Current gynaecological management of women and girls with bleeding disorders in the United Kingdom: A UKHCDO haemophilia treatment centre survey and evaluation of real‐world clinical practice for the British Journal of Haematology
Laura Knox, Imogen Swart‐Rimmer, Naim Rahimi, Callum Harris, Lugain Abdalla, Gary Benson, Clare Brown, Helen Campbell, Ana Carvalhosa, Justin T. Clarke, Sarah Garside, Claire Lentaigne, Jayna Mistry, Priyanka Raheja, Cora Warren, Rezan Abdul‐Kadir, Gill Lowe, Nicola Curry

TL;DR
This study examines gynaecological care for women and girls with bleeding disorders in the UK, highlighting gaps and suggesting improvements for better health outcomes.
Contribution
The study provides a national evaluation of gynaecological care for GWBD and identifies actionable recommendations for improving their treatment.
Findings
Immediate clinical care for heavy menstrual bleeding is adequate, but infrastructure like joint-gynaecology input is lacking.
Direct access to gynaecological services and universal iron testing are recommended to improve care equity.
The study emphasizes the need to address the psycho-social and quality-of-life impacts of heavy menstrual bleeding.
Abstract
Girls and women with bleeding disorders (GWBD) comprise more than half of all registered patients with bleeding disorders in the UK National Haemophilia Database. The gynaecological care of GWBD, until recently, has not been prioritised despite high health burdens, where four of every five patients experience heavy menstrual bleeding (HMB). We report the results of a national survey exploring gynaecological health‐care services offered across haemophilia centres in the United Kingdom, with a focus on HMB. We combine these results with a retrospective cohort analysis of individual patient care records, across a 3‐year period. Of 65 haemophilia centres, 41 responded, covering 90% of the UK GWBD population. Six hundred and ninety‐seven individual patient care records were included, from 13 centres. Our results show that immediate clinical care offered to GWBD experiencing HMB is adequate,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
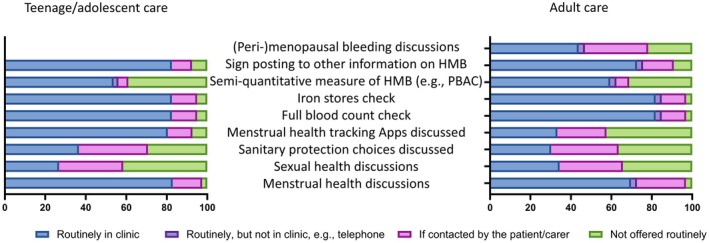 FIGURE 1
FIGURE 1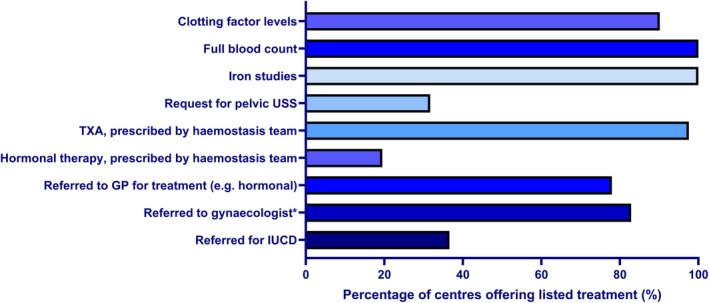 FIGURE 2
FIGURE 2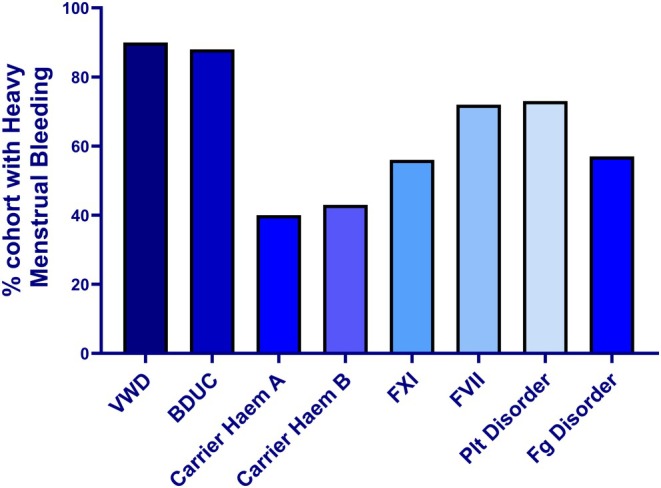 FIGURE 3
FIGURE 3| CCC | HC | |
|---|---|---|
| Number of GWBD | 17 031 | 3229 |
| Number of centres | 29/29 | 12/36 |
| Clinical lead for GWBD | 12/29 | 4/12 |
| Named gynaecology link | 20/29 | 5/12 |
| Joint haematology–gynaecology clinics | 8/29 | 1/12 |
| Centre‐specific gynaecology guidelines | 13/29 | 1/12 |
| PIL covering menstrual health | 20/29 | 4/12 |
| Menarche plan as standard (applicable to fewer CCC/HC) | 5/24 | 1/7 |
| Ongoing review of patients until HMB resolved | 28/29 | 11/12 |
| Gynaecological surgical haemostasis plans written | 28/29 | 12/12 |
| Whole cohort ( | Non‐HMB ( | HMB ( | |
|---|---|---|---|
| ISTH BAT score, median, (IQR) | 5 (IQR 6) | 1 (0–3) | 7 (4–9) |
| BAT score documented, | 376 (54) | 105 (46) | 271 (58) |
| Age at diagnosis, mean, (SD) | 28.9 (9.7) | 29.1 (9.9) | 28.8 (9.6) |
|
| |||
| BDUC | 122 (17.4) | 15 (6.6) | 107 (23) |
| VWD | 78 (11) | 8 (3.5) | 70 (15) |
| Low VWF | 11 (1.6) | 4 (1.8) | 7 (2) |
| Haemophilia A Carrier | 128 (18.4) | 77 (34.0) | 51 (11) |
| Haemophilia B Carrier | 21 (3) | 12 (5.0) | 9 (2) |
