Incidental Right Hilar Metallic Density After Implantable Cardioverter Defibrillator Placement in a Tracheostomized Woman: Suspected Airway Foreign Body With Concurrent Pleural Effusion
Michael J Martinez, Hardik Jain, Neeraj Goindani, Ahmed Bux, Anusha Gupta, Tanya Zagoruychenko

TL;DR
An 80-year-old woman had a tracheostomy cleaning brush accidentally lodged in her airway, which was detected and removed using bronchoscopy.
Contribution
Highlights the risk of tracheostomy-care equipment as a source of iatrogenic foreign bodies in adults.
Findings
A radiopaque density on chest imaging was confirmed as a tracheostomy cleaning brush in the right bronchus intermedius.
Flexible bronchoscopy successfully retrieved the foreign body without complications.
The case emphasizes the importance of correlating imaging with clinical stability and pursuing definitive evaluation when suspicion remains.
Abstract
Adult tracheobronchial foreign bodies are uncommon and can be subtle on radiographs, particularly in device-rich environments. An 80-year-old woman with severe heart failure underwent elective implantable cardioverter defibrillator (ICD) placement and had a linear right hilar radiopaque density and right basilar atelectasis/pleural effusion on postoperative portable chest radiography. She was stable on a tracheostomy collar without respiratory distress. Given the appearance and history of home tracheostomy care, a tracheostomy cleaning brush was suspected. Flexible bronchoscopy via the tracheostomy confirmed and retrieved a cleaning brush from the right bronchus intermedius; purulent secretions were irrigated, and there were no complications. The patient remained hemodynamically stable post-procedure. This case illustrates the value of correlating imaging with clinical stability yet…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1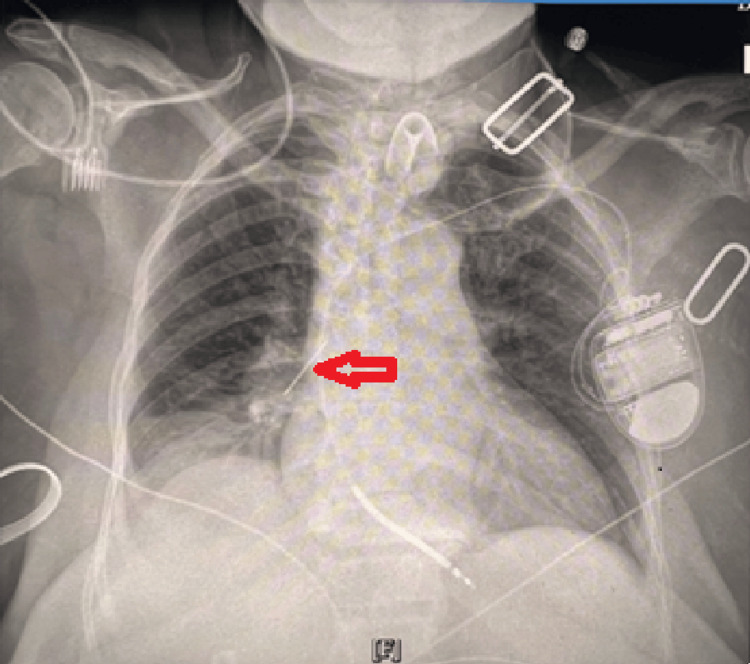 Figure 2
Figure 2| Medication | Dosage | Frequency | Route |
| Carvedilol | 3.125 mg | BID | PO/GT |
| Sacubitril/Valsartan | 24-26 mg | BID | PO/GT |
| Spironolactone | 12.5 mg | Daily | PO/GT |
| Furosemide | 20 mg | Daily | PO/GT |
| Dapagliflozin | 10 mg | Daily | PO/GT |
| Acetylcysteine | 200 mg/mL | Q4H | Nebulizer |
| Sodium chloride | 0.90% | Q4H | Nebulizer |
| Omeprazole | 20 mg | Daily | PO/GT |
| Polyethylene glycol | 17 g | Daily | PO/GT |
| Multivitamin | 1 tab | Daily | PO/GT |
| Vitamin B-12 | 1000 mcg | Daily | PO/GT |
| Ibuprofen | 400 mg | PRN | PO/GT |
| Nystatin | 100,000 U/g | BID | Topical |
| Parameter | Result | Reference range and units |
| Hemoglobin | 10.5 | 12-15.5 g/dL |
| Hematocrit | 31 | 36-46 % |
| WBC count | 4.2 | 4.0-10.5 ×103/µL |
| Platelets | 239–263 | 150-400 ×103/µL |
| Sodium | 141 | 135-145 mmol/L |
| Potassium | 3.6 | 3.5-5.0 mmol/L |
| Bicarbonate (HCO₃) | 30 | 22-28 mmol/L |
| BUN | 8.6 | 7-20 mg/dL |
| Creatinine | 0.5 | 0.6-1.3 mg/dL |
| AST | 21 | 10-40 U/L |
| ALT | 12 | 7-56 U/L |
| Albumin | 4.7 | 3.5-5.0 g/dL |
| INR | 1.05 | 0.9-1.1 |
| Glucose (POC) | 168 | 70-140 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Tracheal and airway disorders · Trauma Management and Diagnosis
Introduction
Foreign body aspiration in adults is less common than in children and may present insidiously; bronchoscopy remains the diagnostic and therapeutic standard [1,2]. Cleaning brushes and other tracheostomy components are known to be iatrogenic foreign bodies in adults and are frequently radiopaque, allowing for radiographic detection and bronchoscopic removal [3,4]. However, radiographic identification is complicated in perioperative and ICU settings. Portable radiographs are prone to artifacts from monitoring leads and external devices that can mimic endobronchial material; careful device mapping and cross-sectional correlation help avoid misinterpretation [5]. Furthermore, foreign bodies may be radiolucent, though metallic iatrogenic objects are exceptions [6,7].
