Functional Dyspepsia Among Nurses Working Rotating Shifts: Its Prevalence and Associations With Sleep Quality and Stress
Rishit Gupta, Arihant Senthil, Smita Nath, Rajnish K Avasthi, Shrey Chopra, Sukul Khanna

TL;DR
This study finds that 31% of nurses working rotating shifts in India suffer from functional dyspepsia, a digestive disorder linked to poor sleep and high stress.
Contribution
The study is the first to report FD prevalence among Indian nurses and its strong association with sleep and stress in this population.
Findings
31% of nurses working rotating shifts had functional dyspepsia, higher than the general Indian population.
FD was strongly correlated with poor sleep quality (74.2% vs. 43.5%) and high stress levels (83.8% vs. 34.7%).
No gender differences were found in FD prevalence among the studied nurses.
Abstract
Background and objective Functional dyspepsia (FD) is one of the most common functional gastrointestinal disorders that frequently impairs quality of life. Among healthcare professionals, shift work may heighten the risk of developing this condition, likely through its impact on stress levels and sleep quality. This study aimed to determine the prevalence of FD among nurses working rotating shifts in India and to examine its relationship with sleep quality and perceived stress. Methods A cross-sectional study was conducted at a tertiary care hospital in New Delhi (January 2022-March 2023). The participating nurses (n=100) completed standardized questionnaires, including the Rome IV criteria for FD diagnosis, Pittsburgh Sleep Quality Index (PSQI), and Perceived Stress Scale-10 (PSS-10). Statistical analyses included chi-square tests to evaluate associations. Results The prevalence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
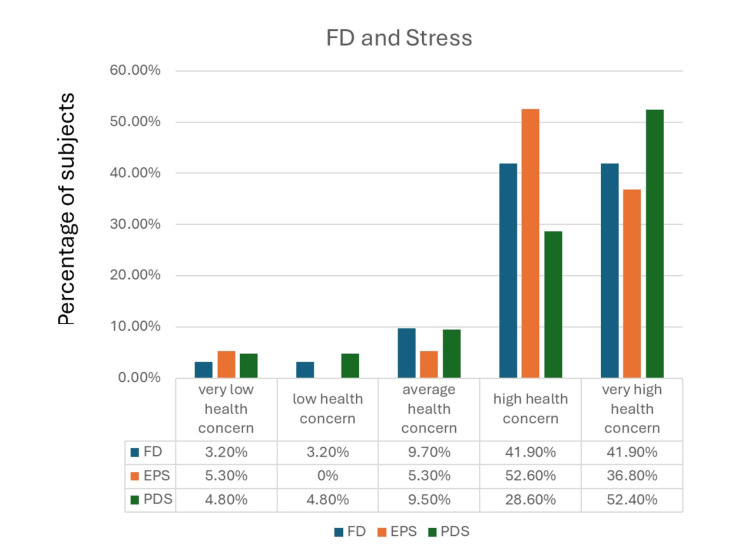 Figure 1
Figure 1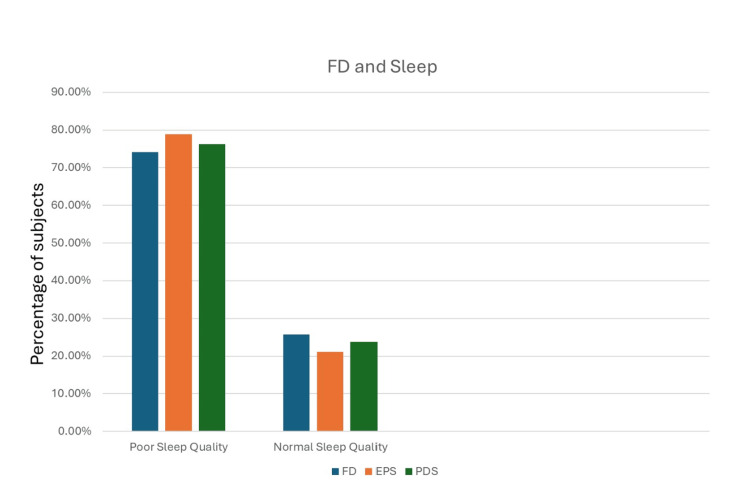 Figure 2
Figure 2| Demographic | FD | No FD |
| Age ≤35 years (n=51) | 13 (25.5%) | 38 (74.5%) |
| Age >35 years (n=49) | 18 (36.7%) | 31 (63.3%) |
| Female (83) | 26 (31.3%) | 57 (68.7%) |
| Male (17) | 5 (29.4%) | 12 (70.6%) |
| Group | Poor sleep quality (%) | P-value | High/very high stress (%) | P-value |
| FD (n=31) | 74.2 | 0.003 | 83.8 | 0.000 |
| PDS (n=21) | 76.2 | 0.01 | 81.0 | 0.000 |
| EPS (n=19) | 78.9 | 0.008 | 89.4 | 0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal motility and disorders · Sleep and Work-Related Fatigue · Sleep and related disorders
Introduction
Dyspepsia is an umbrella term for chronic or recurrent upper abdominal symptoms such as pain, discomfort, postprandial fullness, or early satiety. Studies have shown that about 80% of individuals with dyspepsia show no abnormalities on diagnostic evaluations, including upper gastrointestinal (GI) endoscopy. Most patients with symptoms of dyspepsia can, therefore, be assumed to have functional dyspepsia (FD), i.e., dyspepsia without any apparent organic cause [1,2,3]. Cross-sectional surveys applying symptom-based criteria for assigning a diagnosis of dyspepsia without an endoscopy thus offer a close approximation of FD prevalence [2].
