Ruptured Ovarian Endometrioma During Pregnancy: A Case Report and Review Highlighting Clinically Occult Risk Factors
Yumiko Miyazaki, Sakurako Takada, Rena Yamazaki, Shinya Hirabuki, Hiromasa Sasaki

TL;DR
This case report and review explore ovarian endometrioma rupture during pregnancy, focusing on risk factors like cyst size and adhesions.
Contribution
The study highlights clinically occult risk factors, such as intra-abdominal adhesions, in endometrioma rupture during pregnancy.
Findings
78.5% of cases involved cysts ≥6 cm, indicating large size as a major risk factor.
50% of ruptures occurred in the third trimester, with all cases ≥32 weeks delivered via cesarean.
Intra-abdominal adhesions were reported in seven cases, suggesting a possible occult risk.
Abstract
The rupture of an ovarian endometrioma during pregnancy is a rare cause of acute abdominal pain, and its underlying risk factors are incompletely understood. We report a case of ovarian endometrioma rupture during pregnancy complicated by dense intra-abdominal adhesions and review previously reported cases to clarify potential risk factors. Twenty cases, including our case, were analyzed. Among cases with available data, 78.5% involved cysts measuring ≥6 cm, consistent with previous reports identifying large cyst size as a major risk factor. Adhesions were reported in seven cases, although most studies did not explicitly comment on their presence or absence. Regarding gestational age, 50% of cases occurred during the third trimester, and all cases presenting at ≥32 weeks of gestation were delivered by cesarean section. Beyond visible risk factors, such as cyst size and gestational age,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
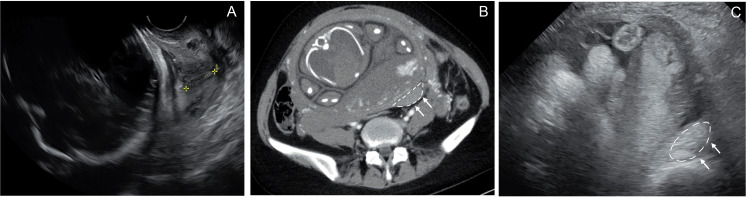 Figure 1
Figure 1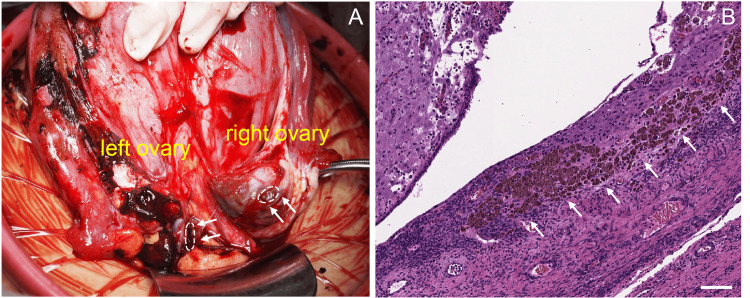 Figure 2
Figure 2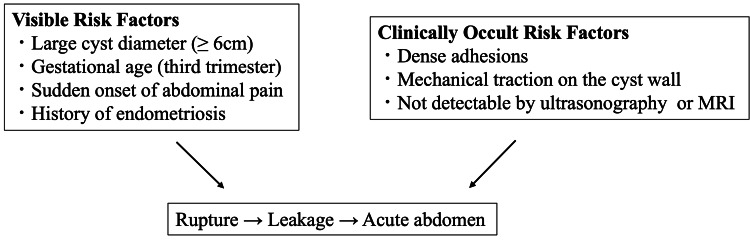 Figure 3
Figure 3| Parameter | Value | Reference range |
| WBC (/μL) | 12,700 | 3300–8600 |
| Hb (g/μL) | 10.8 | 11.6–14.8 |
| PLT (×103/μL) | 350 | 158–348 |
| T-Bil (mg/dL) | 0.4 | 0.4–1.5 |
| AST (U/L) | 16 | 13–30 |
| ALT (U/L) | 10 | 7–23 |
| CK (U/L) | 25 | 41–153 |
| BUN (mg/dL) | 5.0 | 8–20 |
| Cre (mg/dL) | 0.43 | 0.46–0.79 |
| Amylase (U/L) | 130 | 44–132 |
| CRP (g/dL) | 0.16 | 0–0.14 |
| Authors | Age (years) | Gravida | Para | Mode of conception | History of endometriosis | Gestational age (weeks) | Presenting symptoms | Preoperative diagnosis |
| Brill et al. [ | 38 | 3 | 2 | NR | NR | NR (term) | Abdominal pain | Placental abruption |
| Steinberg [ | 35 | 1 | 0 | S | No | 38 | Abdominal pain | Ruptured ovarian cyst |
| Anderson and Edmond [ | 39 | 2 | 1 | NR | No | 37 | Abdominal pain | NR |
| Rossman et al. [ | 25 | 2 | 0 | NR | NR | 30 | Abdominal pain with hyperpyrexia | Ruptured appendix |
| Johnson and Woodruff [ | 39 | NR | NR | NR | NR | 26 | Lower abdominal pain | Degeneration of uterine fibroid |
| Vercellini et al. [ | 29 | 1 | 0 | S | No | 35 | Abdominal pain | Bowel obstruction |
| Barbazan et al. [ | 29 | 1 | 0 | NR | No | 18 | Lower abdominal pain with nausea and vomiting | NR |
| García-Velasco et al. [ | 25 | NR | 0 | S | No | 9 | Lower abdominal pain | Hemorrhagic corpus luteum or endometrioma |
| Loh et al. [ | 25 | NR | NR | S | NR | 6 | Lower abdominal pain | Ectopic pregnancy |
| Gregora and Higgs [ | 44 | 2 | 0 | S | Yes | 18 | Lower abdominal pain | NR |
| Ueda et al. [ | 35 | NR | NR | ART | NR | NR (second trimester) | NR | NR |
| Reif et al. [ | 25 | NR | 0 | ART | Yes | 27 | Abdominal pain | NR |