In complex cases, unilateral pleural effusions may coexist with atelectasis or aspiration. Guideline-based evaluation incorporates imaging and, when indicated, diagnostic thoracentesis to clarify etiology [8]. Interpreting pleural fluid results further guides management, including when to apply laboratory criteria during thoracentesis [9,10]. Computed tomography can help differentiate pleural effusion from parenchymal opacity and clarify confusing projections [11,12]. This case illustrates the value of correlating imaging with clinical stability yet proceeding to definitive airway evaluation when suspicion persists.
Case presentation
An 80-year-old woman with hypertension, hyperlipidemia, type 2 diabetes (HbA1c 6.4% four months prior), obesity (BMI 31.2), chronic systolic heart failure (left ventricular ejection fraction or LVEF 30-35% with dilated inferior vena cava (IVC) and trace pericardial effusion), tracheostomy collar, and percutaneous endoscopic gastrostomy (PEG) tube presented on July 7, 2025 for elective implantable cardioverter defibrillator (ICD) implantation. Additional history included a recent left parietal convexity subdural hematoma and C1 vertebral fractures status post laminectomy. The ICD procedure was uncomplicated with an appropriate right ventricular lead position.
She was afebrile and hemodynamically stable post-procedure (blood pressure 158/82 → 151/87 mmHg (normal value: <120/80 mmHg); heart rate 70-82 bpm (normal values: 60-100 bpm); respiratory rate 18-20 breaths/min (normal values: 12-20 breaths/min); temperature 36.2-37.1 °C (normal values: 36.5°C-37.3°C); SpO₂ 97-100% (normal values: 95-100%) on tracheostomy collar ~35% FiO₂); comfortable, and without dyspnea or chest pain.
Medications
The patient's medications and their dosing frequency are outlined in Table 1.
Exam
Alert and oriented; trach collar in place; no respiratory distress; lungs with normal breath sounds; regular cardiac rhythm without murmurs; soft, nondistended abdomen; no leg edema.
Laboratory data
The results of the laboratory parameters are given in Table 2.
Cardiac testing
Twelve-lead ECG (performed on July 7, 2025) showed normal sinus rhythm (77 bpm) with nonspecific T-wave changes (PR 186 ms, QRS 76 ms, QTc 441 ms) (Figure 1).
Twelve-lead ECG demonstrating normal sinus rhythm with nonspecific T-wave abnormalitiesHeart rate 77 bpm; PR 186 ms; QRS 76 ms; QTc 441 ms.
Imaging
Portable AP chest radiograph (performed on August 7, 2025) showed a left-sided ICD generator with transvenous lead to the right ventricle, a thin linear radiopaque density projected over the right pulmonary hilum (also present during an earlier chest radiograph taken shortly after the patient's admission but prior to the elective ICD placement), right basilar atelectasis with interval improvement, and a right pleural effusion. The left lung was clear (Figure 2).
Portable AP chest radiograph showing left-sided ICD generator and right ventricular leadICD: Implantable cardioverter defibrillator; A thin linear radiopaque density projects over the right hilum, with right basilar atelectasis and a small right pleural effusion.
Additional history
The patient’s daughter reported that a swivel tracheostomy cleaning brush had been used at home by a visiting nurse approximately two weeks before admission [13]. This history and the radiographic appearance increased concern for an intraluminal foreign body.
Procedure
On October 7, 2025, the thoracic surgery team performed flexible fiberoptic bronchoscopy through the existing tracheostomy site while the patient was under general anesthesia. The patient was categorized as American Society of Anesthesiologists (ASA) Physical Status Classification Class 3 [13], indicating a patient with severe systemic disease. A shoulder roll was used for neck extension. After timeout, a foreign body was visualized in the right bronchus intermedius. A snare was passed through the bronchoscope, the object was captured, and because it could not be fully withdrawn into the tracheostomy tube, the trach tube was removed. The foreign body was extracted and the trach was replaced easily. Bronchoscopy was repeated; purulent secretions were suctioned and the airway irrigated with sterile saline. No bleeding occurred. Estimated blood loss was minimal; intake recorded was lactated Ringer’s 50 mL and propofol 3 mL (total 53 mL).
