Revision and postoperative complication rates of conversion total hip arthroplasty after cephalomedullary nailing of intertrochanteric femur fractures: a systematic review and meta-analysis
Harmon S. Khela, Harsh Wadhwa, Henry J. Wong, L. Henry Goodnough

TL;DR
This study finds that conversion total hip arthroplasty after failed femur fracture surgery has a 6.7% revision rate and higher risks compared to standard hip replacement.
Contribution
The study provides the first comprehensive meta-analysis of complication rates for cTHA after cephalomedullary nailing of intertrochanteric fractures.
Findings
Overall revision rate after cTHA was 6.7%, with cemented implants showing lower complication rates than cementless ones.
Cemented stems had significantly lower infection and dislocation rates compared to cementless and diaphyseal cementless stems.
Periprosthetic fracture rates were 5.9% overall, with cemented implants having the lowest rate at 3.2%.
Abstract
Management of failed intertrochanteric (IT) fracture fixation often requires conversion total hip arthroplasty (cTHA), but complication and reoperation rates remain poorly characterized in the literature. This study aimed to characterize revision and postoperative complication rates for cTHA after cephalomedullary nailing of IT fractures. A systematic review and meta-analysis was conducted following PRISMA guidelines. PubMed and Embase were queried for studies examining cTHA outcomes after prior cephalomedullary nailing for IT fractures. The primary outcome was revision rate, while secondary outcomes included rates of infection, dislocation, subsidence, and periprosthetic fracture (PPF). A random-effects model was employed to pool overall and implant-specific complication rates. Seventeen studies with 1,253 cTHA patients met inclusion criteria. Implant type was specified in 799 cases:…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
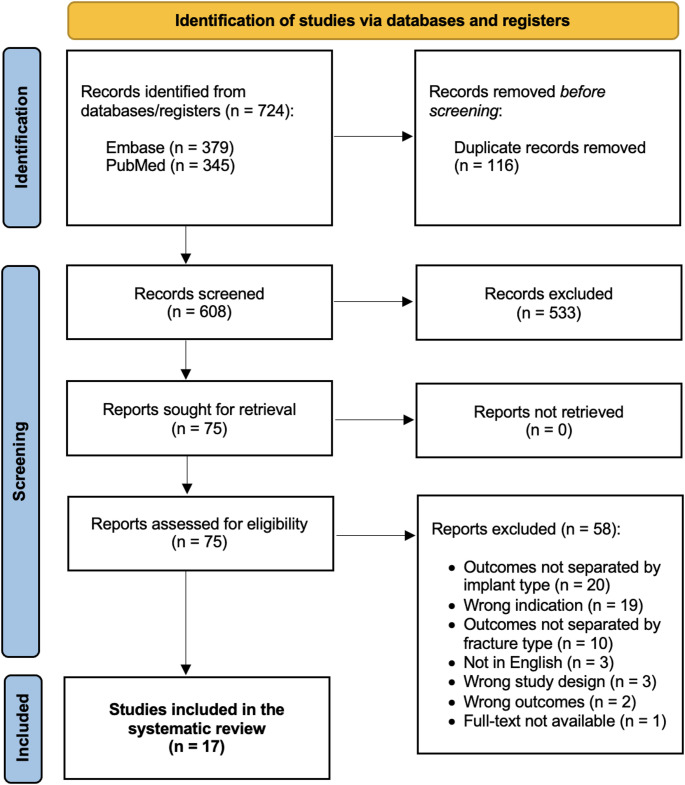 Figure 1
Figure 1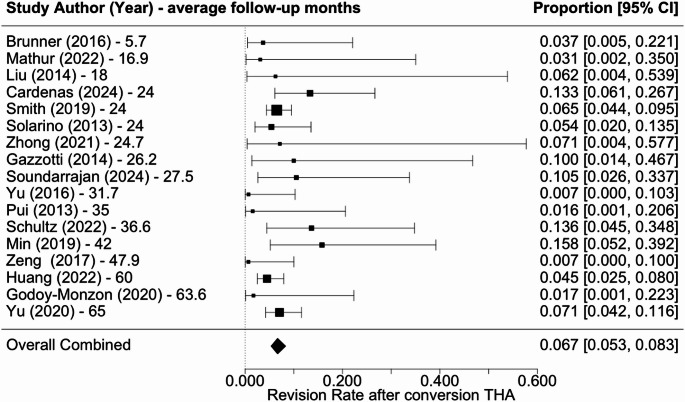 Figure 2
Figure 2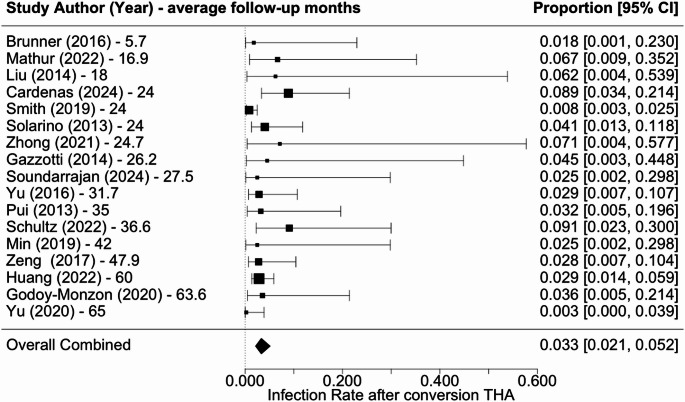 Figure 3
Figure 3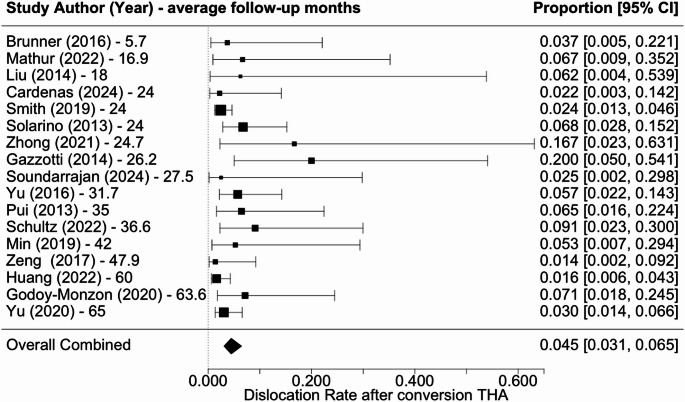 Figure 4
Figure 4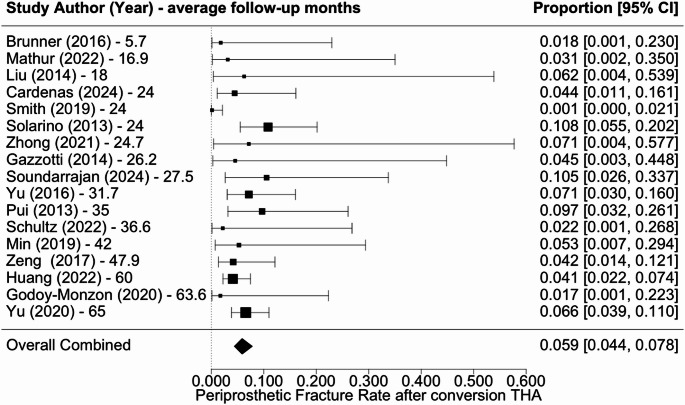 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Orthopaedic implants and arthroplasty · Bone health and osteoporosis research
Introduction
