Expanding the donor pool: Outcomes of liver transplantation using grafts with ≥50% macrosteatosis
Kasra Shirini, Shani S. Kamberi, Srinivasan Muthukrishnan, Omar Alattar, Ruchin Patel, Francheska Nieves, Massimo Arcerito, Josue Alvarez-Casas, Saad Malik, Kirti Shetty, Daniel G. Maluf, Chandra Bhati, Raphael P.H. Meier

TL;DR
This study shows that liver transplants using fatty donor livers can be successful, though they come with some risks.
Contribution
The study demonstrates the viability of using high-macrosteatosis liver grafts in low-to-intermediate MELD recipients.
Findings
All five patients survived beyond one year with functioning grafts.
Two patients experienced thrombotic complications requiring reoperations.
Abstract
Liver grafts with over 50% macrosteatosis are often deemed marginal, but organ shortages necessitate exploring their use. We conducted five transplants with deceased donor grafts containing 50%–90% macrosteatosis, ensuring donor age <55 years, CIT ≤6 hours, and recipient laboratory MELD score ≤30. Two patients required reoperations due to thrombotic complications (acute HAT and PVT), and hospital stay ranged from 6 to 26 days. All patients survived beyond one year with functioning grafts. These findings suggest the feasibility of using high-macrosteatosis grafts in intermediate- to low-laboratory-MELD recipients, albeit with potential thrombotic risks.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
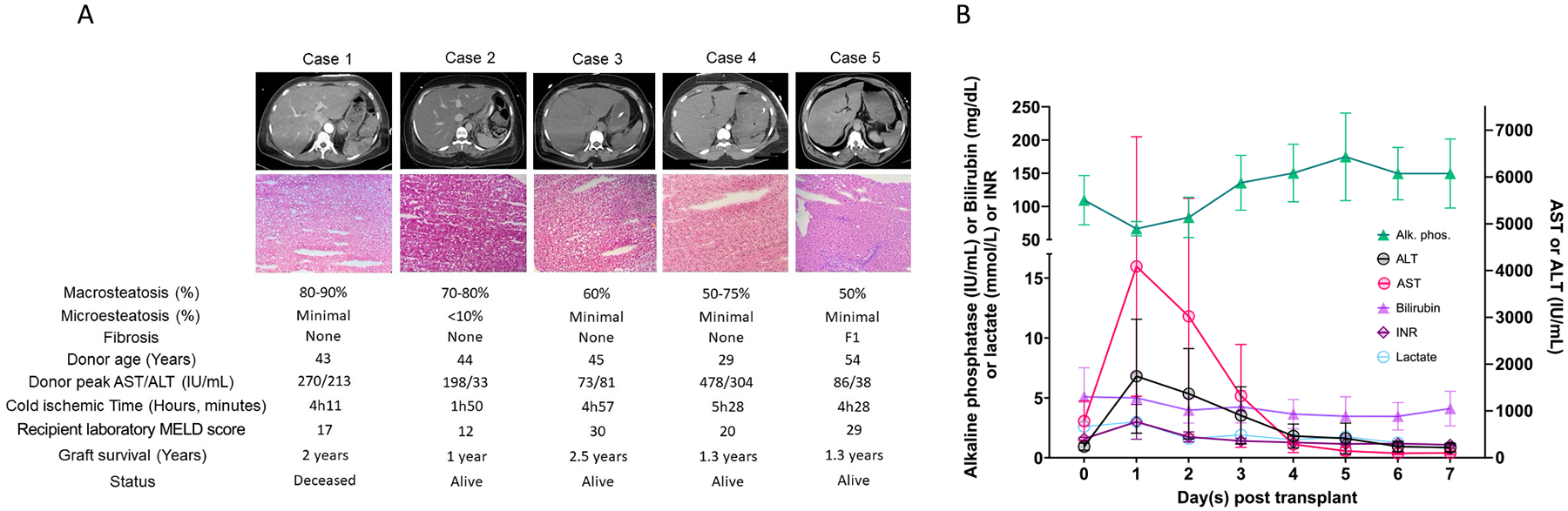 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrgan Transplantation Techniques and Outcomes · Hepatocellular Carcinoma Treatment and Prognosis · Liver Disease and Transplantation
Introduction
Metabolic dysfunction–associated fatty liver disease (MAFLD) impacts up to 50 % of the global population, contributing to a growing pool of steatotic liver grafts [1]. Donor livers with ≥50 % macrosteatosis are often considered marginal grafts, with ≥55 % discarded despite evidence showing acceptable long-term outcomes when appropriately selected and managed [2]. While moderate macrosteatosis (30–60 %) is associated with higher early mortality due to complications such as postreperfusion syndrome, cardiac arrest, and acute kidney injury, it does not significantly affect long-term survival, with 5- and 10-year outcomes comparable to non-steatotic grafts [3]. Steatotic grafts remain a valuable resource when managed with optimized protocols. We hypothesized that strict recipient-donor selection criteria could enable the successful transplantation of high macrosteatosis (≥50 %) livers into low-risk recipients. We present five cases demonstrating this approach and achieving acceptable