The patient was transported to the post-anesthesia care unit (PACU) hemodynamically stable and a postoperative chest radiograph was ordered. The specimen (“foreign body right bronchus intermedius”) was sent to surgical pathology. It was wound class: IV [14]. There were no intraoperative complications. The operating room personnel were present per record and names have been omitted for privacy.
Outcome
The patient remained stable after bronchoscopy with no immediate complications.
Discussion
Evaluation of suspected adult airway foreign bodies should begin by correlating imaging with clinical stability. While many aspirated foreign bodies are radiolucent, making diagnosis challenging [6], iatrogenic objects such as tracheostomy brushes are often metallic and radiopaque [3,4]. In this case, the portable chest radiograph revealed a linear density. Portable films in device-rich environments can be misleading because ECG leads, compression devices, and external hardware may project over the hilum [5]. While a two-view chest radiograph or computed tomography (CT) can clarify confusing projections and differentiate artifacts from true airway material [7,11,12], clinical judgment in this case prioritized immediate intervention. Given the patient’s clear history of home tracheostomy brush use and the distinct metallic appearance of the density, the team opted to bypass additional radiation and proceed directly to bronchoscopy, which serves as both the diagnostic gold standard and the therapeutic solution [1,2].
Iatrogenic foreign bodies constitute a meaningful subset of adult cases. Published reports specifically describe aspiration of tracheostomy components that appear as thin metallic lines on radiographs [3,4]. The daughter’s history provided a plausible mechanism and highlights the importance of standardized tracheostomy care education [15]. Finally, pleural effusion and basilar atelectasis can coexist with foreign bodies. In this patient, the effusion was likely multifactorial (heart failure history and post-operative status) rather than solely a direct sequela of the foreign body, but its presence necessitated careful evaluation [8-10].
Conclusions
The right perihilar radiopaque density in this tracheostomized patient was not an artifact. Flexible bronchoscopy via the tracheostomy retrieved a tracheostomy cleaning brush from the right bronchus intermedius, with no complications and clinical stability post-removal. This case demonstrates that equivocal portable chest radiographs in device-rich settings should still prompt definitive airway evaluation when suspicion persists. CT may assist with localization, but bronchoscopy provides both diagnosis and therapy. Recognizing tracheostomy-care equipment as a potential iatrogenic foreign body can prevent delays and procedure-related complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tracheobronchial foreign bodies in adults Ann Intern Med Limper AH Prakash UB 6046091121990232767810.7326/0003-4819-112-8-604 · doi ↗ · pubmed ↗
- 2Foreign body aspiration in adult airways: therapeutic approach J Thorac Dis Hewlett JC Rickman OB Lentz RJ Prakash UB Maldonado F 33983409920172922132510.21037/jtd.2017.06.137PMC 5708401 · doi ↗ · pubmed ↗
- 3Tracheobronchial aspiration of a tracheostomy tube cleaning brush in a laryngectomized patient Turk Arch Otorhinolaryngol Ünsal N Kaya A Yaşar M Özcanİ Bayram A 1611636320254046264310.4274/tao.2025.2025-2-6PMC 12480997 · doi ↗ · pubmed ↗
- 4Accidental foreign body aspiration through tracheostomy inlet; 26 cases Arch Iran Med Eliçora A Sezer HF Abdullayev G AvcıA Topçu S 308313252022 https://pubmed.ncbi.nlm.nih.gov/35943006/3594300610.34172/aim.2022.50PMC 11904291 · doi ↗ · pubmed ↗
- 5Portable chest radiography: must-know findings and mimics Radiographics Strickland LR Henry TS Mc Adams HP Tailor TD O'Sullivan-Murphy B Heyneman LE 043202310.1148/rg.22013237651275 · doi ↗ · pubmed ↗
- 6Risk factors associated with radiolucent foreign body inhalation in adults: a 10-year retrospective cohort study Respir Res Liu X Ni F Guo T 2382320223608831810.1186/s 12931-022-02165-9PMC 9463778 · doi ↗ · pubmed ↗
- 7Detectability of foreign body materials using X-ray, computed tomography and magnetic resonance imaging: a phantom study Eur J Radiol Voss JO Doll C Raguse JD 10950513520213342182810.1016/j.ejrad.2020.109505 · doi ↗ · pubmed ↗
- 8British Thoracic Society guideline for pleural disease Thorax Roberts ME Rahman NM Maskell NA 114311567820233755315710.1136/thorax-2023-220304 · doi ↗ · pubmed ↗