Intertrochanteric (IT) femur fractures are common injuries, especially among the elderly, accounting for 42.0% of all hip fractures [1]. The global incidence of hip fractures continues to rise as the population ages, with the total annual number of fractures projected to exceed 4.5 million by 2050 [2]. IT fractures are primarily managed with indirect reduction and internal fixation with cephalomedullary nails or dynamic hip screws. Despite advancements in fixation methods, fixation failure can occur due to mechanical complications like intramedullary nail cutout, delayed or incomplete fracture healing, postoperative infection, or the development of post-traumatic arthritis. Failure rates remain as high as 16%, particularly in osteoporotic patients [3].
The primary approaches for managing failed internal fixation of IT fractures are revision fixation or conversion to hemiarthroplasty or total hip arthroplasty. Treatment decision hinges on factors like bone quality, the failed fixation construct, and patient health conditions [4]. Among elderly patients, conversion total hip arthroplasty (cTHA) and hemiarthroplasty are widely accepted as effective salvage options when fixation devices fail [5]. cTHA is associated with extended operative time and increased blood loss relative to primary THA, due to the need for implant removal, revision strategies, and specialized components [6, 7]. cTHA for failed IT fracture fixation is also associated with prolonged hospital stays and higher costs compared to primary THA [6, 7]. Importantly, the timing and cause of failure often dictate the appropriate implant strategy. Tate et al. showed that early cTHA, defined as within 1 year of fracture fixation, was associated with significantly higher risks of reoperation, infection, periprosthetic fracture, dislocation, and medical complications compared to conversions performed after 1 year [8]. Grayson et al. corroborated these findings and found that patients undergoing early conversion within 6 months experienced nearly double the overall complication rate, including markedly higher rates of deep infection, revision surgery, and perioperative transfusion, compared to those converted after 6 months [9].
Despite the increasing use of conversion total hip arthroplasty (cTHA) as a salvage procedure after failed intertrochanteric fracture fixation, postoperative complication and revision rates remain variably reported, and implant-specific outcomes are poorly characterized. The primary aim was to estimate the pooled revision rate following cTHA after failed cephalomedullary nailing of intertrochanteric femur fractures. Secondary aims were to estimate pooled rates of postoperative infection, dislocation, periprosthetic fracture, and femoral stem subsidence. A secondary exploratory analysis was performed to descriptively summarize outcomes stratified by femoral component fixation strategy.