post-transplantation outcomes. Eligible liver grafts were defined by ≥50 % macrosteatosis in cases of young brain death donors (ideally age<55), peak AST/ALT ≤500/350, projected cold ischemia time ≤6 h, and recipients with laboratory MELD scores ≤30. Graft steatosis was quantified on hematoxylin and eosin frozen sections by an independent liver pathologist and confirmed by our own liver pathologist. Median with range is presented. This study was conducted in accordance with the Declaration of Helsinki and approved by the University of Maryland, Baltimore Institutional Review Board (protocol HP-00,113,760). All recipients provided informed consent.
Description of cases
Recipients
Five patients underwent transplantation following our protocol (Fig. 1.A). The median recipient age was 61 (40 – 72) years, with a BMI of 27.1 (19.9 – 30.8) kg/m^2^ (Table 1). Laboratory MELD scores ranged from 12 to 30, with a median of 20. Two cases had laboratory MELD scores of 29 and 30, stable hemodynamics, preserved renal function, and no signs of infection. The primary indications for transplantation included cirrhosis due to chronic hepatitis C associated with hepatocellular carcinoma (HCC) in just one case, metabolic dysfunction-associated steatohepatitis (MASH) (2 cases), and alcohol-associated liver disease (ALD) (2 cases). No macrovascular tumor thrombus was detected on preoperative imaging or biopsy. None of the other recipients had a history of HCC. All patients underwent comprehensive preoperative assessments, including abdominal CT imaging and liver biopsies, to confirm the underlying pathology and evaluate transplant candidacy.
Donors
The donors had an average age of 43 ± 9 years and a mean BMI of 35.1 ± 3.1 kg/m^2^. macrosteatosis levels averaged 66.5 ± 13.6 % (range: 50–90 %), with minimal microsteatosis (<10 %) in all cases. Fibrosis was limited to F1 in one donor liver, with no significant fibrosis in the others. Causes of donor death included anoxia (3 cases), cerebrovascular stroke (1 case), and meningoencephalitis (1 case). Donor liver enzymes showed peak AST/ALT values of 198 (73 – 478) IU/L and 81 (33 – 304) IU/L, respectively, with terminal values of 53 (17 – 276) IU/L and 33 (28 – 110) IU/L. The median cold ischemia time (CIT) was 4h28, ranging from 1h50 to 5h28.
Operation details
During transplantation, vascular anastomoses were completed in a median of 39 (36 – 55) minutes. Estimated blood loss was 2.5 (2 – 12) L, with patients receiving a median of 6 RBC units. One case of severe reperfusion injury was observed in case 1. This patient was relisted and placed on MARS but ultimately did not need a retransplant and fully recovered.