| FVII deficiency | 61 (8.7) | 17 (7.5) | 44 (9) |
| FXI deficiency | 80 (11.5) | 35 (15.3) | 45 (10) |
| Platelet dysfunction | 107 (15.3) | 28 (12.3) | 79 (16.8) |
| Disorders of fibrinogen | 46 (9.8) | 20 (8.7) | 26 (6) |
| Acquired Haemophilia or VWD | 3 (<1) | 3 (1.3) | 0 (0) |
| Other single factor deficiencies | 18 (2.6) | 5 (2.2) | 13 (3) |
| Other/combined | 22 (3.1) | 4 (1.8) | 18 (3.8) |
| Centre 1 ( | Centre 2 ( | Centre 3 ( | Centre 4 ( | Centre 5 ( | Centre 6 ( | |
|---|---|---|---|---|---|---|
|
| ||||||
| Mean age at diagnosis, (SD) | 30.6 (7.5) | 31.8 (8.0) | 27.4 (9.9) | 25.6 (11.9) | 31.8 (13.7) | 31.5 (8.7) |
| BAT recorded, | 88 (83.0) | 105 (99.1) | 15 (14.4) | 33 (28.2) | 65 (95.6) | 10 (10.5) |
|
| ||||||
| HMB, | 59 (55.7) | 78 (73.6) | 70 (67.3) | 79 (67.5) | 36 (52.9) | 60 (63.2) |
| Documented to not to have HMB, | 38 (35.8) | 28 (26.4) | 34 (32.7) | 37 (31.6) | 29 (42.6) | 32 (33.7) |
| No documentation about HMB, | 9 (8.5) | 0 (0) | 0 (0) | 1 (0.9) | 3 (4.4) | 3 (3.1) |
|
| ||||||
| Ferritin checked | 38 (64.4) | 48 (61.5) | 40 (57.1) | 21 (26.6) | 36 (100) | 59 (98.3) |
| Iron deficiency confirmed | 17 (44.7) | 25 (52.1) | 22 (55.0) | 12 (57.1) | 23 (63.9) | 12 (20.3) |
| IDA treated | 5 (29.4) | 24 (96.0) | 22 (100) | 7 (58.3) | 18 (78.3) | 8 (75.0) |
| US performed | 21 (35.6) | 23 (29.5) | 23 (32.9) | 17 (14.5) | 21 (58.3) | 20 (33.3) |
| Active gynaecology input | 14 (23.7) | 23 (29.5) | 12 (17.1) | 27 (34.2) | 17 (47.2) | 20 (33.3) |
| HMB treatment plan in place | 19 (32.2) | 29 (37.2) | 59 (84.3) | 42 (53.2) | 28 (77.8) | 40 (66.7) |
|
| ||||||
| Tranexamic acid | 27 (45.8) | 63 (80.7) | 60 (85.7) | 66 (83.5) | 29 (80.6) | 39 (65.0) |
| Hormonal therapy | 26 (44.1) | 55 (70.5) | 29 (41.4) | 35 (44.3) | 21 (58.3) | 35 (58.3) |
| Progesterone IUCD | 9 (15.2) | 33 (42.3) | 17 (24.2) | 17 (21.5) | 5 (13.9) | 24 (40.0) |
| Surgery | 7 (11.9) | 15 (19.2) | 3 (4.3) | 10 (12.7) | 7 (19.4) | 13 (21.7) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemophilia Treatment and Research · Uterine Myomas and Treatments · Platelet Disorders and Treatments
INTRODUCTION
The care of girls and women with inherited bleeding disorders (GWBD), which includes carriers of haemophilia and conditions such as von Willebrand disease (VWD), has historically been less intensive than the management of men and boys with haemophilia.1, 2 Heavy menstrual bleeding (HMB) is the most common symptom experienced by GWBD, affecting more than 80% of individuals.3, 4, 5 It may be the only symptom experienced during adolescence and, across all those affected with HMB, the duration and extent of bleeding are greater for GWBD than for those without a bleeding condition.6 HMB confers significant health, emotional and societal burdens, having the potential to impact all aspects of an individual's life.7 This includes both the physical effects—often relating to iron depletion—as well as the less appreciated effects on quality of life.8, 9, 10