Methods
Search strategy
This systematic review and meta-analysis were performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [10]. A comprehensive search of the PubMed and Embase databases was completed on May 31, 2024, to identify articles reporting on outcomes following cTHA for patients who failed prior IT fracture fixation using keywords and medical subject headings. A combination of search terms such as “fracture fixation,” “open reduction and internal fixation,” “intertrochanteric,” “failure, “postoperative complications,” and “hip arthroplasty,” were used to query each database. The full search strategy can be found in Supplemental Table 1.
Inclusion and exclusion criteria
Search results were imported into Covidence (Melbourne, Australia), and duplicates were removed. Titles and abstracts were screened based on inclusion and exclusion criteria, followed by a full-text review to assess eligibility. Two authors (H.S.K. and H.W.) independently reviewed the studies, resolving any discrepancies through discussion to reach consensus. Studies were deemed eligible if they met the following inclusion criteria: (1) included a minimum of three patients who underwent cTHA for failed cephalomedullary nail fixation of IT fracture, (2) provided defined data for the patient population, (3) reported revision rate after cTHA, and (4) were published in English. Studies were included only if pertinent data on the patients who had prior cephalomedullary nail fixation could be separately extracted, even if the total cohort included patients who received other fixation types (plate, dynamic hip screw, etc.). Similarly, if a study included a cohort of patients with IT fractures and other fracture types (subtrochanteric, femoral neck, etc.) but did not stratify outcomes based on fracture type or fixation method, it was excluded. Studies were excluded if they (1) did not meet the inclusion criteria, (2) reported on patients with infection or tumor/pathologic fracture cases, or were (3) case reports, commentaries, systematic and literature reviews, or surgical technique articles, (4) not performed on human patients, or (5) not available in full text. Figure 1 provides an overview of the search strategy and screening process.
Fig. 1PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses) flowchart describing the systematic review process
Data collection
Two reviewers extracted data from each study using a standardized data form. The following data were extracted: authors and publication year, study design, sample size, follow-up duration, patient demographic characteristics, initial implant type, cTHA approach, implant used in cTHA, intraoperative details, and postoperative outcomes. Intraoperative data variables obtained were operative time, length of stay, estimated blood loss, and need for transfusion. Clinical outcomes and complications of interest were rates of revision, infection, dislocation, subsidence, PPF, and any other complications reported explicitly in the text. In studies where a fraction of the total cohort underwent cTHA, the patient demographics (sample size, mean age, and gender distribution) only for those who underwent THA was not typically available. Therefore, in these cases, the demographic data we extracted was for the entire sample. A subgroup analysis of studies that reported outcomes based on femoral component type was performed, though implant-specific stratification was inconsistently reported across the literature.
Risk of bias assessment
The methodological quality and risk of bias for each included study were assessed using the Newcastle-Ottawa Scale (NOS) [11]. This tool evaluates non-randomized studies based on three primary domains: selection of study groups, comparability of groups, and ascertainment of either exposure or outcome, depending on the study design. Each study was rated on a scale of up to nine points. Scores of 7–9 indicated low risk of bias, 4–6 indicated high risk of bias, and 0 to 3 indicated very high risk of bias. While NOS scores were used to describe overall study quality, sensitivity analyses stratified by risk-of-bias category were not performed due to the limited number of studies.
Data analysis
Statistical analyses were performed using R version 4.4.1 and the metafor package (version 4.60) [12]. To address rare outcomes, a logit transformation was applied with an adjustment of 0.5 for studies with zero counts in revision, infection, dislocation, and PPF rates. This continuity correction was applied to avoid exclusion of clinically relevant cohorts reporting no complications, although it may influence effect estimates for infrequent outcomes. Combined rates were estimated using random-effects models and displayed through forest plots to provide a visual summary of complications after cTHA across studies. Publication bias assessment was performed using funnel plots and small study effects were tested using Egger’s regression tests. Heterogeneity was evaluated using Cochran’s Q Test and quantified using Higgin’s I^2^ and τ^2^. All statistical tests used a two-sided significance level of ⍺ = 0.05.
Results
The initial search yielded 724 studies, with 116 duplicate records removed before screening. After screening the titles and abstracts of the remaining 608 studies, 533 were excluded based on predefined inclusion and exclusion criteria, leaving 75 full-text articles for further assessment. Following full-text review, an additional 58 studies were excluded (Fig. 1). Ultimately, 17 studies met the eligibility criteria and were included in this systematic review [13–29]. Most of these were retrospective cohort or case series studies, with 13 Level III and 4 Level IV studies.