The exact pathogenesis of FD remains uncertain. Multiple complex pathophysiological mechanisms have been proposed, many of which may overlap and contribute to the development and progression of the disorder: altered GI motility and sensory dysfunction, immune-mediated GI inflammation, changes in the gut microbiome, and improper gut-brain signaling. Evidence also suggests that among a majority of healthcare seekers, psychiatric conditions like anxiety and depression precede various functional GI disorders (FGIDs), including FD, thereby lending credence to a possible contributory psychopathological mechanism [4].
FD is a fairly common condition, with prevalence rates ranging from 5 to 40% in various studies. This broad range likely reflects geographical differences and inconsistencies in the diagnostic criteria used to define FD. The prevalence of FD based on the Rome diagnostic criteria is typically 6-14% higher in Western countries compared to Eastern countries [5]. Shah et al. in their study found that the prevalence of dyspepsia in urban India can be as high as 30.4% [6]. In industrialized countries, as much as 75% of the workforce is estimated to engage in shift or night work [7].
Shift work is linked to a higher risk of obesity, diabetes, cardiovascular disease, malignancies, and immune system disorders [8]. Additionally, irregular shift work is strongly associated with increased GI disturbances or FGIDs [9]. Due to the continuous demands associated with human health and disease management, healthcare facilities must operate 24/7, making shift work an essential component of the healthcare system. A study in South Korea reported that nurses working rotating shifts had a 19.7% prevalence of FD [10]. The primary aim of our study is to determine the prevalence of FD in nurses working in rotating shifts.
Two significant impacts of shift work are a disturbed sleep cycle and a higher level of emotional stress. The irregular sleep cycle of shift workers has been associated with disturbances in the rhythmic secretion of melatonin and cortisol [11]. In a study by Klupińska et al., regular intake of melatonin was found to be associated with significant symptom reduction in patients with FD [12]. This suggests that disruption in the normal circadian rhythm, a primary component of which is melatonin secretion, could be a significant contributor to the development of FD. Moreover, emotional stress has been linked to FD development in younger patients [13]. The secondary objective of this study is to appraise the relationship between sleep quality and emotional stress with the development of FD.
Materials and methods
Study design and setting
This was a cross-sectional hospital-based study that was conducted between January 2022 and March 2023 at the University College of Medical Sciences and GTB Hospital, New Delhi, which is a tertiary care hospital.
Study population and eligibility criteria
Hospital nurses were invited to complete standardized, self-administered questionnaires following a detailed explanation of the process and after obtaining written informed consent. Participation was completely voluntary and uncompensated. Out of the 124 nurses who initially volunteered, 24 were excluded based on the inclusion and exclusion criteria.
Inclusion Criteria
The inclusion criteria were as follows: (1) nurses aged 18-60 years who gave consent, and (2) participants with at least one year of service in the healthcare system.
Exclusion Criteria
The exclusion criteria were as follows: (1) lactating or pregnant women; (2) individuals with a history of inflammatory bowel disease; (3) those who had undergone previous gastrointestinal surgery; and (4) participants with a prior diagnosis of cancer, acid peptic disease, or any history of smoking or alcohol consumption.