| Yu et al. [ | NR | NR | NR | NR | NR | 35 | Abdominal pain | NR |
| Takami et al. [ | 30 | 1 | 0 | ART | Yes | 10 | Abdominal pain | Peritonitis |
| Takami et al. [ | 31 | 3 | 0 | NR | NR | 31 | Abdominal pain | Ruptured endometrioma |
| Takami et al. [ | 32 | 1 | 0 | NR | NR | 32 | Abdominal pain with vomiting | Acute appendicitis |
| Takami et al. [ | 34 | 2 | 1 | NR | Yes | Postpartum | Abdominal pain | Ruptured endometrioma |
| Yamamoto et al. [ | 39 | 1 | 0 | AIH | Yes | 27 | Abdominal pain | Ruptured endometrioma |
| Tanabe et al. [ | 43 | 3 | 1 | NR | Yes | 36 | Abdominal pain | Placental abruption |
| Present case | 39 | 2 | 1 | S | No | 33 | Upper abdominal pain | SHiP |
| Authors | Side | Cyst size (cm) | Enlargement during pregnancy (cm) | Initial management | Surgical approach | Procedure | Adhesions | Gestational age at delivery (weeks) | Mode of delivery |
|
Brill et al. [ | Bilateral ovaries | NR | NR | Surgical | CS | Hysterectomy and bilateral salpingo-oophorectomy | NR | NR | Emergency CS |
|
Steinberg [ | Left ovary | 6 | NR | Surgical | CS | Cystectomy | Yes | 38 | Emergency CS |
|
Anderson and Edmond [ | Left ovary | NR | NR | Surgical | CS | Left oophorectomy | NR | 37 | Emergency CS |
|
Rossman et al. [ | Bilateral ovaries (side not specified) | NR | NR | Conservative | Laparotomy | Bilateral cystectomy | Yes | 30 | Vaginal |
|
Johnson and Woodruff [ | Right ovary | NR | NR | NR | CS | Cesarean section | NR | 27 | CS (type not specified) |
|
Vercellini et al. [ | Right ovary | 8 | NR | Surgical | CS | Cyst enucleation and adhesiolysis | Yes | 35 | Emergency CS |
|
Barbazan et al. [ | Right ovary | 6 | NR | Surgical | Laparotomy | Right oophorectomy | Yes | NR | NR |
|
García-Velasco et al. [ | Left ovary | 8.3 | 6→8.3 | Surgical | Laparotomy | Left salpingo-oophorectomy | Yes | NR | NR |
|
Loh et al. [ | Bilateral ovaries (left ruptured) | 4 (left), 5 (right) | NR | Surgical | Laparoscopy | Bilateral cystectomy | Yes | 39 | NR |
|
Gregora and Higgs [ | Bilateral ovaries (left ruptured) | 6 (left), 2.8 (right) | NR | Surgical | Laparotomy | Opening the cyst and stripping the cyst wall | NR | 41 | Vaginal |
|
Ueda et al. [ | Ovary (side not specified) | 6 | 5→6 | NR | Laparotomy | Peritoneal lavage and drainage | NR | NR | NR |
|
Reif et al. [ | Left ovary | NR | NR | Surgical | CS | Left salpingectomy and partial ovariectomy | Yes | 27 | Emergency CS |
|
Yu et al. [ | Right ovary | 6 | NR | Surgical | CS | Cystectomy | NR | 35 | Emergency CS |
|
Takami et al. [ | Left ovary | 4 | NR | Conservative | Laparotomy | Cystectomy, appendectomy, and drainage | NR | 41 | Vaginal |
|
Takami et al. [ | NR | 5 | NR | Surgical | Laparotomy | Abdominal drainage | NR | 40 | Vaginal |
|
Takami et al. [ | Right ovary | 7 | 6→7 | Surgical | CS | Cyst aspiration, cauterization, and appendectomy | NR | 32 | Emergency CS |
|
Takami et al. [ | Left ovary | 10.5 | 9→10.5 | Conservative | Laparotomy | Drainage and cystectomy | NR | 41 | Vaginal |
|
Yamamoto et al. [ | Right ovary | 6.8 | 5→6.8 | Conservative | CS | Cesarean section and cystectomy | NR | 37 | Elective CS |
|
Tanabe et al. [ | Left ovary | 7 | NR | Conservative | CS | Cystectomy | NR | 36 | Emergency CS |
| Present case | Bilateral ovaries | NR | NR | Surgical | CS | Cystectomy | Yes | 33 | Emergency CS |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometriosis Research and Treatment · Intestinal and Peritoneal Adhesions · Ovarian cancer diagnosis and treatment
Introduction