The risk of bias was relatively low, with an average NOS score of 8 (Table 1). Publication bias and small-study effects were assessed for pooled outcomes using funnel plot inspection and Egger’s regression test. Visual inspection of the funnel plots did not demonstrate clear asymmetry. Formal assessment using Egger’s regression did not indicate statistically significant asymmetry (p > 0.05) (Supplemental Table 2). There was no significant concern for heterogeneity for revision rate (I^2^ = 0.0%, τ^2^ = 0.000), infection rate (I^2^ = 23.2%, τ^2^ = 0.194), dislocation rate (I^2^ = 27.9%, τ^2^ = 0.171), and periprosthetic fracture rate (I^2^ = 6.4%, τ^2^ = 0.027). This was further confirmed using Cochran’s Q test (p > 0.05).
Table 1. Newcastle-Ottawa scale risk of bias assessment of included studiesAuthor (year)Study designLevel of evidenceSelectionComparabilityOutcomeQualityRepresentativeness of exposed cohort (+)Selection of nonexposed cohort (+)Ascertainment of exposure (+)Outcome not present before study (+)Based on design and analysis (++)Assessment of outcomes (+)Follow-up length (+)Adequacy of follow-up cohorts (+)Brunner (2016)Retrospective Multicenter CohortLevel III+++++++7/9Cardenas (2024)Retrospective Multicenter CohortLevel III++++++++8/9Gazzotti (2014)Retrospective Case SeriesLevel IV+++++++7/9Godoy-Monzon (2020)Retrospective Case SeriesLevel IV++++++++8/9Huang (2022)Retrospective CohortLevel III++++++++8/9Liu (2014)Retrospective Case SeriesLevel IV++++++6/9Mathur (2022)Prospective Case SeriesLevel IV++++++++8/9Min (2019)Prospective CohortLevel III+++++++++9/9Pui (2013)Retrospective Multicenter CohortLevel III++++++++8/9Schultz (2022)Retrospective CohortLevel III+++++++++9/9Smith (2019)Retrospective CohortLevel III++++++++8/9Solarino (2013)Retrospective CohortLevel III+++++++7/9Soundarrajan (2024)Retrospective CohortLevel III+++++++7/9Yu (2020)Retrospective CohortLevel III++++++++8/9Yu (2016)Retrospective CohortLevel III++++++++8/9Zeng (2017)Retrospective CohortLevel III+++++++7/9Zhong (2021)Retrospective CohortLevel III+++++++7/9
Across all studies, there were a total of 1253 cTHAs performed. Of these, cTHA implant type was specified in 799 cases. The most common implants used were primary cementless stems (47.9%), followed by primary cemented (38.8%), diaphyseal cementless (12.0%), and diaphyseal cemented (1.3%) stems. Among the studies that further specified implant details, the diaphyseal revision stems were modular taper-fluted designs (n = 28) or full-coated distally loading stems (n = 15). For primary cementless stems, reported designs included metaphyseal-fitting implants such as the Corail, CLS, and Taperloc stems. For primary cemented stems, the Exeter Universal stem—a polished, tapered cemented design—was the most commonly reported. Several studies, however, did not provide sufficient detail to determine specific stem type. The median follow-up time among the included studies was 27.5 months (range: 5.7–65.0 months). An overview of the demographics and intraoperative details for each study is outlined in Tables 2 and 3, respectively.
Table 2. Study characteristics and demographicsAuthor (year)Study designSample sizeMean age (range or SD)Females (%)Mean follow-up, months (range or SD)Initial implantApproachNumber of cTHAsImplant type in cTHAImplant detailsBrunner (2016)Retrospective Multicenter Cohort5781 (8.9)46 (80.7)5.7Proximal femoral nail antirotation (n = 47)Trochanteric fixation nail (n = 10)–27––Cardenas (2024)Retrospective Multicenter Cohort4569.78 (12.14)32 (71.1)24Intramedullary nail (n = 45)–45––Gazzotti (2014)Retrospective Case Series1075.1 (12.67)9 (90.0)26.2 (11.93)Gamma nail (n = 10)–10Primary cementless (n = 8)Diaphyseal revision cementless (n = 2)N/AGodoy-Monzon (2020)Retrospective Case Series2872.7 (10.5)17 (60.7)63.6 (60–84)Cephalomedullary nail (n = 28)Posterolateral28Diaphyseal revision cementless (n = 23)Diaphyseal revision cemented (n = 5)MP Reconstruction Prosthesis (modular taper-fluted stem)(n = 28)Huang (2022)Retrospective Cohort244Uncemented THA: 68 (63–76)Cemented THA: 68 (64–77)Uncemented THA: 60 (48.4)Cemented THA: 57 (47.5)60 (50–67)Proximal femoral nail antirotation (n = 244)Lateral244Primary cementless (n = 124)Primary cemented (n = 120)Taperloc stem (proximal metaphyseal-fitting, wedge-shaped, porous-coated cementless stem) (n = 124)Exeter Universal stem (polished, tapered cemented stem) (n = 120)Liu (2014)Retrospective Case Series973.4 (63–82)6 (85.7)18 (12–24)Proximal femoral nail antirotation (n = 7)–7––Mathur (2022)Prospective Case Series1562.8 (9.1)7 (46.7)16.9 (7.9)Proximal femoral nail antirotation (n = 15)Posterolateral15Diaphyseal revision cementless (n = 15)DePuy Solution System (extensively porous coated distally loading revision stem) (n = 15)Min (2019)Prospective Cohort8364.6 (19–87)33 (39.8)42 (15.6–108)Cephalomedullary nail (n = 19)Anterolateral19Primary cementless (n = 19)Zimmer CLS stem (n = 19)Pui (2013)Retrospective Multicenter Cohort3165.1 (20.5)19 (61.3)35Cephalomedullary nail (n = 31)Posterolateral, Anterolateral31Primary cementless (n = 24)Primary cemented (n = 7)N/ASchultz (2022)Retrospective Cohort2277.09 (8.83)17 (77.3)36.6 (28.4)Cephalomedullary nail (n = 22)Posterolateral, Anterolateral22Diaphyseal revision cementless (n = 17)Diaphyseal revision cemented (n = 5)N/ASmith (2019)Retrospective Cohort36979.93 (5.86)276 (74.8)24Cephalomedullary nail (n = 369)–369––Solarino (2013)Retrospective Cohort7473.8 (7.85)45 (60.8)24Cephalomedullary nail (n = 74)Anterolateral74Diaphyseal revision cementless (n = 39)Primary cemented (n = 19)Primary cementless (n = 16)N/ASoundarrajan (2024)Retrospective Cohort3961.5 (16.1)20 (51.3)27.5 (12–72)Cephalomedullary nail (n = 16)Anterolateral16Primary cementless (n = 16)Zimmer Wagner SL stem (monoblock, tapered, distal-loading, grit-blasted titanium stem) (n = 16)Yu (2020)Retrospective Cohort198Uncemented THA: 66.84 (4.72)Cemented THA: 66.73 (5.12)Uncemented THA: 53 (54.1)Cemented THA: 52 (52.0)65 (60–69)Proximal femoral nail antirotation (n = 198)–198Primary cementless (n = 98)Primary cemented (n = 100)Corail stem (proximal metaphyseal-fitting stem) (n = 98)Exeter Universal stem (polished, tapered cemented stem) (n = 100)Yu (2016)Retrospective Cohort7070.07 (11.76)33 (47.1)31.67 (5.24)Proximal femoral nail antirotation (n = 70)Posterolateral, Anterolateral70Primary cementless (n = 36)Primary cemented (n = 34)N/AZeng (2017)Retrospective Cohort7276.93 (9.25)41 (56.9)47.92 (4.31)Proximal femoral nail antirotation (n = 72)Posterolateral72Primary cementless (n = 42)Primary cemented (n = 30)N/AZhong (2021)Retrospective Cohort1867.3 (38–92)8 (80.0)24.7 (12–36)Intramedullary nail (n = 6)Posterolateral6––cTHA conversion total hip arthroplasty, SD standard deviation
Table 3. Intraoperative details and postoperative outcomesAuthor (year)Number of cTHAsMean operative time, minutes (SD)Mean LOS, days (SD)Mean EBL, mL (SD)Need for Transfusion, n (%)Number of Transfused UnitsRevision, n (%)Infection, n (%)Dislocation, n (%)Subsidence, n (%)PPF,n (%)Other complications, nBrunner (2016)27–––0 (0.0)–1 (3.7)0 (0.0)1 (3.7)0 (0.0)0 (0.0)–Cardenas (2024)45–3.77 (2.58)576.83 (366.59)0 (0.0)–6 (13.3)4 (8.9)1 (2.2)0 (0.0)2 (4.4)Falls (n = 2)Acute renal failure (n = 1)Heterotopic ossification (n = 1)IT band syndrome (n = 1)Myocardial infarction (n = 1)Potential metal allergy (n = 1)Gazzotti (2014)10–––7 (70.0)2, 3, or 4 units1 (10.0)0 (0.0)2 (20.0)0 (0.0)0 (0.0)Persistent thigh pain (n = 3)Ipometria > 2 cm (n = 1)Godoy-Monzon (2020)28–––––0 (0.0)1 (3.6)2 (7.2)0 (0.0)0 (0.0)Sympotomatic abductor deficiency (n = 1)Huang (2022)244–––––11 (4.5)7 (2.9)4 (1.6)11 (4.5)10 (4.1)Insufferable hip pain (n = 7)Lower limb shortening (n = 6)Thrombotic events (n = 2)Liu (2014)7–––0 (0.0)–0 (0.0)0 (0.0)0 (0.0)0 (0.0)0 (0.0)–Mathur (2022)15––461.3 (22.3)15 (100.0%)1 unit (n = 12), 2 