancer Incidence and Screening · Breast Cancer Treatment Studies · Digital Radiography and Breast Imaging
Introduction and background
Breast cancer is the most common malignancy among women worldwide, and its burden is rising rapidly across India, including the Union Territory (UT) of Jammu and Kashmir (J&K) [1-3]. The incidence of breast cancer in India has increased by nearly 39% between 1990 and 2016, reflecting a significant epidemiological transition [4]. In 2020, breast cancer accounted for 13.5% of all cancer cases and 10.6% of all cancer-related deaths in the country [2]. Recent trends also indicate a shift toward a younger age at diagnosis, with a growing proportion of cases presenting in pre-menopausal women. Detecting cases at advanced stages leads to higher treatment costs and worse clinical outcomes, underscoring the need for early identification.
The Government of India, through the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases, and Stroke (NPCDCS), has outlined operational guidelines and standardized recommendations for breast cancer screening and early detection [5, 6]. Despite these initiatives, substantial challenges persist. Delays in diagnosis, inadequate referral pathways, limited community awareness of risk factors and screening methods, and suboptimal knowledge even among healthcare professionals continue to impede early detection [1, 6]. Socio-cultural barriers, stigma, and unequal access to diagnostic facilities further exacerbate these gaps.
A preliminary scan of available literature reveals a marked imbalance between the Jammu and Kashmir divisions. Research from Jammu is modest, focusing primarily on psychiatric comorbidities, awareness, and general cancer patterns [7-9]. In contrast, Kashmir has produced more extensive biomedical literature, including phenomenological accounts, analyses of treatment failures, epidemiological assessments, and clinicopathological profiles [10-14]. This asymmetry highlights critical evidence gaps, particularly regarding epidemiological determinants, demographic distribution, clinical characteristics, and screening practices in Jammu.
Jammu and Kashmir was selected for focused review due to its unique geopolitical and health-system context. Evidence from fragile and conflict-affected settings indicates that prolonged instability adversely affects continuity of care, preventive services, and access to early diagnosis [15]. Geographic barriers and sociocultural determinants further contribute to delayed breast cancer detection in India [16]. Recent National Council on Radiation Protection and Measurements (NCRP)-based analyses highlight persistent regional gaps in cancer surveillance and burden estimation, underscoring the need for region-specific synthesis [17].
Given these considerations, this review synthesizes available evidence on breast cancer in J&K, examining epidemiology, risk factors, screening and diagnostic pathways, and management. A clearer understanding of the regional burden can help strengthen early detection, improve outcomes, and guide policy and public health interventions tailored to the unique context of the UT.
The absence of a formal risk of bias assessment represents a limitation of this narrative review and should be considered when interpreting the findings.
Review
Methods
This review adopted a narrative synthesis approach to summarize current evidence on breast cancer epidemiology, risk factors, screening practices, and diagnostic pathways in the Union Territory of Jammu and Kashmir. A narrative review methodology was adopted due to the limited number of region-specific studies from the Union Territory of Jammu and Kashmir and marked heterogeneity in study designs and outcome reporting. As the available evidence included diverse methodologies - ranging from hospital-based and registry studies to qualitative and community surveys - a systematic review or PRISMA-based meta-analysis was not feasible. A narrative approach was therefore used to synthesize fragmented evidence and provide contextual clinical and public health interpretation relevant to this region. A comprehensive literature search was performed on PubMed, MEDLINE, and Google Scholar for studies published between January 2000 and December 2024, using a combination of Medical Subject Headings (MeSH) and free-text keywords such as "breast cancer", "carcinoma breast", "Jammu", "Kashmir", "epidemiology", "risk factors", "screening", and "clinicopathological profile", with Boolean operators (AND, OR). Additionally, reference lists of included studies were manually screened to identify relevant articles, while grey literature, non-indexed publications, and dissertations were excluded to maintain scientific rigor. Two independent reviewers screened titles and abstracts, followed by full-text assessment of potentially eligible articles. Duplicate records were removed manually. Disagreements were resolved by discussion and consensus.