The rupture of an ovarian endometrioma during pregnancy is a rare but potentially serious cause of acute abdominal pain. Although ovarian endometriomas are common in women of reproductive age, rupture during pregnancy is uncommon, with only sporadic reports of such cases in the literature [1,2]. Symptoms are often nonspecific, and the differential diagnosis includes adnexal torsion, hemorrhagic cyst rupture, appendicitis, and other causes of acute abdominal pain during pregnancy [3]. Spontaneous hemoperitoneum in pregnancy (SHiP) is another rare cause of acute abdomen during pregnancy, reported in association with endometriosis-related vascular disruption [4], and should be considered in the differential diagnosis. Accordingly, the preoperative diagnosis of ovarian endometrioma rupture remains challenging in many cases.
Previous case reports have primarily focused on clinically identifiable risk factors such as cyst size and gestational age [1,3]. However, less attention has been paid to factors that are difficult to evaluate preoperatively, such as intra-abdominal adhesions [1,3,5].
We present a case of ovarian endometrioma rupture during pregnancy complicated by dense intra-abdominal adhesions and provide a review of previously reported cases. The objective of this study was to explore both clinically apparent and occult risk factors contributing to ovarian endometrioma rupture during pregnancy.
Case presentation
Our patient was a 39-year-old woman, gravida 2, para 1, with no notable medical history. She had never been diagnosed with endometriosis. She conceived spontaneously and visited a local clinic at 16 weeks of gestation. However, she did not receive regular antenatal care and was referred to our institution for perinatal management at 30 weeks of gestation. No ovarian enlargement was apparent at the initial visit.
The patient developed sudden-onset, persistent upper abdominal pain at 33 weeks and 2 days of gestation. The pain did not resolve, and she was therefore transported to the emergency department. Upon admission, her vital signs were stable, with a body temperature of 37.2 °C, blood pressure of 114/73 mmHg, heart rate of 84 beats/min, and oxygen saturation of 98% on room air. Abdominal examination revealed tenderness in the right upper quadrant. Obstetric assessment revealed a reassuring fetal heart rate pattern with irregular uterine contractions. Vaginal examination showed a closed cervix without evidence of vaginal bleeding or rupture of membranes.
Laboratory investigations revealed a white blood cell count of 12,900/μL, a C-reactive protein level of 0.16 mg/dL, and a hemoglobin level of 10.9 g/dL (Table 1). Transvaginal ultrasonography demonstrated a shortened cervix of 18 mm (Figure 1A). Transabdominal ultrasonography revealed a hematoma posterior to the uterus (Figure 1B). Contrast-enhanced computed tomography revealed hemorrhagic ascites and a hematoma posterior to the left side of the uterus (Figure 1C). Based on these findings, the patient was diagnosed with spontaneous hemoperitoneum in pregnancy (SHiP).
Ultrasonographic and computed tomographic findings of ruptured ovarian endometrioma during pregnancy.(A) Transvaginal ultrasonography revealed cervical shortening.(B) Transabdominal ultrasonography image showing a hematoma posterior to the uterus. The bleeding site is indicated by dotted lines and arrows.(C) Contrast-enhanced abdominal computed tomography image showing a high-density area posterior to the uterus, suggestive of a hematoma (indicated by dotted lines and arrows).