Survey questionnaires
Four distinct sets of questionnaires, comprising a total of 44 questions, were employed in this study. First, a general pro forma was used to collect demographic data and ensure adherence to the inclusion and exclusion criteria. Next, the diagnosis of FD was based on the Rome IV criteria and was assessed using the Rome IV questionnaire [14]. Sleep quality was evaluated using the Pittsburgh Sleep Quality Index (PSQI), a validated instrument for assessing sleep in adults. The PSQI differentiates between “good” and “poor” sleep quality by analyzing seven domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medications, and daytime dysfunction over the preceding month. A total score of 5 or higher signifies poor sleep quality [15]. In addition, the Perceived Stress Scale-10 (PSS-10) was administered to provide an initial assessment of stress levels. The Perceived Stress Scale-10 (PSS-10) offers a validated framework for categorizing stress into five distinct groups. The 10-item questionnaire assigns scores of 0-7 to "very low health concern," 8-11 to "low health concern," 12-15 to "average health concern," 16-20 to "high health concern," and 21 or above to "very high health concern" [16]. This detailed stratification allows for a good understanding of the severity of stress in the study population.
Statistical analysis
The data collected from the above-mentioned questionnaires were entered into an MS Excel sheet and then transferred to SPSS Statistics software 20.0 (IBM Corp., Armonk, NY). Scoring and categorization were done as mentioned in the questionnaire. Descriptive tables were generated, and the chi-square test was applied to find associations, if any, between different parameters. The statistical significance level was set at 5%.
Ethical considerations
The study was conducted after obtaining approval from the Institutional Ethics Committee-Human Research (IECHR), in accordance with the Declaration of Helsinki at the University College of Medical Sciences and GTB Hospital.
Informed consent
Hospital nurses were asked to fill out standardized, self-reported questionnaires after receiving a thorough explanation of the study and providing written informed consent. Their involvement was completely voluntary, and no incentives were offered.
Results
Our study was conducted among nurses engaged in rotating shift work at GTB Hospital and involved a total of 100 participants. The participants were comprised of 83% females (n=83) and 17% males (n=17).
Prevalence of FD and its subtypes
Based on their responses, 31% (n=31) of patients had FD, and 69% (n=69) did not. The Rome IV questionnaire classifies FD into two subcategories, postprandial distress syndrome (PDS) and epigastric pain syndrome (EPS). Among all patients, 12% (n=12) had PDS only, 10% (n=10) had EPS only, and 9% (n=9) had both PDS and EPS. Accordingly, when including overlapping cases, 21% of participants (n=21) had PDS (either alone or with concurrent EPS), and 19% (n=19) had EPS (either alone or with concurrent PDS). These percentages are not mutually exclusive, as patients who meet the criteria for both subtypes are counted in both groups.
Assessment of sleep quality and stress amongst participants
Based on the results of the PSQI questionnaire, 53% (n=53) of the patients had poor sleep quality, while 47% (n=47) did not. Perceived stress was measured using the PSS-10 questionnaire: 24% (n=24) of the patients were categorized under ‘very high health concern’, 26% (n=26) under ‘high health concern’, 27% (n=27) under ‘average health concern’, 16% (n=16) under ‘low health concern’, and 7% (n=7) under ‘very low health concern’.
Correlation of biological sex with various parameters
Table 1 shows the distribution of FD by age group and sex among our participants.
Of note, 83% of the participants (n=83) were female, and 17% (n=17) were male in our study. No statistically significant correlation was found between biological sex and any of the measured parameters. Out of the 31 patients who had FD, 26 were female (p=0.225). Twenty-one patients had PDS, and 18 of these were female (p=0.389). 19 patients had EPS, and 15 of these were female (p=0.490). Among females, about half (50.6%) had poor sleep quality, and among males, a majority (64.7%) had poor sleep quality. Based on responses to the PSS-10 questionnaire, perceived stress represented a high or very high health concern for 53% of female participants and 35.2% of male participants.
Correlation of perceived stress with FD
The presence of FD was strongly associated with higher perceived stress. Figure 1 illustrates the relationship of FD and its subtypes with stress.
Association between FD and stressFD: functional dyspepsia; EPS: epigastric pain syndrome; PDS: postprandial distress syndrome
Overall, 83.8% of patients with FD fell into the high or very high stress category (p=0.000), compared with only 34.7% of those without FD. A similar pattern was observed in both subtypes. Among patients with PDS, 81% reported high or very high stress (p=0.000), versus 41.8% of PDS-negative individuals. Likewise, 89.4% of patients with EPS were categorized as having high or very high stress according to PSS-10 (p=0.001), compared with 40.8% of those without EPS.
Correlation of sleep quality with FD
FD was also significantly correlated with poor sleep quality. Figure 2 demonstrates the relationship of FD and its subtypes with sleep quality.
Association between FD and sleep qualityFD: functional dyspepsia; EPS: epigastric pain syndrome; PDS: postprandial distress syndrome
Among individuals with FD, 74.2% reported poor sleep quality (PSQI score ≥5; p=0.003), compared with 43.5% of those without FD.