units (n = 3)0 (0.0)1 (6.7)1 (6.7)0 (0.0)0 (0.0)Intraoperative hypotension (n = 1)Min (2019)19–––––3 (15.8)0 (0.0)1 (5.3)0 (0.0)1 (5.3)–Pui (2013)31–––––0 (0.0)1 (3.2)2 (6.4)1 (3.2)3 (9.7)Urinary tract infection (n = 1)Pulmonary embolism (n = 1)GI bleed (n = 1)Acute renal failure (n = 1)Abductor tendon deficiency (n = 1)Heterotopic ossification (n = 2)Intraoperative nerve injury (n = 1)Schultz (2022)22176.3 (54.7)5.5 (2.9)600 (240)––3 (13.6)2 (9.1)2 (9.1)0 (0.0)0 (0.0)Sepsis (n = 10)Acute kidney injury (n = 1)Urinary tract infection (n = 1)Anemia (n = 7)Smith (2019)369–5.3 (3.5)–––24 (6.5)3 (0.8)9 (2.4)0 (0.0)0 (0.0)Care involving other specified rehabilitation procedure leading to revision (n = 3)Urinary tract infection (n = 3)Other mechanical complication of orthopaedic device, implant or graft (n = 2)Myasthenia gravis (n = 1)Atrial flutter (n = 1)SA node dysfunction (n = 1)Acute venous thromboembolism (n = 1)Bacterial pneumonia (n = 1)Solarino (2013)74117 (76–192)–585 (430–1720)43 (58.1%)3 or more units4 (5.4)3 (4.0)5 (6.8)0 (0.0)8 (10.8)Death due to pulmonary embolism (n = 2)Ischemic myocardial infarction (n = 1)Soundarrajan (2024)16–––––2 (12.5)0 (0.0)0 (0.0)0 (0.0)2 (12.5)–Yu (2020)198–––––14 (7.1)0 (0.0)6 (3.0)18 (9.1)13 (6.6)Unbearable hip pain (n = 7)Yu (2016)70–––––0 (0.0)2 (2.9)4 (5.7)0 (0.0)5 (7.1)Urinary tract infection (n = 2)Pulmonary embolism (n = 2)Atrial fibrillation (n = 2)Acute renal failure (n = 1)Abductor tendon deficiency (n = 2)Heterotopic ossification (n = 4)Intraoperative nerve injury (n = 1)Zeng (2017)72–––––0 (0.0)2 (2.8)1 (1.4)0 (0.0)3 (4.2)Urinary tract infection (n = 1)Atrial fibrillation (n = 2)Prosthetic instability (n = 1)Limb length discrepancy (n = 1)Abductor tendon deficiency (n = 2)Heterotopic ossification (n = 1)Intraoperative nerve injury (n = 1)Zhong (2021)6––327.5 (81.7)––0 (0.0)0 (0.0)1 (16.7)0 (0.0)0 (0.0)–cTHA conversion total hip arthroplasty, EBL estimated blood loss, LOS length of stay, PPF periprosthetic fracture, SD standard deviation
Overall revision rate was 6.7% (5.3–8.3%) (Fig. 2), infection rate was 3.3% (2.1–5.2%) (Fig. 3), dislocation rate was 4.5% (3.1–6.5%) (Fig. 4), and PPF rate was 5.9% (4.4–7.8%) (Fig. 5). Subsidence was reported in only three studies at rates of 4.5%, 3.2%, and 9.1% [18, 22, 27]. Additional complications associated with cTHA were diverse, including frequent occurrences of urinary tract infections, heterotopic ossification, and abductor tendon deficiencies. Cardiovascular complications such as pulmonary embolism and atrial fibrillation, along with persistent pain issues like severe hip or thigh discomfort, were also documented.
Fig. 2. Forest plot of revision rate following cTHA
Fig. 3. Forest plot of infection rate following cTHA
Fig. 4. Forest plot of dislocation rate following cTHA
Fig. 5. Forest plot of periprosthetic fracture rate following cTHA
An exploratory analysis was performed by implant type. There were six studies that stratified outcomes based on implant type: primary cementless (n = 265), primary cemented (n = 220), and diaphyseal cementless (n = 17) stems (Supplemental Table 3) [16, 18, 20, 21, 26, 27]. The overall pooled revision rate was 10.1% (7.0-14.5%) for cementless implants, 2.4% [1.0–5.6%] for cemented implants, and 7.0% (0.9–37.2%) for diaphyseal cementless implants. Infection rates were 2.8% (1.3–6.1%) for cementless, 1.8% (0.5–6.2%) for cemented, and 8.9% (1.8–34.7%) for diaphyseal cementless implants, while dislocation rates were 3.3% (1.6–6.6%), 2.4% (1.0-5.6%), and 18.3% (1.7–74.4%), respectively. Subsidence occurred in 8.1% (4.3–15.0%) of cementless implants, 3.8% (1.9–7.5%) of cemented implants, and 7.0% (0.9–37.2%) of diaphyseal cementless implants, while PPF was reported in 7.7% (4.7–12.5%), 3.2% (1.5–6.5%), and 7.0% (0.9–37.2%), respectively. However, it is important to note that stem choice may have been highly confounded by baseline patient factors and bone quality.