The patient was treated with acetaminophen and pentazocine; however, her abdominal pain worsened. Follow-up transabdominal ultrasonography revealed an increase in intra-abdominal fluid volume, prompting an emergency cesarean section with hemostatic surgery.
Hemorrhagic ascites were observed intraoperatively in the abdominal cavity. A female infant weighing 2016 g was delivered by cesarean section, with Appearance, Pulse, Grimace, Activity, and Respiration (APGAR) scores of 8 and 9 at 1 and 5 min, respectively [6]. The umbilical arterial pH was 7.21. Both ovaries contained endometriomas, and ruptured cysts with spilled contents were observed bilaterally (Figure 2A). The ovaries were densely and bilaterally adherent to the posterior uterine wall. Bilateral ovarian cystectomy was performed, followed by hemostasis and extensive peritoneal lavage. The estimated blood loss was 610 mL. Histopathological examination confirmed bilateral ovarian endometriomas (Figure 2B).
Intraoperative and histopathological findings of ruptured ovarian endometrioma.(A) Intraoperative findings showing bilateral ovarian endometriomas with cyst rupture on both sides (dotted lines and arrowheads indicate rupture sites).(B) The cyst wall was lined with endometrial tissue and showed hemosiderin deposition (indicated by arrows), and the endometrial stroma exhibited decidual-like changes. Scale Bar: 100 μm.
The patient’s abdominal pain resolved after surgery, and inflammatory marker levels gradually normalized. The postoperative course was uneventful, and she was discharged on day 6 after the operation. The neonate was admitted to the neonatal intensive care unit and discharged on day 29. This study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent for publication of this report was obtained from the patient.
Discussion
The rupture of an ovarian endometrioma during pregnancy is a rare but clinically serious cause of acute abdominal pain [3,7]. The risk factors for and mechanisms underlying ovarian endometrioma rupture are not fully understood owing to the rarity of the condition. Management strategies are mainly based on case reports and small case series. We present a case of ruptured ovarian endometrioma complicated by dense intra-abdominal adhesions, along with a review of 19 previously reported cases, summarized in Tables 2, 3, to explore both visible and clinically occult risk factors for rupture. Cases of SHiP without documented rupture of an ovarian endometrioma were excluded from this review because vascular disruption-related hemorrhage represents a distinct clinical entity that differs in pathophysiology and clinical course.
Currently, no consensus has been reached on the cyst size for which surgical intervention is recommended prior to pregnancy to prevent rupture during gestation. In our review, the mean maternal age was 33.4 years, and 68.7% of the patients were nulliparous (Table 2). Cysts measuring ≥ 6 cm accounted for 78.5% of the cases with available data in this review (Table 3), which is consistent with findings from reports identifying larger cysts as a visible risk factor for rupture during pregnancy [20]. Gestational age may also play a critical role in cyst rupture [3]. In our review, 50% of the cases occurred during the third trimester (Table 2), and all cases presenting at or beyond 32 weeks of gestation were managed with cesarean section. These findings suggest that progressive uterine enlargement in late pregnancy restricts the operative field, necessitating cesarean section to enable treatment of ovarian endometrioma rupture (Table 3). However, immediate delivery is not always mandatory; reports include a case at 31 weeks that reached term following surgical drainage alone [1] and another at 27 weeks that was successfully managed conservatively with analgesics [2]. These findings emphasize the need for individualized management strategies tailored to gestational age, clinical severity, and the overall condition of both mother and fetus.
In contrast to the amount of information available on tumor size and gestational age as risk factors, limited information exists on intra-abdominal adhesions in ovarian endometrioma. Adhesions were explicitly described in seven cases, including the present case (Table 2); however, most reports did not mention the presence or absence of adhesions. Adhesions in such cases may be underreported in the literature because they are often difficult to detect or underestimated on routine preoperative imaging. However, several studies have suggested an association between adhesions and ovarian endometrioma rupture [1,3,5]. In our case, dense adhesions severely restricted ovarian mobility, resulting in localized mechanical stress on the cyst wall (Figure 2A). This mechanical stress or traction may have increased wall tension and predisposed the endometrioma to rupture, even without marked cyst enlargement. These observations suggest that adhesions are a clinically occult risk factor for endometrioma rupture during pregnancy.