Postoperative outcomes
Postoperative liver function tests showed peak AST and ALT levels of 2425 (571 – 15,000) IU/L and 400 (297 – 6559) IU/L, respectively, normalized within four days (Fig. 1.B). Two patients developed prothrombotic complications: one case of portal vein thrombosis (PVT), and one case of hepatic artery thrombosis both managed surgically. Additionally, two patients required reoperations due to biliary leakage.
Follow-up and survival
The median hospital stay was 11 days, ranging from 6 to 26 days. Median follow-up was 476 (396 – 920) days. The 2-year graft survival rate was 100 %, with four patients alive and maintaining well-functioning grafts at the end of the follow-up. One patient passed away after two years due to HCC recurrence.
Discussion
We demonstrate the feasibility of transplanting macrosteatosis liver allografts (≥50 %) with acceptable long-term outcomes, conditional on a careful donor-recipient selection. Our protocol prioritized low-risk recipients with low laboratory MELD scores, short CIT, and young donors with low AST/ALT values, aligning with prior studies showing that meticulous graft selection reduces early dysfunction risks [2].
Low laboratory MELD scores, young donor age, and short CIT are crucial for successful steatotic graft transplantation. In our series, two patients with laboratory MELD scores of 29 and 30 were included. The absence of aggravating risk factors such as severe renal dysfunction, severe portal hypertension, or systemic infection allowed us to proceed with these cases. Kaltenbach et al. evidenced that macrosteatosis over 40 % raises short-term risks but not long-term outcomes within high-risk subgroups [4]. A 2025 multicenter study found that steatotic grafts in liver transplantation for HCC were associated with worse disease-free survival and overall survival compared to non-steatotic grafts, particularly with longer cold ischemia times (≥6 h), higher donor BMI (≥40 kg/m^2^), and recipients with non-alcoholic fatty liver disease, included in the HAML score [5]. Of note, none of our recipients had any of these risk factors.
Our recipients showed high post-transplant AST/ALT peak levels, indicating significant Ischemia-reperfusion injury (IRI). Considering this, we prioritized donors with moderately elevated AST/ALT values to minimize the double hit. Notably, sequential biopsy studies have demonstrated that moderate macrosteatosis (30–60 %) often resolves rapidly post-transplant, with complete regression observed within one week and sustained at six months. This supports our observation that steatosis may not persist long-term if recipients overcome the early perioperative risks [6].
Steatotic liver grafts are particularly vulnerable to IRI due to increased mitochondrial oxidative stress, impaired ATP-restoration, and heightened inflammatory responses [7]. Despite these challenges, satisfactory outcomes were achieved without machine perfusion. These findings align with broader reviews of marginal grafts, which emphasize that steatotic livers—along with elderly and DCD grafts [8–10]—can expand the donor pool when paired with optimized donor–recipient matching and preservation strategies [11]. Ex vivo hypothermic and normothermic machine perfusion (NMP) is increasingly used in the U.S. to reduce IRI, improve graft survival, and mitigate biliary complications [12,13]. We did not have access to machine perfusion at that time; however, it is likely that the liver grafts we describe here would have benefited from being pumped and further assessed. So-called ‘defatting protocols’ offer further potential for optimizing extreme steatotic grafts [14]. These protocols leverage pharmacological agents such as forskolin (NKH477), L-carnitine, and insulin-like growth factor-1 (IGF-1) to reduce triglyceride content and restore mitochondrial function [15]. Recent studies have shown that ‘defatting protocols’ during NMP can reduce fat content by up to 40 % in severely steatotic livers, enhancing graft viability and expanding the donor pool [15]. While promising, clinical evidence remains limited; further studies are needed to validate their safety and efficacy.
Our case series underscores the feasibility of utilizing severely macrosteatotic grafts, encouraging their broader acceptance in carefully selected recipients. Stringent postoperative monitoring is crucial for the early detection of early allograft dysfunction (EAD) and primary non-function. Various parameters and scoring systems can be used to closely monitor the recipient of a severely steatotic liver graft [16,17].