Discussion
The management of failed IT fracture fixation remains a significant challenge despite advancements in fixation techniques. Existing literature on outcomes following cTHA for failed IT fracture fixation is limited. This systematic review and meta-analysis found a pooled revision rate of 6.7% after cTHA for failed cephalomedullary nailing of IT fractures. Additionally, we characterized rates of infection (3.3%), dislocation (4.5%), and PPF (5.9%). Subgroup analysis of femoral component type identified variation in revision and complication rates among primary cemented, primary cementless, and diaphyseal cementless implants.
Compared to primary THA, current evidence has largely supported that cTHA carries a higher complication burden [7, 30–33]. Our study found a revision rate of 6.7% following cTHA for failed cephalomedullary nailing of IT fractures, aligning with prior research. In a national database study, the authors matched primary THA and cTHA patients based on age, gender, and other comorbidities and reported a 4.0% revision rate at 90 days and 10.1% at one year for cTHA, which was notably elevated compared to 1.5% and 2.8% for primary THA, respectively [30]. Similarly, in a single-center prospective database study composed of 163 matched primary and cTHA patients, revision surgery was more prevalent in the cTHA cohort (11.7%) than the primary THA cohort (4.9%) [7]. Schwarzkopf et al. identified and matched 119 cTHAs and 251 primary THAs and determined that patients undergoing cTHA had a greater likelihood of requiring diaphyseal fixation and revision type implant components in addition to having a longer hospital length of stay and longer operative time [31]. Ryan et al. also found that intraoperative complications in cTHA were four times higher than those seen in primary THA, with conversion cases requiring significantly more blood transfusions and experiencing a greater incidence of fractures [7]. Other studies have confirmed this trend of increased intraoperative and short-term postoperative medical complications in cTHA compared to primary THA [32, 33]. These findings, in conjunction with our results, emphasize that while cTHA is an important salvage option for failed IT fracture fixation, it is a higher risk procedure than primary THA.
Moreover, in our study, rates of infection (3.3%), dislocation (4.5%), and periprosthetic fractures (5.9%) following cTHA similarly surpassed the rates typically reported for primary THA. Douglas et al. noted that cTHA is associated with higher rates of periprosthetic joint infection (7.7% vs. 1.4% at 90 days; 11.2% vs. 2.3% at 1 year; 12.2% vs. 2.4% at 2 years), dislocations (4.5% vs. 2.0% at 90 days), and mechanical complications (5.5% vs. 1.0% at 90 days) compared to primary THA [34]. In a different study, dislocation rates in cTHA (8.0%) were greater than primary THA (2.5%), although PPF rates were similar (3.1% vs. 3.7%) [26]. Other comparisons between cTHA and primary THA have indicated that cTHA is consistently associated with an elevated rate of postoperative surgical site infections [24]. Such evidence reinforces our results and the observed trend that conversion procedures inherently entail greater surgical complexity and postoperative risk.
In this study, due to limited reporting detail, no formal between-group statistical comparisons could be performed based on implant type, even though implant-specific descriptive pooled estimates are presented. Nevertheless, there is a lack of agreement in existing literature on the optimal conversion method after failed IT fracture fixation. A recent meta-analysis by Dix et al. compared various conversion methods (e.g., cemented, uncemented, and hemiarthroplasty) after failed IT fracture fixation and found no substantial difference in complication rates across methods, suggesting that outcomes may be more dependent on underlying patient factors and the technical challenges inherent to conversion procedures [33]. Similarly, Luthringer et al. reported that while cTHA might offer slightly better functional outcomes compared to hemiarthroplasty, complication rates remained comparable [35]. However, specific studies have highlighted that implant type may influence outcomes, suggesting that factors beyond the arthroplasty type, such as fixation method and implant model, may play a pivotal role in determining complication rates and functional outcomes [28, 36]. For instance, Zeng et al. reported variable outcomes based on femoral stem selection in cTHA after IT fracture failure [28]. The authors highlighted that cemented stems generally had fewer revisions, while cementless and diaphyseal stems were associated with increased risks of subsidence and instability. Conversely, Thalody et al. did not find substantial differences in outcomes between primary cementless metaphyseal-engaging femoral stems and revision diaphyseal-engaging stems used in cTHA [36]. Many of these studies are likely limited by their sample size and long-term follow-up, limiting conclusions about the true effect size of femoral component type on patient outcomes.