Further to the challenges that an individual with HMB faces personally are the compounding issues that relate to the openness with which discussions around menstrual health are undertaken by clinicians11 and a reluctance by GWBD to seek advice regarding menstrual concerns, worsened both by familial normalisation of what constitutes abnormal/heavy menstrual blood loss12 and the commonly reported feelings of shame when discussing menses.13 To address these issues, a report from the European Haemophilia Consortium (EHC) and the European Association for Haemophilia and Allied Disorders (EAHAD) set out recommendations to prioritise the needs of GWBD.14 Added to this, the UK Haemophilia Centre Director's Organisation (UKHCDO) published their recommendations on the gynaecological care of GWBD.15, 16
In July 2025, the UK Haemophilia Society presented evidence to Parliament summarising their findings from extensive patient and public involvement, highlighting the gaps and inequalities in care for GWBD.17 The most recent UKHCDO annual figures (2023–2024) reported that there were 40 565 patients registered in the United Kingdom with bleeding conditions, of which 21 942 (54%) are GWBD.18 Notably, despite GWBD comprising more than half the patient population, it is only the most recent UK national specification for the management of patients with inherited bleeding disorders where recommendations for gynaecological care of GWBD are described.19 This study aims to describe contemporary practices of care, relating to the gynaecological health of GWBD, both at a centre‐level and patient‐level across the United Kingdom, to highlight variation in practices and provide a benchmark from which clinical services can develop.
METHODS AND MATERIALS
We conducted a project with two arms: (1) a national survey of haemophilia centre‐specific clinical standards of practice and (2) a patient‐specific analysis of GWBD reviewed in clinic appointments across a 36‐month period.
Clinical centre survey
We sent a pre‐piloted survey, using Survey Monkey, to all haemophilia centres in the United Kingdom (e.g. England, Wales, Scotland and Northern Ireland). The full survey can be found in Table S1.
The initial survey request was sent from the UKHCDO management team to the Haemophilia Centre Directors via email, and a reminder was sent 4 weeks later. Following this, personal direct emails were sent to the directors of those centres where no response had been received (both large comprehensive care centres [CCC] and smaller haemophilia centres [HC]).
Individual clinic management case study
We used a cross‐sectional approach to evaluate current practice at the patient level for newly registered GWBD. A pilot was conducted at four centres using a prespecified audit tool (Table S2) with focused data collection based on recommendations set out in the UKHCDO Guideline.15 The study was extended to the remaining UK CCC and HC via an email invitation from the UKHCDO management team. Local audit approval was sought at each site.
Individual case study, whole cohort
Individuals were included via a two‐step process: all females aged 10–55 years, who were menstruating, and registered between 1 January 2021 and 31 December 2024 were eligible. Case notes were screened for reports of HMB, either at diagnosis or during any documented clinical contact from the time of registration across the 36 months. Exclusions were patients diagnosed in the paediatric service or a different geographical region and transferred to a participating adult site to standardise results for each centre. Demographic data were extracted for all included individuals (age, diagnosis, bleeding assessment tool [BAT] score at diagnosis).