Vascular complications were notable in our study, with one patient developing hepatic artery thrombosis and another experiencing PVT, both managed successfully. One may hypothesize that the cytokine storm following steatotic graft implantation might favor prothrombotic conditions, possibly compounded by ischemia–reperfusion injury and endothelial dysfunction. These complications contributed to extended hospital stays and which highlights the need for careful perioperative management. While no consensus exists on prophylactic anti-coagulation, its selective use in high-risk cases, such as those with prior PVT or complex anastomoses, hypercoagulable states, warrants further consideration.
Our report is limited by its small sample size, variability in sampling and histologic steatosis evaluation, lack of a control group, and medium-term follow-up. These limitations underscore that our findings should be regarded as descriptive and primarily hypothesis-generating. Future multicenter studies are needed to validate findings, evaluate the recurrence of hepatic steatosis or progression to NASH, and assess the utilization of steatotic grafts in the setting of advanced preservation techniques. ‘Defatting protocols’ combined with machine perfusion could optimize the utilization rate of steatotic grafts.
In conclusion, transplanting macrosteatosis liver grafts in selected recipients is feasible. Despite important limitations such as small sample size, lack of a control group, and variability in histologic evaluation, our findings suggest that, with strict selection criteria, these grafts can expand the donor pool while maintaining excellent liver transplantation outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wong VW, Ekstedt M, Wong GL, Hagström H. Changing epidemiology, global trends and implications for outcomes of NAFLD (in eng) J Hepatol Sep 2023;79(3): 842–52. 10.1016/j.jhep.2023.04.036. · doi ↗
- 2Kwong AJ, Impact of donor liver macrovesicular steatosis on deceased donor yield and posttransplant outcome (in eng) Transplantation Feb 1 2023;107(2): 405–9. 10.1097/tp.0000000000004291.36042548 PMC 9877102 · doi ↗ · pubmed ↗
- 3Altshuler PJ, Evaluating outcomes related to donor and recipient metabolic environment: macrosteatotic allografts and nonalcoholic steatohepatitis (in eng) Liver Transpl Apr 2022;28(4):623–35. 10.1002/lt.26313. · doi ↗
- 4Kaltenbach MG, Harhay MO, Abt PL, Goldberg DS. Trends in deceased donor liver enzymes prior to transplant: the impact on graft selection and outcomes (in eng) Am J Transpl Jan 2020;20(1):213–9. 10.1111/ajt.15573. · doi ↗
- 5Wang K, Outcomes and risk factors for liver transplantation using steatotic grafts for hepatocellular carcinoma: a multicenter study (in eng) Eur J Surg Oncol Aug 2025;51(8):110061. 10.1016/j.ejso.2025.110061.40288219 · doi ↗ · pubmed ↗
- 6Croome KP, Livingston D, Croome S, Keaveny AP, Taner CB, Nakhleh R. Sequential protocol biopsies post-liver transplant from donors with moderate macrosteatosis: what happens to the fat? (in eng) Liver Transpl Feb 2021;27(2):248–56. 10.1002/lt.25867. · doi ↗
- 7Abbas SH, Ceresa CDL, Pollok JM. Steatotic donor transplant livers: preservation strategies to mitigate against ischaemia-reperfusion injury (in eng) Int J Mol Sci 2024;25(9). 10.3390/ijms 25094648. Apr 24. · doi ↗
- 8Meier RPH, Kelly Y, Yamaguchi S, Braun HJ, Lunow-Luke T, Adelmann D, Niemann C, Maluf DG, Dietch ZC, Stock PG, Kang SM, Feng S, Posselt AM, Gardner JM, Syed SM, Hirose R, Freise CE, Ascher NL, Roberts JP, Roll GR. Advantages and Limitations of Clinical Scores for Donation After Circulatory Death Liver Transplantation. Front Surg 2022. 10.3389/fsurg.2021.808733. · doi ↗