Beyond differences in implant selection, several mechanical and anatomical factors intrinsic to conversion total hip arthroplasty may contribute to the elevated complication rates observed in this population. Prior fracture fixation and surgical exposure can compromise the abductor mechanism, increasing the risk of postoperative instability and dislocation. Additionally, altered proximal femoral anatomy, residual bone defects following implant removal, and stress risers from prior screw or nail tracks may predispose patients to periprosthetic fracture and stem subsidence. Technical challenges associated with removal of well-fixed cephalomedullary nails, including cortical damage during extraction, may further exacerbate bone loss and complicate femoral reconstruction. These factors likely interact with patient-specific characteristics such as bone quality and fracture pattern, the importance of selecting femoral components based on patient-specific anatomical and clinical factors to mitigate complication risks and improve outcomes.
There are several limitations that should be acknowledged. First, our analysis was limited to studies retrieved from two databases (PubMed and Embase). The included studies were largely of Level III and IV evidence, which inherently limits the reliability of our conclusions and introduces potential bias. Our attempt to compare complication rates by implant type was constrained by the limited number of studies providing granular stratified data, thereby limiting any conclusions from our findings on implant-related outcomes. Additionally, our analysis may be subject to selection bias, as patients who underwent cTHA with cemented stems were likely older, frailer, and had poorer bone quality, which may have influenced implant selection and the likelihood of being included in studies reporting revision outcomes. As such, cemented stems may have been preferentially used in patients with lower functional demands or higher medical risk, potentially skewing complication rates.
This study also focused on cTHA revision and complication rates without incorporating functional outcome measures such as the Harris Hip Score, which limits our ability to evaluate patient-centered functional results comprehensively. Such outcomes were also not reliably reported in the included studies. Moreover, there were inconsistencies in follow-up durations across studies, which may impact the reported complication rates; outcomes like revision, infection, or dislocation are influenced by the length of follow-up, and varying durations make direct comparisons challenging. This approach was necessary due to inconsistent reporting across studies and is acknowledged as a methodological limitation. In cases when THA-specific demographic data were unavailable, our use of cohort-level demographic data may have introduced misclassification bias. Although we used statistical methods to minimize bias in the meta-analysis, the innate variability in study design, patient demographics, and reporting practices introduces an element of heterogeneity that cannot be fully controlled. Future research with higher-level evidence, larger sample sizes, standardized outcome measures, and extended follow-up periods is necessary to address these gaps and provide more definitive guidance on cTHA after cephalomedullary nailing of IT fractures.
Conclusion
cTHA is a viable option for failed cephalomedullary nail fixation of IT fracture, with a revision rate of 6.7%, and infection, dislocation, and PPF rates of 3.3%, 4.5%, and 5.9%. Cemented femoral components demonstrated the lowest revision (2.4%), infection (1.8%), dislocation (2.4%), subsidence (3.8%), and PPF (3.2%) rates compared to cementless and diaphyseal cementless stems, which carry different respective complication profiles. Although implant-specific trends were observed, the limited data preclude firm conclusions. Future studies with larger, stratified cohorts are needed to better evaluate the effect of femoral component type on outcomes. Ultimately, implant decisions should be tailored to the individual patient, weighing patient risk factors and functional demands.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tate JP, Reinhart NM, Bridges CA, Brown NM, Sherman WF (2025) Comparative outcomes of early versus late conversion to total hip arthroplasty following hip fracture fixation. J Arthroplasty Published Online January 21. 10.1016/j.arth.2025.01.01510.1016/j.arth.2025.01.01539848449 · doi ↗ · pubmed ↗
- 2Grayson W, Eikani C, Benson M, Jozefowski N, Brown NM (2024) High rate of complications with early conversion hip arthroplasty following fracture treatment. J Am Acad Orthop Surg Glob Res Rev 8(11) e 24.00318. Published 2024 Nov 19. 10.5435/JAAOS Global-D-24-0031810.5435/JAAOS Global-D-24-00318 PMC 1157820639792608 · doi ↗ · pubmed ↗
- 3Smith A, Denehy K, Ong KL, Lau E, Hagan D, Malkani A (2019) Total hip arthroplasty following failed intertrochanteric hip fracture fixation treated with a cephalomedullary nail. Bone Joint J 91–96. 10.1302/0301-620X.101B 6.BJJ-2018-1375.R 1. 101-B(6_Supple_B 10.1302/0301-620X.101B 6.BJJ-2018-1375.R 131146562 · doi ↗ · pubmed ↗