Comparable findings emerged when FD was stratified by subtypes. Poor sleep was present in 76.2% of patients with PDS (p=0.001) compared with 46.8% of those without PDS. Similarly, 78.9% of EPS-positive patients had poor sleep quality (p=0.008), versus 46.9% of EPS-negative individuals. Table 2 summarizes these findings.
Discussion
To our knowledge, this is the first study to use the Rome IV criteria for calculating the prevalence of FD in the Indian context. Rome IV divides FD into two subcategories, PDS and EPS. Patients may be assigned one or both of these diagnoses based on which symptoms predominate in their responses. In this cross-sectional questionnaire-based study, we found a 31% prevalence of FD among our subjects, all of whom were nurses working in rotating shifts; 12% of respondents had only PDS, 10% had only EPS, and 9% had both. In comparison, Shah et al. [6] reported a dyspepsia prevalence of 30.4% in the general urban Indian population, indicating that the prevalence of FD in our study group is comparatively higher. Similar studies conducted in South Korea reported the prevalence of FD among nurses working rotating shifts to be 19.7% [10] and 22.2% [17], respectively. Nagarethinam et al. reported that 19% of healthcare professionals in a tertiary care center in Australia were diagnosed with FD [18]. Several studies have also shown that non-day shift workers experience more GI symptoms than those on regular day shifts [9,19,20], with comparable patterns observed for functional bowel disorders [21] and IBS [22]. This suggests a possible link between shift work and FD.
According to our study, neither biological sex significantly correlated with FD incidence. Various studies have found that females are at a relatively higher risk of developing FD [2,23]. However, our study found no correlation between biological sex and the risk of developing FD.
Correlation of FD with sleep quality
Shift work is known to cause disturbances in the sleep cycle as well as reduced quality of sleep, and various studies have shown these to be significant contributors to the development of GI disturbances. In a study by Torsvall et al., the average duration of sleep following a night shift was reduced by more than two hours compared with sleep after an afternoon shift. This reduction predominantly affected REM (rapid eye movement) and Stage 2 NREM (non-rapid eye movement) sleep, both of which play important roles in long-term memory consolidation [24]. Additionally, 28% of night-shift patients also reported adding a spontaneous afternoon nap to their main sleep after their night shift [25]. These findings suggest that shift work causes significant alterations in sleep quality, duration, and pattern.
Roehrs et al. showed that modest reductions in sleep, and, specifically, REM sleep deprivation, had a somatic hyperalgesic effect. Their findings also indicated that the effects of sleep loss accumulated over multiple nights of sleep deprivation and further contributed to hyperalgesia [26]. Possible pathophysiological mechanisms that might explain this finding include decreased cholinergic activity, a finding observed in rats deprived of REM sleep [27], and depletion of serotonin and its metabolite (5-HIAA) [28,29]. An important concept in sleep physiology is that of the circadian rhythm, colloquially referred to as the 24-hour biological clock. Reduced night sleep time and compensatory daytime sleep are associated with disturbances in hormonal secretions, an important component of the circadian rhythm [11].
In addition, the circadian rhythm has been shown to affect gut visceral sensitivity [30]. This is further evidenced by the findings of Nojkov et al., who interestingly concluded that increased IBS prevalence in rotating shift workers was a consequence of circadian rhythm disruption, rather than poor sleep quality [22]. In our study, poor sleep quality was significantly associated with a higher risk of FD. Out of all the participants who had FD, about three-quarters had poor sleep. This is consistent with a study done in South Korea, which also shows a significant correlation between poor sleep quality and FD [17]. We believe that both poor sleep quality as well as a disturbed circadian rhythm in nurses working in rotating shifts might contribute to the increased prevalence of FD in this population.
Correlation of FD with perceived stress
Shift work has been associated with higher stress levels, and higher perceived stress has, in turn, been linked to an increased risk of GI morbidity. Night shift work has been associated with increased occupational stress among nurses [31]. Furthermore, among nurses, psychosocial problems are more common amongst those working rotating shifts than those working during the day [32]. The gut-brain axis is an emerging concept that outlines bidirectional communication between cognitive and emotional centers of the brain and the enteric nervous system. The central nervous system has a definite role in peripheral intestinal functioning and may play a role in various GI pathologies [33]. Improper gut-brain signaling has been implicated in the development of various FGIDs. This might, in part, explain a possible psychopathological mechanism behind FGID development.