HMB group
For those individuals experiencing HMB, further data were collected. Fully anonymised data were sent from participating sites to the study team for analysis. Data from the largest centres were directly compared to further evaluate clinical variability.
Data analysis
Statistical analyses were performed on GraphPad Prism (v10.3.1) or SPSS (v31). Normality was assessed using visual histogram assessment and the Shapiro–Wilk test. Results were represented by mean ± SD/median ± interquartile range (IQR), comparisons made using t‐tests or Mann–Whitney, as appropriate. ANOVA was chosen to compare results across the six larger centres (Table 3) with binomial logistic regression to further interrogate results. Significance was set at p < 0.05.
RESULTS
Survey
Online questionnaires were distributed to 65 centres, including 29 CCC and 36 HC. Of the CCC, seven treated adults alone, seven children (age 0–18 years) alone and 15 treated patients across their lifespan. Responses were received from all (n = 29, 100%) CCC and 33% (n = 12) of the HCs. Ten of the included HCs treated adults and children, two adults only. The 41 centres covered 89.8% of the UK patient population with an inherited bleeding disorder (male and female) and specifically 92.3% of registered GWBD.
Of the 41 centres, many (n = 23, 56%) did not have a dedicated clinical lead (haemophilia specialist nurse or doctor) for GWBD and most did not have access to joint gynaecology–haematology clinics (n = 32, 78%). Despite this, two‐thirds of respondents had a named gynaecology link with whom patient care could be directly discussed. Only one in three (14/41) centres had a local guideline that offered recommendations on the gynaecological care of GWBD. Of these 14 centres, all 14 detailed how to manage acute onset HMB; 13/14 covered longer term management; 10/14 covered education around menstrual health and management of the menarche; and 11/14 covered the management of gynaecological surgery/procedures. Of 41 centres, 39 reported that formal surgical haemostatic management plans were provided.
Across the 41 respondents, 28 centres routinely reviewed all GWBD in their clinics (68%), 10 centres saw patients only if they had low factor levels and two offered patient‐initiated follow‐up. These percentages did not differ between CCC and HC. Just over half of all respondents (n = 22, 55%) provided a patient information leaflet (PIL) on menstrual health, with varying responses as to whether these were centre‐specific, age‐specific or accessed via external services such as the Haemophilia Society (Table 1). All but one centre proactively asked patients about menstrual health during a clinic appointment, and the remaining centre discussed menstruation if the patient asked about their periods.
Age‐specific stages of life
73% (n = 30) centres provide care for GWBD in the pre‐menarche stage and all offer education to patients about HMB, with 94% also educating the family/carers. Notably, fewer centres educated the patient and/or family about what constitutes a normal menstrual cycle (70% and 61.3% respectively). One in four centres discussed how to manage menarche with the patient and/or checked iron stores pre‐menarche. Half of centres checked haemoglobin at this life stage.
At the time of menarche, one in five centres (20%) uses a written menarche plan as standard for all GWBD, which includes haemophilia clinical team contacts for the patient, in case of need. 45% of centres routinely ask about menarche in clinic but do not actively offer an individualised haemostasis plan. One centre confirmed that the GP manages the menarche.
Post‐menarche the care offered to young adults/teenagers does not differ from adult care (Figure 1). The fewest positive responses across both age groups related to discussions around the impact of a bleeding disorder on sexual health; the breadth of sanitary protection choices available and how to monitor menstrual flow to flag times of concern. Peri‐menopausal menstrual health was also an area infrequently discussed.
Day‐to‐day management of GWBD and their gynaecological health in the clinic setting, teenage versus adult populations. Forty‐one centres provided answers about adolescent care, since all centres cover this ‘cross‐over’ age range. Thirty‐three centres responded about adult care only. These histograms show the overall percentage of responses to each question, according to whether the response was fully affirmative (dark blue); partially affirmative (purple); conditionally affirmative (pink); or refuted (green). Data relating to teenage/adolescent care are shown in the left, and for adult care, it is shown in the right. One additional question was asked regarding the care of adults—relating to the (peri‐)menopausal life stage. HMB, heavy menstrual bleeding; PBAC, pictorial bleeding assessment chart.