In this case, intra-abdominal fluid accumulation was observed preoperatively, raising suspicion of SHiP. SHiP may be associated with hypovolemic shock due to massive hemorrhage [4]. In contrast, rupture of an ovarian endometrioma does not necessarily result in severe bleeding. Therefore, the temporal progression of vital signs, perioperative findings, and the presence or absence of anemia may aid in differentiating between these two conditions. The proposed role of adhesions in endometrioma rupture is consistent with the pathophysiology of SHiP, in which deep infiltrating endometriosis-related fibrosis and adhesions are thought to induce traction-related vascular rupture during pregnancy [4,5]. Although decidualization has also been suggested to play a role in the development of SHiP [4], the relationship between decidualization and the enlargement or rupture of endometrioma remains largely unclear. While SHiP primarily involves vascular disruption rather than cyst wall rupture, both conditions may share a common mechanism through which anatomical pregnancy-related changes affect pre-existing endometriotic adhesions.
Our review highlights the difficulty in achieving an accurate preoperative diagnosis of ruptured ovarian endometrioma, with only 35.7% of cases correctly identified prior to surgery. Ruptured endometrioma should be considered in the differential diagnosis of acute abdominal pain during pregnancy given the nonspecific clinical presentation and limitations of prenatal imaging, particularly in patients with known or suspected endometriomas.
Both visible and clinically occult risk factors should be considered when managing ovarian endometriomas during pregnancy (Figure 3). Early assessment for ovarian endometriomas may facilitate diagnosis. In select patients with large cysts and suspected adhesions, surgical intervention before pregnancy could reduce rupture-related complications.
Conceptual framework of risk factors associated with ovarian endometrioma rupture during pregnancy. This schematic diagram summarizes the visible and clinically occult risk factors for ovarian endometrioma rupture during pregnancy based on the findings in this review. This figure illustrates a conceptual framework and does not imply definitive causal relationships.
This review is limited by the heterogeneity of the included case reports and the frequent absence of standardized or complete clinical data, which precludes robust quantitative analysis and necessitates cautious interpretation of the findings. Adhesions could not be objectively graded, and reporting bias cannot be excluded. However, highlighting adhesions as a clinically occult risk factor for ovarian endometrioma rupture provides a novel perspective for guiding the diagnosis and management of future cases and research.
Conclusions
The rupture of an ovarian endometrioma during pregnancy is a rare but serious cause of acute abdominal pain. In addition to visible risk factors, such as cyst size and gestational age, clinically occult factors, such as intra-abdominal adhesions, may contribute to the risk of ovarian endometrioma rupture. Careful and early assessment and documentation of ovarian endometriomas may support clinical decision-making in these cases; however, the role of surgical intervention before pregnancy in preventing ovarian endometrioma rupture requires further investigation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Characteristics of ovarian endometrioma during pregnancy J Obstet Gynaecol Res Takami M Kajiyama R Miyagi E Aoki S 325032564720213415573710.1111/jog.14862 · doi ↗ · pubmed ↗
- 2A case of ruptured decidualized ovarian endometrioma: usefulness of serial MRI for determining adequate management Case Rep Obstet Gynecol Yamamoto S Kikuchi T Fujii H 3234784202220223595922610.1155/2022/3234784 PMC 9357808 · doi ↗ · pubmed ↗
- 3A systematic review on endometriosis during pregnancy: diagnosis, misdiagnosis, complications and outcomes Hum Reprod Update Leone Roberti Maggiore U Ferrero S Mangili G 701032220162645060910.1093/humupd/dmv 045 · doi ↗ · pubmed ↗
- 4Endometriosis and spontaneous hemoperitoneum in pregnancy: evaluation of the magnitude of the risk in women becoming pregnant via in vitro fertilization Fertil Steril Benaglia L Reschini M La Vecchia I Candotti G Somigliana E Vercellini P 1023102811520213327263210.1016/j.fertnstert.2020.10.030 · doi ↗ · pubmed ↗
- 5Beyond infertility: obstetrical and postpartum complications associated with endometriosis and adenomyosis Fertil Steril Vigano P Corti L Berlanda N 80281210420152634827410.1016/j.fertnstert.2015.08.030 · doi ↗ · pubmed ↗
- 6Evaluation of the newborn infant; second report J Am Med Assoc APV HODA JALS WEIM BEC 1985198816819581359863510.1001/jama.1958.03000150027007 · doi ↗ · pubmed ↗
- 7Rupture of endometriotic ovarian cyst causes acute hemoperitoneum in twin pregnancy Fertil Steril Reif P Schöll W Klaritsch P Lang U 2125212395201110.1016/j.fertnstert.2011.01.02321315338 · doi ↗ · pubmed ↗
- 8Intrapartum rupture of bilateral ovarian endometrial cysts: case report Am J Obstet Gynecol Brill HM Kaplan S Rapoport L 2002017319571338181310.1016/s 0002-9378(16)37282-9 · doi ↗ · pubmed ↗