According to our findings, a substantial majority of patients with FD (83.8%) exhibited stress levels indicative of significant health concern. In contrast, only 43.5% of patients without FD demonstrated comparable stress levels. These findings align with other studies that have analyzed the correlation between GI problems and psychological factors. Higher perceived levels of stress have been associated with an increased incidence of GI symptoms in healthcare professionals [18]. Koh et al. concluded that significant psychosocial distress is an independent risk factor for the development of FD [10]. According to a population-based survey conducted in Sweden, participants with anxiety had higher odds of developing FD compared to those without FD [34].
Our findings suggest that perceived stress and poor sleep quality are strongly associated with the presence of functional dyspepsia among nurses engaged in rotating shift work. While these associations are statistically significant and consistent with prior literature, the cross-sectional nature of our study precludes causal inference. It is therefore more appropriate to interpret these results as correlational rather than causal. Future longitudinal or interventional studies with larger sample sizes and multivariate analyses are warranted to clarify the independent contributions of stress, sleep, and other occupational factors to FD risk.
Limitations
This study has several limitations. Being single-center and cross-sectional, its findings may not be generalizable and cannot establish causality. The absence of a control group and the potential influence of unmeasured confounders limit internal validity. Diagnostic accuracy may also have been affected by the lack of endoscopic confirmation, as FD was defined solely by Rome IV symptom criteria. In addition, the modest response rate raises the possibility of selection bias, as nurses experiencing symptoms may have been more likely to participate. Finally, external stressors related to variable work schedules could not be fully accounted for, which may have influenced the observed associations.
Conclusions
This study found a 31% prevalence of FD among nurses working rotating shifts, which is higher than rates reported in many international cohorts and slightly exceeds estimates for the general Indian population. Poor sleep quality was significantly associated with FD, with the majority of affected nurses reporting suboptimal sleep, suggesting that circadian rhythm disruption may play a key role in symptom development. Additionally, perceived stress was notably greater in nurses with FD compared to those without, supporting the involvement of stress-related mechanisms in FD pathophysiology. These findings highlight the occupational health risks faced by nurses engaged in shift work, underscoring the need for institutional policies and workplace interventions that promote sleep hygiene, stress management, and mental health support. Identifying at-risk individuals through screening and providing targeted interventions may help alleviate the burden of FD and enhance the well-being and productivity of healthcare professionals. Future longitudinal studies involving larger and more diverse populations, the inclusion of control groups, and the use of objective diagnostic methods such as endoscopy are needed to clarify causal relationships and improve preventive strategies. Ultimately, addressing modifiable factors such as sleep and stress in this vulnerable workforce could contribute not only to better GI health but also to enhanced quality of life and occupational performance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Functional dyspepsia: current understanding and future perspective Digestion Oshima T 263310520243759867310.1159/000532082 · doi ↗ · pubmed ↗
- 2Functional dyspepsia Lancet Ford AC Mahadeva S Carbone MF Lacy BE Talley NJ 1689170239620203304922210.1016/S 0140-6736(20)30469-4 · doi ↗ · pubmed ↗
- 3What is the prevalence of clinically significant endoscopic findings in subjects with dyspepsia? Systematic review and meta-analysis Clin Gastroenterol Hepatol Ford AC Marwaha A Lim A Moayyedi P 830832830-7, 837.e 1-2820102054162510.1016/j.cgh.2010.05.031 · doi ↗ · pubmed ↗
- 4Mood and anxiety disorders precede development of functional gastrointestinal disorders in patients but not in the population Clin Gastroenterol Hepatol Jones MP Tack J Van Oudenhove L Walker MM Holtmann G Koloski NA Talley NJ 101410201520172808740410.1016/j.cgh.2016.12.032 · doi ↗ · pubmed ↗
- 5Clinical and epidemiological differences in functional dyspepsia between the East and the West Neurogastroenterol Motil Mahadeva S Ford AC 1671742820162633191910.1111/nmo.12657 · doi ↗ · pubmed ↗
- 6Epidemiology of dyspepsia in the general population in Mumbai Indian J Gastroenterol Shah SS Bhatia SJ Mistry FP 103106202001 https://pubmed.ncbi.nlm.nih.gov/11400800/11400800 · pubmed ↗
- 7Association between light at night, melatonin secretion, sleep deprivation, and the internal clock: health impacts and mechanisms of circadian disruption Life Sci Touitou Y Reinberg A Touitou D 9410617320172821459410.1016/j.lfs.2017.02.008 · doi ↗ · pubmed ↗
- 8Shift work and body composition: a systematic review and meta-analysis Minerva Endocrinol (Torino) Sooriyaarachchi P Jayawardena R Pavey T King N 4484564920243406073210.23736/S 2724-6507.21.03534-X · doi ↗ · pubmed ↗