HMB was monitored by a variety of methods at 32 centres (78%). In 26 centres, a mix of the ISTH BAT20 and/or patient discussions were used, and in six centres, the PBAC was used. No centre used a questionnaire, such as the SAMANTA, which has been designed for menstrual health.21 95% of centres follow a GWBD experiencing HMB until the symptoms have resolved, and most of these centres provide that care directly although, in six cases, the joint haematology–gynaecology clinic offers this service. Two centres direct the individuals to the GP for routine HMB care.
Biomarker measurements were evaluated commonly: most centres routinely offering a full blood count and iron status check (n = 40, 98%). (Iron studies were defined as a measurement which included some or all of ferritin, transferrin saturations, total iron binding capacity and serum iron levels.) 63% (n = 26) reported that they would repeat iron studies in a previously iron deplete/anaemic patient. In more routine settings, outside HMB, 49% (n = 20) centres would check iron status at the time of diagnosis of an inherited bleeding condition; 29% would check at every clinic for menstruating females; 41% during pregnancy and 34% after delivery.
Clinicians reported that they would refer a patient to gynaecology or their joint haematology–gynaecology clinic: 11/41 routinely referred when HMB is diagnosed (Figure 2); 24/41 referred only if first‐line therapy failed, for example, when HMB persisted after the use of a single agent tranexamic acid or hormonal therapy; five centres referred for patients to discuss insertion of a Mirena coil or other intrauterine system (IUS); five centres referred when HMB was impacting quality of life; five referred to exclude/investigate structural causes; and seven centres referred for the management of ongoing iron depletion.
*Immediate management by haemophilia treating teams when a patient presents with HMB, not requiring hospital admission. The histogram shows percentages of the total number of respondents (n = 41) answering that their centre's standard practice involves each listed management strategy. ‘referred to gynaecologist’ included 25 centres specifying referral to gynaecology clinic and an additional nine centres referring to a joint haematology–gynaecology clinic. GP, general practitioner; IUCD, intrauterine contraceptive device; TXA, tranexamic acid; USS, ultrasound scan.
Individual case study
Seven hundred and twenty‐seven patients were identified at 13 centres (11 CCC, 2 HC) with a newly registered bleeding disorder between 1 January 2021 and 31 December 2024. Thirty individuals had moved centre and were deemed ineligible. In total, 697 patients were included. The mean age at diagnosis was 28.9 years (SD: 9.7), range: 8–55 years. Two hundred and twenty‐eight individuals (32.7%) did not experience HMB, and 469 (67.3%) did experience HMB. There was no difference between those without or with HMB; mean—29.1 years (SD 9.9), range 8–50 years, versus 28.8 years (SD 9.6), range 8–55 years, respectively, p = 0.73 (Table 2). As previously described, we found a variable likelihood of individuals experiencing HMB, according to their bleeding disorder diagnosis. Our data confirm a preponderance of HMB in those with VWD, bleeding disorder of unknown cause (BDUC), platelet disorders and FVII deficiency (Figure 3).
Percentage of GWBD experiencing HMB, according to their registered inherited bleeding disorder type. BDUC, bleeding disorder of unknown cause; F, factor; Fg, fibrinogen; VWD, von Willebrand disease.
HMB group
91% of the HMB cohort (n = 428/469) had a documented full blood count. Only 64.7% had a documented ferritin (n = 302). Two‐fifths of the overall HMB cohort (n = 180), or more pertinently, 59.2% of those tested with a ferritin, had confirmed iron deficiency (e.g. ferritin <30 μg/L), 144 of whom were on iron replacement (either IV or PO). Thirty‐six iron‐deficient patients (20%) did not have evidence of iron being prescribed. Just over one‐third (36.7%) had evidence of a pelvic US having been requested—although in one‐third of this group (n = 55/172), there was no documentation to confirm whether this had occurred. 12% were planned for, or had been investigated with, a hysteroscopic procedure.
UKHCDO recommendations are that a menstrual plan be in place for all GWBD who menstruate. 65% (n = 166) did have one. Furthermore, 75% of the HMB cohort had documentation outlining the use of tranexamic acid (TXA) for treatment. The UKHCDO guideline recommends TXA as a first‐line treatment for women trying to conceive or when hormonal therapies are not acceptable. TXA is also recommended in combination with hormonal therapies to improve treatment efficacy. Oral hormonal therapy was discussed with 58% (n = 258/469); discussions around IUS were documented for 29% of individuals. Only one‐third of patients had active gynaecological involvement. One in five individuals was directed to educational patient information on menstrual care, either using centre‐specific leaflets or leaflets from the Haemophilia Society. Most had no documented discussion around possible surgical management options (70%, n = 308). Moreover, importantly, 9% (n = 42) of individuals had an unscheduled hospital attendance (e.g. visit to the emergency department) for HMB symptoms.