Studies were included if they focused specifically on breast cancer in the Jammu and Kashmir region, reported epidemiological trends, risk factors, clinicopathological profiles, or screening and diagnostic practices, were original research articles published in peer-reviewed journals, and were available in English. Studies were excluded if they did not pertain to Jammu and Kashmir, addressed cancers other than breast cancer, were review articles, commentaries, editorials, or conference abstracts, or were non-English publications or lacked adequate scientific rigor.
Data extraction was carried out using a predefined template that captured author details, year of publication, study design and journal, sample size and study setting, epidemiological indicators such as incidence, prevalence, mortality, and stage at diagnosis, assessed risk factors, and information on screening and diagnostic practices. Two reviewers independently extracted data to ensure accuracy and minimize bias. Owing to methodological heterogeneity across studies, a narrative synthesis approach was employed, with findings organized thematically to highlight epidemiological patterns, risk determinants, screening practices, and regional disparities between Jammu and Kashmir. Quality assessment focused on journal indexation, clarity of methodology, appropriateness of sampling, and completeness of reporting, though no formal risk-of-bias tool was applied because of the diversity in study designs. Ethical approval was not required as the review analyzed secondary data from published sources, and all studies were duly cited. The review was not registered on PROSPERO, as narrative reviews are generally not eligible for registration.
A total of 207 records were identified through database searches (PubMed: 48, Google Scholar: 117, and MEDLINE: 42), and an additional six records were found from other sources. After removing duplicates, 153 records were retained for screening, all of which underwent title and abstract review. Of these, 121 were excluded, and 32 full-text articles were sought for retrieval. Four full texts could not be obtained, leaving 28 articles assessed for eligibility. Twenty-one articles were excluded, mainly for not being specific to Jammu and Kashmir (n=8), not focusing on breast cancer (n=5), being reviews or commentaries (n=3), having insufficient methodology (n=2), or other reasons (n=3). Ultimately, 12 studies met the inclusion criteria and were incorporated into the qualitative synthesis (Figure 1).
PRISMA flow diagram showing identification, screening, eligibility assessment and inclusion of studiesPRISMA - Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Results
Epidemiological Characteristics and Age Profile
The literature indicates a distinct epidemiological pattern of breast cancer in the Union Territory of Jammu and Kashmir, characterized by a younger age of onset than commonly documented in high-income regions. Evidence from Kashmir shows that most women present with the disease in their late 30s to early 60s, suggesting a predominantly pre-menopausal burden [12]. The age distribution reported in clinical cohorts from tertiary settings aligns with national trends of rising breast cancer among younger Indian women. Registry-based findings from Jammu and Kashmir further establish breast cancer as a major malignancy among females; however, granular clinical age data remain limited within registry-only outputs [14]. Table 1 provides an overview of studies documenting such characteristics, while Table 2 emphasizes early menarche as a recurrent epidemiological determinant in Kashmir cohorts, reflecting shifting reproductive profiles within the region. As summarized in Table 3, this evidence demonstrates greater clinical depth from Kashmir, whereas research output from Jammu remains focused on psychosocial aspects rather than epidemiological stratification.
Stage at Presentation and Disease Progression
Across available clinical datasets, late-stage diagnosis emerges as a dominant challenge. Studies from tertiary centers in Kashmir reveal that more than 70% of patients present with stage III breast cancer at diagnosis, whereas only around 27% report at stage II [13]. This skewed stage distribution suggests poor symptom recognition, delayed health-seeking behavior, and limited access to structured screening pathways. Complementary evidence from a treatment outcome analysis underscores high rates of local, regional, and distant failures, suggesting that delays likely extend beyond initial diagnosis to include inadequate post-treatment surveillance and follow-up [11]. These patterns highlight critical weaknesses within both early detection and survivorship care in the UT. Table 2 consolidates these failure patterns, while Table 3 reinforces that such clinical insights originate exclusively from Kashmir, leaving a significant evidence gap on disease staging and progression in Jammu.