Documentation detailing the social impact of HMB was poor: 50 individuals (10%) were noted to have absences from school or work, and in two‐thirds of notes, there was no documentation as to whether this impact of HMB had been explored. 20% (n = 93) of the group reported fatigue, but again half (n = 206) of individuals were not asked about this symptom.
Centre‐specific variation
Finally, we explored individual centre differences, with a focus on HMB prevalence and evaluation of iron deficiency. We compared six large centres (e.g. returning >65 patient entries), Table 3. Prevalence of HMB varied (53–73%). Logistic regression analysis confirmed that the bleeding condition diagnosis conferred the strongest influence on this difference (p < 0.001) rather than a difference between centres. Clinical practices for checking iron status were highly variable, with between one‐quarter and 100% of individuals having their iron levels checked. For those with a ferritin showing iron depletion/deficiency, variability in treatment was evident, and in two centres, fewer than two in three iron‐deficient patients received therapy.
DISCUSSION
Equity of access to, and the provision of, high quality care is a central tenet of good healthcare. However, the impact of HMB despite its universality, and the management of gynaecological health more broadly for GWBD, has not been prioritised. In the last few years, these health inequalities have become more prominent.22 This descriptive analysis was conducted in recognition of these inequalities and to better understand contemporary clinical care offered across the United Kingdom to highlight areas for harmonisation and improvement.
The number of respondents to our survey was high, with all 29 CCC responding, covering more than 90% of registered patients. As such, our data are highly representative of the care offered across the United Kingdom. The results confirm that just over half of the centres lack a clinical lead focused on women's health, only one‐third of centres have local guidance to direct clinical care, and only one in five centres have joint clinics. These results are less favourable than those from a European survey, where twice as many centres offered joint gynaecology clinics and had local management algorithms for all aspects of gynaecological care.23 These differences may, in part, reflect inclusion bias in the European survey (40% response rate), whereas our data included all CCC, or it may more broadly reflect country‐specific differences.
There was evidence of good practice in some aspects of care for GWBD. Education around HMB was universally offered at the pre‐menarche life stage, and similarly, all centres discussed HMB across all age groups. Added to this, most centres offered a standard approach to HMB diagnosis—with blood tests, an anti‐fibrinolytic medication, and then—generally—referral to start hormonal control methods. The individual clinical case study confirmed this common approach. Interestingly, within the near 700‐strong patient number evaluated, only two‐thirds were documented to have HMB—a figure that is considerably lower than other publications.3, 4, 5 This may represent poor clinical capture of HMB and/or may reflect that many publications report survey results, which can suffer reporting bias.
There were, however, large variations in the longer term management of HMB. Notably, few patients were managed with active gynaecological input (32%). Greater communication and joint working, with cross‐fertilisation of best practices between specialities, would improve the confidence of haematologists to manage HMB and could have a rapid beneficial impact on patient care. Nevertheless, there are barriers to joint working, including consultant time, access to funding to set up services and a variability of prioritisation between hospitals which would need to be addressed to support adoption of these clinics.24, 25
Our patient partner stressed the importance of joint haematology–gynaecology care and that excessive bleeding during perimenopause and bleeding relating to sex should be proactively addressed in consultations. Furthermore, clinicians should go further to support requests by patients for reasonable adjustments at work for HMB to facilitate ongoing employment.
In resource‐rich countries, HMB is one of the most common causes of iron deficiency.26 Our data highlight opportunities to improve screening for iron depletion in our at‐risk patients. Iron loss is associated with significant health burden, further compounded by societal and economic costs. The impact of absenteeism annually in the United Kingdom from HMB is £4.7 billion.27 These data highlight the urgent need for routine clinical practices, around detection and monitoring of iron deficiency, to change.28 The authors advocate annual monitoring of iron status for all GWBD who are menstruating.
There are limitations to our data. Although 90% of the registered UK GWBD were included in the centre‐specific survey, we were unable to include all HCs. Survey data can be skewed, according to the individual and the patient mix of the centre where the questionnaire is completed. Notably, only 11% of the audit cohort were diagnosed with VWD, which is unexpectedly low, given that in the United Kingdom, each year, approximately 25% of newly registered females have VWD. Our clinical audit data reflected the answers provided in the survey, which was reassuring. We did not collect ethnicity or socioeconomic data (including the impact of period poverty on patients), which would have been of particular interest given several inherited bleeding disorders have a higher prevalence in ethnic minority populations. We did not ask if written material was provided in patients' first spoken language. ISTH BAT score reporting29 varied significantly between centres, making the results for this criterion less broadly applicable.
CONCLUSION
Our comprehensive national survey shows that clinical care offered to GWBD experiencing HMB is adequate, with much room for improvement. Areas for immediate prioritisation include greater access to gynaecological services; universal, routine testing of iron status; and more broadly, a shift towards clinical practices that recognise and address the impact HMB has on patients' psycho‐social, sexual and quality of life.
AUTHOR CONTRIBUTIONS
Laura Knox, Imogen Swart‐Rimmer, Naim Rahimi, Callum Harris, and Lugain Abdalla designed the audit of practice, piloted and completed the audit; Gill Lowe and Nicola Curry supported the audit project, reviewed and analysed audit data. Gary Benson, Ana Carvalhosa, Justin T. Clarke, Sarah Garside, Claire Lentaigne, Priyanka Raheja, Cora Warren, Rezan Abdul‐Kadir, Gill Lowe, and Nicola Curry designed the survey of clinical centres. Nicola Curry collated and analysed the data; Nicola Curry and Laura Knox wrote the first draft of the manuscript. All authors reviewed and updated the manuscript.
FUNDING INFORMATION
The author(s) received no financial support for the research, authorship and/or publication of this article.
CONFLICT OF INTEREST STATEMENT
The authors declare no competing financial interests in relation to this manuscript.
ETHICS STATEMENT
Formal ethics were not required for the national survey, and all participating sites followed local approval practices prior to undertaking the audit.
Supporting information
Table S1.
Table S2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Weyand AC , James PD . Sexism in the management of bleeding disorders. Res Pract Thromb Haemost. 2020;5(1):51–54.33537529 10.1002/rth 2.12468 PMC 7845070 · doi ↗ · pubmed ↗
- 2Hermans C , Johnsen JM , Curry N . Women and girls with inherited bleeding disorders: focus on haemophilia carriers and heavy menstrual bleeding. Haemophilia. 2024;30(Suppl 3):45–51.38532560 10.1111/hae.14983 · doi ↗ · pubmed ↗
- 3Djambas KC , Gouider E , von Mackenen S , Kadir RA . Heavy menstrual bleeding in women with inherited bleeding disorders. Haemophilia. 2020;26(Suppl 3):16–19.32356352 10.1111/hae.13888 · doi ↗ · pubmed ↗
- 4Du P , Bergamasco A , Moride Y , Truong Berthoz F , Özen G , Tzivelekis S . Von Willebrand disease epidemiology, burden of illness and management: a systematic review. J Blood Med. 2023;14:189–208.36891166 10.2147/JBM.S 389241 PMC 9987238 · doi ↗ · pubmed ↗
- 5Maas DPMSM , Saes JL , Blijlevens NMA , Cnossen MH , den Exter PL , van der Heijden OWH , et al. High prevalence of heavy menstrual bleeding in women with rare bleeding disorders in The Netherlands: retrospective data from the R Bi N study. J Thromb Haemost. 2023;21(10):2726–2734.37517479 10.1016/j.jtha.2023.07.014 · doi ↗ · pubmed ↗
- 6Kadir RA , Economides DL , Sabin CA , Pollard D , Lee CA . Assessment of menstrual blood loss and gynaecological problems in patients with inherited bleeding disorders. Haemophilia. 1999;5(1):40–48.10215946 10.1046/j.1365-2516.1999.00285.x · doi ↗ · pubmed ↗
- 7NICE . Heavy menstrual bleeding: assessment and management, NG 88. London: National Institute for Health and Care Excellence; 2021 a [cited 2025 May 15]. Available from: http://www.nice.org.uk 29634173 · pubmed ↗
- 8Schoep ME , Adang EMM , Maas JWM , De Bie B , Aarts JWM , Nieboer TE . Productivity loss due to menstruation‐related symptoms: a nationwide cross‐sectional survey among 32 748 women. BMJ Open. 2019;9:e 026186.10.1136/bmjopen-2018-026186 PMC 659763431248919 · doi ↗ · pubmed ↗