Molecular Profile and Histopathological Characteristics
Histopathological evaluation across Kashmiri cohorts consistently identifies infiltrating ductal carcinoma (IDC) as the most common tumor subtype [13], a pattern concordant with Indian and global distributions. However, the molecular subtype distribution adds an important layer to regional clinical management. A large tertiary-center cohort study from Kashmir documented that hormone receptor-positive, HER2-negative (HR+/HER2-) tumors constituted the predominant subtype (44.5%), whereas triple-negative breast cancer (TNBC) accounted for 15.7% of all cases [18]. TNBC was associated with significantly poorer survival outcomes and more aggressive disease trajectories, indicating the need for timely subtype-specific management. These molecular findings, presented in Table 2, offer critical prognostic and therapeutic implications for the region. As seen in Table 3, such molecular datasets are currently exclusive to Kashmir, indicating the absence of comparable data from Jammu and underscoring the need for region-wide tumor profiling.
Awareness Levels, Screening Practices, and Accessibility Initiatives
Despite evidence of younger disease onset, community-level awareness and screening remain disappointingly low. A cross-sectional population-based survey reported inadequate knowledge of breast cancer symptoms, risk factors, and screening modalities among women, particularly those above 40 years of age [9]. Even though younger women demonstrated relatively higher awareness, this did not translate into sustained screening practices. These behavioral inconsistencies contribute directly to delayed presentation, as reflected in the high proportion of late-stage diagnoses [13]. Efforts to bridge diagnostic gaps have been demonstrated through the "Chiraiya" mobile mammography project in Jammu Province, which screened 1505 women aged ≥40 years and revealed disparities in rural uptake and poor follow-up adherence [19]. Table 1 captures the screening intervention methodology, while Table 3 highlights the initiative's implications for equitable screening access. This model illustrates that mobile units may offer scalable public health solutions in geographically challenging areas of the UT, provided systematic recall and referral mechanisms are strengthened.
Psychosocial and Mental Health Burden
The psychosocial dimension of breast cancer care is particularly visible in research from Jammu, where multiple studies highlight a high burden of anxiety, depression, stress, and post-traumatic stress disorders among patients [7, 8]. Determinants include rural residence, treatment modality, time since diagnosis, parity, and family structure. Qualitative exploration from Kashmir further reveals the lived emotional distress associated with breast cancer, including stigma, socioeconomic insecurity, and reliance on coping mechanisms such as spirituality and family support [10]. As summarized in Tables 1 and 2, these findings make a compelling case for integrating structured psychological screening and support into oncology services across the UT. Table 3 demonstrates that while clinical data are richer for Kashmir, psychosocial evidence is concentrated in Jammu, highlighting the need for comprehensive bilateral data integration.
Discussion
While the reviewed studies frequently highlight differences between Jammu and Kashmir, these differences are best understood in the context of broader demographic, socioeconomic, and health-system characteristics as depicted in Table 4.
Jammu is relatively more urbanized, with higher population concentration around major cities such as Jammu city, and comparatively better access to tertiary health-care facilities. In contrast, Kashmir has a higher proportion of rural and geographically dispersed populations, with access to specialized oncology services concentrated in a limited number of urban centers. Differences in female literacy, health-seeking behavior, and availability of diagnostic infrastructure may further influence stage at presentation and reporting of breast cancer cases. Variations in medical education institutions, research activity, and cancer surveillance capacity across the two regions may also contribute to the observed imbalance in published literature. These contextual factors should be considered when interpreting apparent regional differences in breast cancer epidemiology [15].
Breast cancer in Jammu and Kashmir reflects an evolving epidemiological profile similar to the recent shifts observed globally, where rising incidence among younger women has been attributed to changing reproductive behaviors, hormonal influences, obesity, and delayed childbearing [20]. Regional findings in Kashmir showing early-age onset and premenopausal diagnosis align with this global risk-transition model [12-14]. Furthermore, the predominance of HR+/HER2- tumors and a substantial proportion of TNBC cases in Kashmir highlight the growing importance of biomarker-based management, which is increasingly emphasized in international breast cancer care frameworks [10].
In addition to clinical gaps, psychosocial morbidity is a prominent and under-recognized dimension in breast cancer care within the UT. High prevalence of depression, anxiety, and PTSD among patients in Jammu [7, 8] echoes international evidence asserting that quality of life and treatment response are negatively affected when emotional distress is untreated [21]. These findings reinforce the need for an integrative care model in J&K that incorporates psycho-oncology services alongside conventional therapeutics.
Delayed presentation remains a persistent challenge in J&K, with over two-thirds of women presenting in stage III [13]. This parallels low-resource settings worldwide, where stigma, limited diagnostic infrastructure, and socioeconomic factors impede timely screening and care [22]. The success of the mobile mammography initiative in Jammu demonstrates that resource-appropriate screening approaches can improve early detection when properly linked with follow-up and referral pathways [16]. Such strategies reflect global recommendations advocating community-based outreach and mobile diagnostic models as viable solutions for underserved populations [22].
Therefore, the current evidence underscores three critical public health priorities for J&K: establishing a population-based cancer registry, expanding decentralized community-level screening programs, and incorporating structured psychological support into oncologic care. Implementing these components can narrow the disparity between Kashmir and Jammu research outputs and align J&K's health response with global cancer control goals.
Conclusions
Breast cancer in Jammu and Kashmir demonstrates a rising burden marked by younger age of onset, late-stage diagnosis, inadequate awareness, and substantial psychosocial morbidity. Kashmir contributes more evidence on clinical, pathological, and molecular profiles, whereas Jammu reflects significant psychological and community-based gaps. With most cases presenting beyond stage II, strengthened community screening, decentralized diagnostic services, and mental health integration are urgently required. Evidence from this review highlights the need to establish population-based cancer surveillance, multidisciplinary oncology services, and context-specific screening pathways, including mobile mammography programs, to improve early detection and reduce mortality. Such targeted interventions will help address the emerging epidemiological shift and bridge the disparity in breast cancer research and management across the Union Territory.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A review of breast cancer awareness among women in India: cancer literate or awareness deficit?Eur J Cancer Gupta A Shridhar K Dhillon PK 205820665120152623285910.1016/j.ejca.2015.07.008PMC 4571924 · doi ↗ · pubmed ↗
- 2Cancer statistics, 2020: report from National Cancer Registry Programme, India JCO Glob Oncol Mathur P Sathishkumar K Chaturvedi M 10631075620203267307610.1200/GO.20.00122 PMC 7392737 · doi ↗ · pubmed ↗
- 3Patterns of cancer in males and females in Jammu Region JK Science Gupta A Puri I Gupta M 4751232021 https://journal.jkscience.org/index.php/JK-Science/article/view/45
- 4Breast cancer in India: present scenario and the challenges ahead World J Clin Oncol Mehrotra R Yadav K 2092181320223543329410.5306/wjco.v 13.i 3.209PMC 8966510 · doi ↗ · pubmed ↗
- 5National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases & Stroke (NPCDCS) Operational Guidelines (2013-17)Cancer, Diabetes, Cardiovascular Diseases & Stroke (NPCDCS) Operational 202120132021 https://mohfw.gov.in/sites/default/files/Operational%20Guidelines%20of%20NPCDCS%20%28Revised%20-%202013-17%29_1.pdf
- 6Screening for breast cancer: cost-effective solutions for low- & middle-income countries Indian J Med Res Mishra GA Pimple SA Mittra I Badwe RA 22923615420213485443010.4103/ijmr.IJMR_2635_20PMC 9131750 · doi ↗ · pubmed ↗
- 7Prevalence and determinants of anxiety disorders among females with breast cancer attending a tertiary care hospital in Jammu JK Science Kumari R Mir MT Mahajan R 98103252023 https://journal.jkscience.org/index.php/JK-Science/article/view/187
- 8Psychiatric comorbidities and breast cancer: a study from Jammu region of UT of J&K, India J Cancer Res Ther Mir MT Kumari R Gupta RK Sharma R Gul N Langer B 05019202310.4103/jcrt.jcrt_1081_2238384017 · doi ↗ · pubmed ↗